Das könnte Ihnen auch gefallen
- Insight Adventures ™ 2011Dokument4 SeitenInsight Adventures ™ 2011Jesse GrosNoch keine Bewertungen
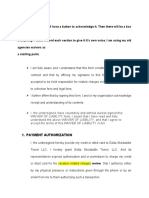
- 4 Waivers To Sign Off On Everything. Please Reword Each Section To Give It It's Own Voice, I Am Using My Old Agencies Waivers As A Starting PointDokument10 Seiten4 Waivers To Sign Off On Everything. Please Reword Each Section To Give It It's Own Voice, I Am Using My Old Agencies Waivers As A Starting PointDolapo AmobonyeNoch keine Bewertungen
- Travel Protection Plan Provides Cancellation Flexibility and Peace of MindDokument1 SeiteTravel Protection Plan Provides Cancellation Flexibility and Peace of MindgordomanotasNoch keine Bewertungen
- Guarantee LetterDokument1 SeiteGuarantee LetterWizcarmelo ParcellanoNoch keine Bewertungen
- Booking and Payments ConditionsDokument4 SeitenBooking and Payments ConditionsJeevan ParazuliNoch keine Bewertungen
- Tata Aig Travel Guard Claim FormDokument3 SeitenTata Aig Travel Guard Claim FormMarneni Yallamanda RaoNoch keine Bewertungen
- Airline Flight InsuranceDokument9 SeitenAirline Flight InsurancePratiksha MisalNoch keine Bewertungen
- Booking/Request Form: Contact DetailsDokument3 SeitenBooking/Request Form: Contact DetailsYuvalNoch keine Bewertungen
- RM AOSASw GBHWK7 RW 7 MP 99 QDokument38 SeitenRM AOSASw GBHWK7 RW 7 MP 99 QfernanroldanNoch keine Bewertungen
- Policy InformationDokument20 SeitenPolicy InformationMandyLynnEdwardsNoch keine Bewertungen
- Healix Travel InsuranceDokument14 SeitenHealix Travel InsuranceMel WallaceNoch keine Bewertungen
- Procedure to Claim Refund for Cancelled Flight InsuranceDokument1 SeiteProcedure to Claim Refund for Cancelled Flight InsuranceSubham TalukdarNoch keine Bewertungen
- Policy InformationDokument32 SeitenPolicy InformationSteve HagerupNoch keine Bewertungen
- T-17000 Rev. 4 7.28.2016Dokument56 SeitenT-17000 Rev. 4 7.28.2016Mark AbiadNoch keine Bewertungen
- Policy InformationDokument34 SeitenPolicy Informationnikhil0104Noch keine Bewertungen
- Service Agreement TemplateDokument3 SeitenService Agreement Templateceleste law50% (6)
- Policy WordingDokument15 SeitenPolicy WordingkvnkatNoch keine Bewertungen
- Appendices:: Terms & ConditionsDokument13 SeitenAppendices:: Terms & ConditionsYanYan YumulNoch keine Bewertungen
- Citi Card BenefitsDokument17 SeitenCiti Card BenefitsShashank ShekharNoch keine Bewertungen
- Guide 7Dokument32 SeitenGuide 7jstefankoNoch keine Bewertungen
- DCL CS - Personal Information - JAN31Dokument4 SeitenDCL CS - Personal Information - JAN31mauro libermanNoch keine Bewertungen
- General InsuranceDokument4 SeitenGeneral InsuranceNAKSHA007100% (1)
- BicyCal Terms & ConditionsDokument2 SeitenBicyCal Terms & ConditionsgreenbikeshareNoch keine Bewertungen
- Reg Form For Celtic PilgrimageDokument2 SeitenReg Form For Celtic PilgrimagebridgelmNoch keine Bewertungen
- Certificate of InsuranceDokument31 SeitenCertificate of InsurancebenNoch keine Bewertungen
- Certificate of Insurance PDFDokument31 SeitenCertificate of Insurance PDFbenNoch keine Bewertungen
- Motor Claim FormDokument4 SeitenMotor Claim FormAnsh SharmaNoch keine Bewertungen
- Metta Voyage Term e ConditionDokument3 SeitenMetta Voyage Term e ConditionHotel Sunny OceanNoch keine Bewertungen
- Condicionado Traducido Ingles Dec 20Dokument48 SeitenCondicionado Traducido Ingles Dec 20Apothecary ExpressNoch keine Bewertungen
- 167 19396 PDFDokument36 Seiten167 19396 PDFAnonymous FYSfr1Noch keine Bewertungen
