Das könnte Ihnen auch gefallen
- A Simplified ECG GuideDokument4 SeitenA Simplified ECG Guidejalan_z96% (26)
- ECG ReviewDokument146 SeitenECG ReviewThea DinoNoch keine Bewertungen
- Answer Diagnosis: 1. RhythmDokument2 SeitenAnswer Diagnosis: 1. RhythmSuggula Vamsi KrishnaNoch keine Bewertungen
- Free Medical ECG Interpretation PresentationsDokument30 SeitenFree Medical ECG Interpretation PresentationsRohini SelvarajahNoch keine Bewertungen
- BBB EcgDokument33 SeitenBBB EcgLokbre YoasNoch keine Bewertungen
- Cardiac Pacing: Terms You Will Become Familiar With in This Section of TheDokument21 SeitenCardiac Pacing: Terms You Will Become Familiar With in This Section of TheClt Miskeen100% (1)
- EKG Interpretation NursingDokument14 SeitenEKG Interpretation NursingTanya ViarsNoch keine Bewertungen
- 10 Steps To Learn ECG InterpretationDokument5 Seiten10 Steps To Learn ECG InterpretationMohammadNoch keine Bewertungen
- HEENT Cheat SheetDokument22 SeitenHEENT Cheat SheetKatrina FeriNoch keine Bewertungen
- ECG WorldDokument139 SeitenECG WorldsatyaNoch keine Bewertungen
- Dr. Adeel Ahmed Waheed: House Officer M-4Dokument84 SeitenDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNoch keine Bewertungen
- The 12-Lead EKG: A Step-by-Step GuideDokument31 SeitenThe 12-Lead EKG: A Step-by-Step GuideJay JiangNoch keine Bewertungen
- Right Side EcgDokument4 SeitenRight Side EcgDragos CirsteaNoch keine Bewertungen
- Disorders of The BoneDokument2 SeitenDisorders of The BoneRPh Krishna Chandra JagritNoch keine Bewertungen
- EkgDokument67 SeitenEkgFendi Rafif Dad'sNoch keine Bewertungen
- ECG InterpretationDokument73 SeitenECG Interpretationsultan khabeebNoch keine Bewertungen
- ECG Learning ModulesDokument150 SeitenECG Learning ModulesdodiNoch keine Bewertungen
- Waves and Intervals Heart Activity Normal/Abnormal (1 Small Box 0.04sec) (1 Big (5 Small) 0.2sec)Dokument6 SeitenWaves and Intervals Heart Activity Normal/Abnormal (1 Small Box 0.04sec) (1 Big (5 Small) 0.2sec)Eben Ezar Dela CruzNoch keine Bewertungen
- Cardiology Consult Manual 2018 PDFDokument450 SeitenCardiology Consult Manual 2018 PDFmepimplolabotellas100% (2)
- Jesse Felts PGY2, Not A CardiologistDokument43 SeitenJesse Felts PGY2, Not A Cardiologistイオン天国Noch keine Bewertungen
- Medical Mnemonic BookletDokument14 SeitenMedical Mnemonic Bookletahmed abd elazizNoch keine Bewertungen
- ECG Interpretation TheoryDokument4 SeitenECG Interpretation TheorySteph PiperNoch keine Bewertungen
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDokument88 SeitenAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNoch keine Bewertungen
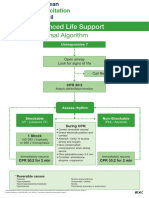
- Advanced Life Support - A0 PDFDokument1 SeiteAdvanced Life Support - A0 PDFiulia-uroNoch keine Bewertungen
- Ekg Panum or OsceDokument69 SeitenEkg Panum or OsceGladish RindraNoch keine Bewertungen
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDokument64 SeitenAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7Noch keine Bewertungen
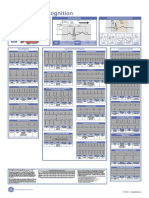
- Poster1 Arrhythmia Recognition e PDFDokument1 SeitePoster1 Arrhythmia Recognition e PDFPierf-17Noch keine Bewertungen
- ECG Flashcards: Atrial ArrhythmiasDokument27 SeitenECG Flashcards: Atrial ArrhythmiasDima HabanjarNoch keine Bewertungen
- EKG - Assignment Without AnswersDokument10 SeitenEKG - Assignment Without AnswersJon Millhollon100% (1)
- Electrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramDokument29 SeitenElectrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramMihaela PrisacaruNoch keine Bewertungen
- JVP Guide: Assessing Jugular Venous Pulse Waves and PressureDokument53 SeitenJVP Guide: Assessing Jugular Venous Pulse Waves and PressureJoshua JayakaranNoch keine Bewertungen
- Basics of Pacing CombinedDokument54 SeitenBasics of Pacing CombinedMichael Susanto100% (1)
- Fundamentals of ECGDokument112 SeitenFundamentals of ECGadithya polavarapu100% (1)
- Poster1 Arrhythmia Recognition e PDFDokument1 SeitePoster1 Arrhythmia Recognition e PDFMiko RamosoNoch keine Bewertungen
- Cardiology 2020Dokument113 SeitenCardiology 2020Fatima ShoukatNoch keine Bewertungen
- Avnrt VS AvrtDokument79 SeitenAvnrt VS AvrtDwi Nugroho PrastowoNoch keine Bewertungen
- Dysrhytmia NotesDokument11 SeitenDysrhytmia NoteshannahhwolfNoch keine Bewertungen
- Cardiac ArrhythmiasDokument11 SeitenCardiac ArrhythmiasChino Paolo SamsonNoch keine Bewertungen
- Clinical History of Chest PainDokument59 SeitenClinical History of Chest PainBelalNoch keine Bewertungen
- Paediatric Emergencies NotesDokument6 SeitenPaediatric Emergencies NotesJana AldourNoch keine Bewertungen
- Bio Accoustic 131203Dokument10 SeitenBio Accoustic 131203Choirun Nisa Nur AiniNoch keine Bewertungen
- Heart Blood HistoDokument53 SeitenHeart Blood HistoAnonymous 52lBinNoch keine Bewertungen
- Atrial FlutterDokument16 SeitenAtrial Flutterapi-527603714100% (1)
- Ecg Pathology 02Dokument95 SeitenEcg Pathology 02Andi MP Manurung100% (1)
- SVTDokument8 SeitenSVTJulieNoch keine Bewertungen
- Anatomy of The Lung & Mechanics of VentilationDokument1 SeiteAnatomy of The Lung & Mechanics of Ventilationphileo182Noch keine Bewertungen
- Canada Airspace - TP6010BDokument2 SeitenCanada Airspace - TP6010BWilliam RiosNoch keine Bewertungen
- Classification of MurmursDokument2 SeitenClassification of MurmursNazneen SiddiquiNoch keine Bewertungen
- Ekg Full BibleDokument6 SeitenEkg Full BibleTJNoch keine Bewertungen
- Cardiovascular Nursing: Study Online atDokument7 SeitenCardiovascular Nursing: Study Online atLilly DayeNoch keine Bewertungen
- 10 Steps To Learn ECG InterpretationDokument5 Seiten10 Steps To Learn ECG InterpretationIbrahem Y. NajjarNoch keine Bewertungen
- Understanding ECG and Cardiac PhysiologyDokument99 SeitenUnderstanding ECG and Cardiac Physiologysahar awaisNoch keine Bewertungen
- ELECTROCARDIOGRAM by Aldrin Jayson AlmadenDokument23 SeitenELECTROCARDIOGRAM by Aldrin Jayson AlmadenItsMe AJNoch keine Bewertungen
- EAR First AidDokument4 SeitenEAR First Aidr_lakshmi2722Noch keine Bewertungen
- ECG Interpretation in One PageDokument2 SeitenECG Interpretation in One PageRyan AycockNoch keine Bewertungen
- Elementsandprinciples Poster2Dokument1 SeiteElementsandprinciples Poster2api-310282544Noch keine Bewertungen
- Renal DR - Najeeb Word To Word.Dokument71 SeitenRenal DR - Najeeb Word To Word.Aleeza KhanNoch keine Bewertungen
- ECG Online Course GuideDokument44 SeitenECG Online Course GuideShobana RaveendranNoch keine Bewertungen
- The Cardiac Cycle: Chapter 19Dokument62 SeitenThe Cardiac Cycle: Chapter 19BishwambherNoch keine Bewertungen
- A Simplified ECG GuideDokument4 SeitenA Simplified ECG GuideMarian Ioan-LucianNoch keine Bewertungen
- VQ - O2 GradientDokument27 SeitenVQ - O2 GradientIkbal NurNoch keine Bewertungen
- Me 1Dokument74 SeitenMe 1Shaz ChindhyNoch keine Bewertungen
