Das könnte Ihnen auch gefallen
- Anaesthetic of Choice During Pregnancy and LactationDokument5 SeitenAnaesthetic of Choice During Pregnancy and LactationDegefu TadesseNoch keine Bewertungen
- How To Stop Overthinking EverythingDokument17 SeitenHow To Stop Overthinking EverythingKai Bade100% (2)
- Anes Preoperative-AssessmentDokument6 SeitenAnes Preoperative-AssessmentChristine Mendoza100% (1)
- Pharmacology AntibioticsDokument70 SeitenPharmacology Antibioticsmaggie100% (1)
- Social Success Requires You Be Social - Girls ChaseDokument16 SeitenSocial Success Requires You Be Social - Girls ChaseKhalaf SpencerNoch keine Bewertungen
- Health9 - Q2 - Mod1-Drug Scenario in The Philippines - v1Dokument16 SeitenHealth9 - Q2 - Mod1-Drug Scenario in The Philippines - v1Rhea Mae Julian100% (2)
- The Present (Universal Truth)Dokument111 SeitenThe Present (Universal Truth)Hitesh YadavNoch keine Bewertungen
- Preoperative Assessment and Premedication - PACUDokument60 SeitenPreoperative Assessment and Premedication - PACUTraceNoch keine Bewertungen
- MIND ON PORN (Practical Research)Dokument18 SeitenMIND ON PORN (Practical Research)Ivy DeoquinoNoch keine Bewertungen
- Pulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveVon EverandPulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveNoch keine Bewertungen
- I.V. FluidsDokument33 SeitenI.V. FluidsVineel Bezawada100% (1)
- Immediate Post Anesthetic RecoveryDokument12 SeitenImmediate Post Anesthetic Recoverysubvig100% (2)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
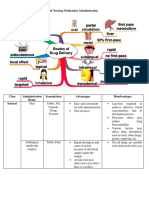
- Different Routes of Nursing Medication AdministrationDokument13 SeitenDifferent Routes of Nursing Medication AdministrationRonica MendozaNoch keine Bewertungen
- Anesthesia TechnologyDokument56 SeitenAnesthesia TechnologyDeepali SinghNoch keine Bewertungen
- Pre AnaestheticsDokument69 SeitenPre AnaestheticsPraney SlathiaNoch keine Bewertungen
- Unit 3 Fluid and ElectrolyteDokument20 SeitenUnit 3 Fluid and ElectrolyteChandan ShahNoch keine Bewertungen
- Sub.-Hospital and Clinical Pharmacy Chapter-3 Drug Distribution System in HospitalDokument38 SeitenSub.-Hospital and Clinical Pharmacy Chapter-3 Drug Distribution System in HospitalVescop 18-21Noch keine Bewertungen
- NUR 104 Nursing Process MY NOTESDokument77 SeitenNUR 104 Nursing Process MY NOTESmeanne073100% (1)
- MethergineDokument2 SeitenMethergineJulie May33% (3)
- Neonatal ResuscitationDokument7 SeitenNeonatal ResuscitationJavier López García100% (1)
- Pharmacy Training - Gastro Intestinal TractDokument56 SeitenPharmacy Training - Gastro Intestinal TractDylanSalam100% (1)
- Anaesthesia Outside The Operating Theatre Update 2010Dokument5 SeitenAnaesthesia Outside The Operating Theatre Update 2010Marcella AmadeaNoch keine Bewertungen
- Administering Medication Via A Small-Volume NebulizerDokument2 SeitenAdministering Medication Via A Small-Volume NebulizerJerilee SoCute WattsNoch keine Bewertungen
- Bangalore DR ListDokument11 SeitenBangalore DR Listkrisveli76% (42)
- UntitledDokument48 SeitenUntitledSakshi YadavNoch keine Bewertungen
- Cancer Consult Expertise in Clinical Practice, Volume 1 Solid Tumors & Supportive Care 2nd Edition (PDF Book)Dokument754 SeitenCancer Consult Expertise in Clinical Practice, Volume 1 Solid Tumors & Supportive Care 2nd Edition (PDF Book)Duk Han Kim100% (1)
- Beta LactamDokument18 SeitenBeta LactamCesar Saba0% (1)
- PHARMAKOKINETICSDokument16 SeitenPHARMAKOKINETICSGauthaman KarunakaranNoch keine Bewertungen
- Circulatory Shock: Santosh DevDokument32 SeitenCirculatory Shock: Santosh DevdevdsantoshNoch keine Bewertungen
- Ah02 Anesthesia TechnicianDokument1 SeiteAh02 Anesthesia TechnicianbiomedmaulikNoch keine Bewertungen
- A Review Sublingual Route For Systemic Drug DeliveryDokument6 SeitenA Review Sublingual Route For Systemic Drug DeliveryPriambodo Gandhi100% (1)