- Liberty Insurance Claim ProcessDokument1 SeiteLiberty Insurance Claim ProcessChandresh SinghNoch keine Bewertungen
- General Conditions: Insurance CancellationDokument5 SeitenGeneral Conditions: Insurance CancellationCodruta HiripanNoch keine Bewertungen
- UpdatedAtlanta Public Schools - Registration FormDokument2 SeitenUpdatedAtlanta Public Schools - Registration Formglobetrek@1Noch keine Bewertungen
- Insurance & Takaful Claim Form GuideDokument7 SeitenInsurance & Takaful Claim Form GuidenuyuNoch keine Bewertungen
- CW and Non-US Celebrity Ver. 230101Dokument23 SeitenCW and Non-US Celebrity Ver. 230101Alex UlleNoch keine Bewertungen
- Aeroplan Ins Certs enDokument36 SeitenAeroplan Ins Certs enfaroNoch keine Bewertungen
- Bonus Travel - : - Airline Reservations - Car Rental Reservations - Hotel Reservations - Cruise and Tour PackagesDokument3 SeitenBonus Travel - : - Airline Reservations - Car Rental Reservations - Hotel Reservations - Cruise and Tour PackagesMarija BlagojevicNoch keine Bewertungen
- Travel Policy WordingsDokument36 SeitenTravel Policy WordingsKiran BangaloreNoch keine Bewertungen
- Juan Travel Services About My Options Before I Confirmed My Booking But I Declined To Purchase The TravelDokument1 SeiteJuan Travel Services About My Options Before I Confirmed My Booking But I Declined To Purchase The TravelAngelo De LeonNoch keine Bewertungen
- Terms and Conditions en 2017Dokument9 SeitenTerms and Conditions en 2017milandivacNoch keine Bewertungen
- Insurance PolicyDokument2 SeitenInsurance Policyratilal bhushanNoch keine Bewertungen
- 1Accident-Notification-Form Old SchemeDokument6 Seiten1Accident-Notification-Form Old SchemeJosephino CastilloNoch keine Bewertungen
- SmartTraveller Travel Claim FormDokument2 SeitenSmartTraveller Travel Claim FormKhairul HaizamNoch keine Bewertungen
- Your Guide To Protection Benefits: Citi PrestigeDokument40 SeitenYour Guide To Protection Benefits: Citi PrestigeJames SmithNoch keine Bewertungen
- FPG Insurance Proposal - 2023Dokument3 SeitenFPG Insurance Proposal - 2023Marylyn Joy PamatigaNoch keine Bewertungen
- Non Owned Hired Auto Supplement InsuranceDokument2 SeitenNon Owned Hired Auto Supplement InsuranceJohn RossNoch keine Bewertungen
- Booking FormDokument1 SeiteBooking FormkarynmarkwellNoch keine Bewertungen
- Travel Requirements For Carestream Van Zile Travel Service: Non-EmployeesDokument3 SeitenTravel Requirements For Carestream Van Zile Travel Service: Non-EmployeessasrfNoch keine Bewertungen
- Travel Smart Intl Terms and ConditionsDokument11 SeitenTravel Smart Intl Terms and ConditionsUmair A. SaryoNoch keine Bewertungen
- AA Claim FormDokument5 SeitenAA Claim FormpenchanskyNoch keine Bewertungen
- Claim Report: Travel Insurance Report FormDokument7 SeitenClaim Report: Travel Insurance Report Formhoneytrap99Noch keine Bewertungen
- Recording Claim Losses and Expenses: Your Guide and Forms: OverviewDokument11 SeitenRecording Claim Losses and Expenses: Your Guide and Forms: OverviewharryNoch keine Bewertungen
- RE: Product: Claim Number: Incident Date:: Amex Assurance Company PO BOX 981553 EL PASO TX 79998-9920Dokument6 SeitenRE: Product: Claim Number: Incident Date:: Amex Assurance Company PO BOX 981553 EL PASO TX 79998-9920Alexander RogersNoch keine Bewertungen
- Travel Insurance Claim FormDokument5 SeitenTravel Insurance Claim FormKailash KabraNoch keine Bewertungen
- Axa PolicyDokument8 SeitenAxa PolicyazNoch keine Bewertungen