- 1 The Electrical Activity of The HeartDokument2 Seiten1 The Electrical Activity of The HeartRickertsNoch keine Bewertungen
- Technical Information: Navigation Lights User GuideDokument3 SeitenTechnical Information: Navigation Lights User GuideadammzjinNoch keine Bewertungen
- Neonatal Examination: 2016 EditionDokument18 SeitenNeonatal Examination: 2016 EditionDoha100% (1)
- Sinus Rhythm DisturbancesDokument3 SeitenSinus Rhythm DisturbancesMarcus Philip GonzalesNoch keine Bewertungen
- Acls TachiDokument1 SeiteAcls TachiratnawkNoch keine Bewertungen
- Arterial DiseaseDokument57 SeitenArterial DiseaseYil MosNoch keine Bewertungen
- ECG How To InterpretDokument10 SeitenECG How To InterpretMohamad DanialNoch keine Bewertungen
- Physio CardioDokument36 SeitenPhysio Cardiopooh7Noch keine Bewertungen
- Jurnal Reading Yanuar HermawanDokument10 SeitenJurnal Reading Yanuar HermawanAdrian UluNoch keine Bewertungen
- W ' E O M T ?: HAT S The Vidence For RAL Otor HerapyDokument2 SeitenW ' E O M T ?: HAT S The Vidence For RAL Otor HerapyAdrian UluNoch keine Bewertungen
- 1372 1386Dokument15 Seiten1372 1386Adrian UluNoch keine Bewertungen
- FF 6 ADokument6 SeitenFF 6 AAdrian UluNoch keine Bewertungen
- W ' E O M T ?: HAT S The Vidence For RAL Otor HerapyDokument2 SeitenW ' E O M T ?: HAT S The Vidence For RAL Otor HerapyAdrian UluNoch keine Bewertungen
- External Pulse Generator: Product HighlightsDokument2 SeitenExternal Pulse Generator: Product HighlightsScrbdJoe100Noch keine Bewertungen
- (Medbook4u Com) IllBaby1Dokument693 Seiten(Medbook4u Com) IllBaby1Certificate SurrenderNoch keine Bewertungen
- NCP Chest PainDokument2 SeitenNCP Chest PainCG Patron BamboNoch keine Bewertungen
- PVC Ablation in Non Ischaemic CMODokument8 SeitenPVC Ablation in Non Ischaemic CMOZaraNoch keine Bewertungen
- Atrial FibrillationDokument6 SeitenAtrial FibrillationMihai VicolNoch keine Bewertungen
- MCQ Kardiorespirasi 16Dokument10 SeitenMCQ Kardiorespirasi 16RevikaNoch keine Bewertungen
- Supraventricular Tachycardia: Arun Umesh Mahtani,, Devi Gopinath NairDokument17 SeitenSupraventricular Tachycardia: Arun Umesh Mahtani,, Devi Gopinath Nairwindar baquero100% (1)
- Daftar Pustaka ImaDokument2 SeitenDaftar Pustaka ImaDesrina PungkyNoch keine Bewertungen
- Tachycardia AlgorythmDokument1 SeiteTachycardia AlgorythmUZNAPMNoch keine Bewertungen
- ECG Interpretation Guide for Cardiac DysrhythmiasDokument70 SeitenECG Interpretation Guide for Cardiac DysrhythmiassserggiosNoch keine Bewertungen
- The Ischemic ElectrocardiogramDokument16 SeitenThe Ischemic ElectrocardiogramAdiel OjedaNoch keine Bewertungen
- 2 Midterm Exam Propedeutic-1: Attempt ReviewDokument8 Seiten2 Midterm Exam Propedeutic-1: Attempt ReviewYousra AhmedNoch keine Bewertungen
- UsmleDokument3 SeitenUsmleuwandfaNoch keine Bewertungen
- Patologi Bedah Sistem Kardiovaskuler Dan RespirasiDokument65 SeitenPatologi Bedah Sistem Kardiovaskuler Dan RespirasiMuhammad IqbalNoch keine Bewertungen
- Cardiac ArrestDokument19 SeitenCardiac ArrestHaimelien De LimosNoch keine Bewertungen
- Tetralogy of Fallot (TF)Dokument25 SeitenTetralogy of Fallot (TF)Safira RNoch keine Bewertungen
- Pericardial Diseases: Acute PericarditisDokument26 SeitenPericardial Diseases: Acute PericarditisamsirakNoch keine Bewertungen
- Ecg 2Dokument106 SeitenEcg 2hammad992Noch keine Bewertungen
- Atrioventricular Septal Defect Avsd CompleteDokument2 SeitenAtrioventricular Septal Defect Avsd CompleteFelicia Shan SugataNoch keine Bewertungen