Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Brown Mcqs in PathologyDokument69 SeitenBrown Mcqs in Pathologyfadiawwad100% (4)
- Materi 1 Dr. Apt. Diana Laila Ramatillah, M.farmDokument32 SeitenMateri 1 Dr. Apt. Diana Laila Ramatillah, M.farmDimas RfNoch keine Bewertungen
- Pathophysiology: Mycobacterium Leprae/ Mycobacterium LepromatosisDokument2 SeitenPathophysiology: Mycobacterium Leprae/ Mycobacterium LepromatosisAkeroNoch keine Bewertungen
- Microbial Diseases of The Different Organ System and Epidem.Dokument36 SeitenMicrobial Diseases of The Different Organ System and Epidem.Ysabelle GutierrezNoch keine Bewertungen
- Quiz On School Health NursingDokument7 SeitenQuiz On School Health Nursingchoobi0% (2)
- Bio SSM Term 2 With Cbse QuestionsDokument148 SeitenBio SSM Term 2 With Cbse QuestionsArcha B SuneeshNoch keine Bewertungen
- Vaccine IMCIDokument2 SeitenVaccine IMCIEricNoch keine Bewertungen
- Estafilococo Aureus Patogenicidad. Virulencia 2021Dokument23 SeitenEstafilococo Aureus Patogenicidad. Virulencia 2021Gabriela ChaconNoch keine Bewertungen
- A Brief History of The Discovery of The ImmunoglobDokument6 SeitenA Brief History of The Discovery of The ImmunoglobVentanucoNoch keine Bewertungen
- Hematology 1 L2 Hematopoiesis LectureDokument4 SeitenHematology 1 L2 Hematopoiesis LectureChelze Faith DizonNoch keine Bewertungen
- Diagnosis and Management of Tinea InfectionsDokument10 SeitenDiagnosis and Management of Tinea InfectionsGaluh Citta PuspitasariNoch keine Bewertungen
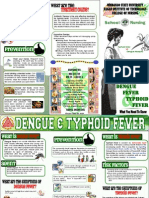
- Final Dengue and TyphoidDokument2 SeitenFinal Dengue and TyphoidJessie Glenn EgamNoch keine Bewertungen
- Hepatitis B VaccineDokument3 SeitenHepatitis B VaccineChoox PriiNoch keine Bewertungen
- Vas JEMDokument91 SeitenVas JEMJeM LobiLabNoch keine Bewertungen
- Lab Result Kiran Farebrother VDRLDokument1 SeiteLab Result Kiran Farebrother VDRLMazterMaztermaztermazter MaztermaztermazterYandeNoch keine Bewertungen
- Whooping Cough (Pertussis) InformationDokument2 SeitenWhooping Cough (Pertussis) InformationtombstoneepitaphNoch keine Bewertungen
- Medical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual DownloadDokument28 SeitenMedical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual DownloadJason AppellNoch keine Bewertungen
- Submitted To DR Ritu Jindal Professor and Head of Dept Dept of Pedodontics and Preventive DentistryDokument43 SeitenSubmitted To DR Ritu Jindal Professor and Head of Dept Dept of Pedodontics and Preventive Dentistrydr parveen bathlaNoch keine Bewertungen
- Th1/Th2 Dominance Symptoms ListDokument3 SeitenTh1/Th2 Dominance Symptoms ListXemantic100% (1)
- Materi MIMBAR 20 - BPK HadiDokument20 SeitenMateri MIMBAR 20 - BPK HadiYoga RivaldiNoch keine Bewertungen
- Immunology Exam November 2019Dokument13 SeitenImmunology Exam November 2019Vuyo TunesNoch keine Bewertungen
- Assignment 3 Pandemic (Zika Virus) Hebat Module (Unit 2)Dokument9 SeitenAssignment 3 Pandemic (Zika Virus) Hebat Module (Unit 2)Helen PappuNoch keine Bewertungen
- CertificateDokument1 SeiteCertificateHдиѕөмє SãJîDNoch keine Bewertungen
- Acute Hemorrhagic Leukoencephalitis Hurst Disease Secondary To h1n1 in A Child A Story of Full Recovery From QatarDokument4 SeitenAcute Hemorrhagic Leukoencephalitis Hurst Disease Secondary To h1n1 in A Child A Story of Full Recovery From Qataremilia candraNoch keine Bewertungen
- Essentials of MicrobiologyDokument647 SeitenEssentials of MicrobiologyMarsidi SaidNoch keine Bewertungen
- Module 2 - PLANNING (Davao)Dokument20 SeitenModule 2 - PLANNING (Davao)Anne Abejuela ObialNoch keine Bewertungen
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDokument52 SeitenCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaNoch keine Bewertungen
- 4th Generation HIV TestingDokument31 Seiten4th Generation HIV TestingSC SCNoch keine Bewertungen
- Infection Control in Dental RadiologyDokument41 SeitenInfection Control in Dental RadiologyDrShweta Saini0% (1)
- Anatomy - QuizDokument2 SeitenAnatomy - Quizloan kimNoch keine Bewertungen