- Unit 7Dokument29 SeitenUnit 7Deta Meila Putri0% (1)
- Pharmacotherapy During Pregnancy, Childbirth and Lactation: Principles To ConsiderDokument7 SeitenPharmacotherapy During Pregnancy, Childbirth and Lactation: Principles To Consideryuliana nurcahyatiNoch keine Bewertungen
- Chapter - 037 - 1 Infective Endocarditis ClassDokument41 SeitenChapter - 037 - 1 Infective Endocarditis ClassWisdomIsMiseryNoch keine Bewertungen
- Seminar 4Dokument49 SeitenSeminar 4Yamuna SubramaniamNoch keine Bewertungen
- Coccidiosis Power PointDokument36 SeitenCoccidiosis Power PointBob UrbandubNoch keine Bewertungen
- Premedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Dokument34 SeitenPremedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Viresh Upase Roll No 130. / 8th termNoch keine Bewertungen
- IV TherapyDokument7 SeitenIV Therapydlneisha61Noch keine Bewertungen
- Osteoarthritis and Role of NurseDokument15 SeitenOsteoarthritis and Role of NurseAl VivoNoch keine Bewertungen
- Obstetrics AnesthesiaDokument31 SeitenObstetrics AnesthesiaNorfarhanah ZakariaNoch keine Bewertungen
- Nursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalDokument55 SeitenNursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalFayizatul AkmarNoch keine Bewertungen
- 5 - Local AnetheticsDokument30 Seiten5 - Local AnetheticsCorry QyNoch keine Bewertungen
- Pacu Tylenol PresentationDokument10 SeitenPacu Tylenol PresentationStanford AnesthesiaNoch keine Bewertungen
- Patient Controlled AnalgesiaDokument129 SeitenPatient Controlled AnalgesiamehranerezvaniNoch keine Bewertungen
- Mech Vent For Fun & BenefitDokument196 SeitenMech Vent For Fun & BenefitJade Providence100% (1)
- Fluid and Electrolyte TherapyDokument39 SeitenFluid and Electrolyte TherapyrikarzNoch keine Bewertungen
- Physiology of BalanceDokument27 SeitenPhysiology of Balancemulkihakam21Noch keine Bewertungen
- Opioid-Free Anaesthesia - Atow-461-00 - BDokument6 SeitenOpioid-Free Anaesthesia - Atow-461-00 - BEugenio Martinez HurtadoNoch keine Bewertungen
- (CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaDokument41 Seiten(CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaRahman Anwar100% (1)
- Poisoning and Its ManagementDokument25 SeitenPoisoning and Its ManagementAnant kushwahaNoch keine Bewertungen
- Technique: Preventing and Controlling Infections in Home Care and HospiceDokument7 SeitenTechnique: Preventing and Controlling Infections in Home Care and HospiceOlaMostafaNoch keine Bewertungen
- Regional AnesthesiaDokument54 SeitenRegional AnesthesiaIdza Fariha AfriNoch keine Bewertungen
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDokument2 SeitenAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasNoch keine Bewertungen
- 2017 ASA Refresher Courses in Anesthesiology (165-172)Dokument8 Seiten2017 ASA Refresher Courses in Anesthesiology (165-172)Edelweis JavanicaNoch keine Bewertungen
- Neurologic Assessment RationaleDokument16 SeitenNeurologic Assessment RationaleflorenzoNoch keine Bewertungen
- Factors Affecting Drug Metabolism PDFDokument2 SeitenFactors Affecting Drug Metabolism PDFPaige50% (2)
- Pharmacology: Erick Sioco Inserto, RNDokument3 SeitenPharmacology: Erick Sioco Inserto, RNAerickt Sioco-InsertoNoch keine Bewertungen
- Introduction To HematologyDokument61 SeitenIntroduction To HematologyThis is PonyNoch keine Bewertungen
- Cardiovascular System: Medrcal-Surgrcal NursingDokument6 SeitenCardiovascular System: Medrcal-Surgrcal NursingGTX123Noch keine Bewertungen
- Chapter 01: Drug Definitions, Standards, and Information Sources Willihnganz: Clayton's Basic Pharmacology For Nurses, 18th EditionDokument4 SeitenChapter 01: Drug Definitions, Standards, and Information Sources Willihnganz: Clayton's Basic Pharmacology For Nurses, 18th Editioncharlie johnsonNoch keine Bewertungen