- Insurance PolicyDokument2 SeitenInsurance Policyqx7spnzxmmNoch keine Bewertungen
- Ghislain Mufanzala KahashaDokument3 SeitenGhislain Mufanzala KahashaEfi ColorNoch keine Bewertungen
- Party Rental Business Playbook Everything Needed To Start a Moonwalk Business!Von EverandParty Rental Business Playbook Everything Needed To Start a Moonwalk Business!Noch keine Bewertungen
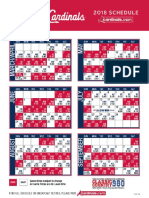
- 2018 Cardinal ScheduleDokument1 Seite2018 Cardinal Schedulebsnider3728Noch keine Bewertungen
- Guyot Jan 18Dokument8 SeitenGuyot Jan 18bsnider3728Noch keine Bewertungen
- Guyot April 2017Dokument8 SeitenGuyot April 2017bsnider3728Noch keine Bewertungen
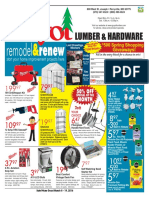
- January: Lumber & HardwareDokument8 SeitenJanuary: Lumber & Hardwarebsnider3728Noch keine Bewertungen
- Guyot August 2017Dokument8 SeitenGuyot August 2017bsnider3728Noch keine Bewertungen
- Small Business Saturday 2016Dokument2 SeitenSmall Business Saturday 2016bsnider3728Noch keine Bewertungen
- Lumber & Hardware: We Now Carry Melissa & Doug Toys!Dokument4 SeitenLumber & Hardware: We Now Carry Melissa & Doug Toys!bsnider3728Noch keine Bewertungen
- Guyot December 2017 AdDokument8 SeitenGuyot December 2017 Adbsnider3728Noch keine Bewertungen
- Guyot October Ad 2017Dokument8 SeitenGuyot October Ad 2017bsnider3728Noch keine Bewertungen
- May Guyot 2017Dokument8 SeitenMay Guyot 2017bsnider3728Noch keine Bewertungen
- Guyot February 2017Dokument2 SeitenGuyot February 2017bsnider3728Noch keine Bewertungen
- Lumber & Hardware: Fall $500 Give-Away WinnersDokument8 SeitenLumber & Hardware: Fall $500 Give-Away Winnersbsnider3728Noch keine Bewertungen
- November 16 GuyotDokument4 SeitenNovember 16 Guyotbsnider3728Noch keine Bewertungen
- Guyot DecemberDokument4 SeitenGuyot Decemberbsnider3728Noch keine Bewertungen
- Lumber & Hardware: Save On DuckbackDokument8 SeitenLumber & Hardware: Save On Duckbackbsnider3728Noch keine Bewertungen
- August2016 GuyotDokument4 SeitenAugust2016 Guyotbsnider3728Noch keine Bewertungen
- April 2016 2 GuyotDokument8 SeitenApril 2016 2 Guyotbsnider3728Noch keine Bewertungen
- September 16 Guyot For SuntimesDokument8 SeitenSeptember 16 Guyot For Suntimesbsnider3728Noch keine Bewertungen
- 2016 April Bogo AdDokument1 Seite2016 April Bogo Adbsnider3728Noch keine Bewertungen
- Guyot March AdDokument8 SeitenGuyot March Adbsnider3728Noch keine Bewertungen
- Lumber & Hardware: Values Await You!Dokument8 SeitenLumber & Hardware: Values Await You!bsnider3728Noch keine Bewertungen
- Feb 2016 Guyot Paint SaleDokument1 SeiteFeb 2016 Guyot Paint Salebsnider3728Noch keine Bewertungen
- April 2015 GuyotDokument8 SeitenApril 2015 Guyotbsnider3728Noch keine Bewertungen
- Season: Lumber & HardwareDokument8 SeitenSeason: Lumber & Hardwarebsnider3728Noch keine Bewertungen
- Guyot For JulyDokument8 SeitenGuyot For Julybsnider3728Noch keine Bewertungen
- Guyot For FebruaryDokument4 SeitenGuyot For Februarybsnider3728Noch keine Bewertungen
- Guyot For Sept 2015Dokument8 SeitenGuyot For Sept 2015bsnider3728Noch keine Bewertungen
- Guyot May 2015Dokument8 SeitenGuyot May 2015bsnider3728Noch keine Bewertungen
- 38th Murphysboro Sophomore Basketball Tournament 2015Dokument1 Seite38th Murphysboro Sophomore Basketball Tournament 2015bsnider3728Noch keine Bewertungen
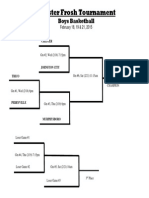
- Chester FBBK Trny 14-15 BracketDokument1 SeiteChester FBBK Trny 14-15 Bracketbsnider3728Noch keine Bewertungen