- UCL Aneasthesia Year 4 Workbookv15Dokument83 SeitenUCL Aneasthesia Year 4 Workbookv15Jay KayNoch keine Bewertungen
- Sample Q1Dokument34 SeitenSample Q1Joyeeta Tahseen KhanNoch keine Bewertungen
- Local AnaestheticsDokument26 SeitenLocal Anaestheticsv_vijayakanth7656Noch keine Bewertungen
- Critical Care in PregnancyDokument21 SeitenCritical Care in PregnancyamuzaNoch keine Bewertungen
- Clinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978Von EverandClinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978P. Duchêne-MarullazNoch keine Bewertungen
- Components of Food-Questions and AnswersDokument3 SeitenComponents of Food-Questions and Answersmahesh_mymailNoch keine Bewertungen
- E60 FullDokument232 SeitenE60 FullPedro PerezNoch keine Bewertungen
- Pathophysiology of ChorioamnionitisDokument1 SeitePathophysiology of Chorioamnionitisjhobarry0% (1)
- Special Power of Attorney: Benedict Joseph M. CruzDokument1 SeiteSpecial Power of Attorney: Benedict Joseph M. CruzJson GalvezNoch keine Bewertungen
- The ADHD Diagnosis GuideDokument13 SeitenThe ADHD Diagnosis GuideArunima KapoorNoch keine Bewertungen
- Early Intervention - Social Media DetoxDokument4 SeitenEarly Intervention - Social Media DetoxYouth in Science and Business FoundationNoch keine Bewertungen
- Department of Education: Cluster 8A Northeast Marilog In-Service Training (Inset)Dokument8 SeitenDepartment of Education: Cluster 8A Northeast Marilog In-Service Training (Inset)Jeffren P. MiguelNoch keine Bewertungen
- Infopack - Learn From Life - RevisedDokument10 SeitenInfopack - Learn From Life - RevisedProutist Universal MaltaNoch keine Bewertungen
- Patient Safety Incidents Associated With Airway Devices in Critical Care: A Review of Reports To The UK National Patient Safety AgencyDokument8 SeitenPatient Safety Incidents Associated With Airway Devices in Critical Care: A Review of Reports To The UK National Patient Safety AgencyBudi YunantoNoch keine Bewertungen
- SGS Corpcom Business Statements A1 en LR 19 05Dokument6 SeitenSGS Corpcom Business Statements A1 en LR 19 05Tutunaru OxanaNoch keine Bewertungen
- Workers Welfare Standards Qatar 2022 v2Dokument12 SeitenWorkers Welfare Standards Qatar 2022 v2Ali ImamNoch keine Bewertungen
- KNUST Owned Hostels Room AllocatorDokument9 SeitenKNUST Owned Hostels Room Allocatoralyussif84Noch keine Bewertungen
- Drug-Study ErgonDokument2 SeitenDrug-Study ErgonPaolo UyNoch keine Bewertungen
- Transferring and BandagingDokument8 SeitenTransferring and BandagingDarwin AndalNoch keine Bewertungen
- SARTIKA LESTARI - PositifDokument1 SeiteSARTIKA LESTARI - Positifsartika lestariNoch keine Bewertungen
- Hello G10 Semester 2Dokument136 SeitenHello G10 Semester 2romaehab201912Noch keine Bewertungen
- Format Hospital PDFDokument8 SeitenFormat Hospital PDFAnil KumarNoch keine Bewertungen
- Automated Online Exam Proctor: A Synopsis Report Submitted in Partial Fulfillment of The Requirement For The Degree ofDokument11 SeitenAutomated Online Exam Proctor: A Synopsis Report Submitted in Partial Fulfillment of The Requirement For The Degree ofAkhil SinghNoch keine Bewertungen
- Puti Mustika Swandyani, Agus Santoso, Yohanes KristiantoDokument11 SeitenPuti Mustika Swandyani, Agus Santoso, Yohanes KristiantoAnonimNoch keine Bewertungen
- Healthy Living: 33617 - 07 - Ch07 - p129-149 Pp4.indd 129 2/17/10 7:38:42 PMDokument46 SeitenHealthy Living: 33617 - 07 - Ch07 - p129-149 Pp4.indd 129 2/17/10 7:38:42 PMYaqut CabrayilovaNoch keine Bewertungen
- Pros and Cons of Research in E.H.Dokument3 SeitenPros and Cons of Research in E.H.goldMINDNoch keine Bewertungen
- Use of Alternative Daily Cover at Landfills: I D E MDokument3 SeitenUse of Alternative Daily Cover at Landfills: I D E MKrieteNoch keine Bewertungen