Das könnte Ihnen auch gefallen
- NBME 18 AnswersDokument202 SeitenNBME 18 AnswersTony Lǎo Hǔ Chen86% (37)
- Harrison MCQ NephrologyDokument7 SeitenHarrison MCQ Nephrologydrtpk80% (15)
- Board Reveiw Electrolyte Acid Base MCQ and AnswerDokument15 SeitenBoard Reveiw Electrolyte Acid Base MCQ and AnswerEma100% (8)
- Renal FailureDokument48 SeitenRenal FailureMakanjuola Osuolale John100% (1)
- Online Assignment Kidney DiseasesDokument22 SeitenOnline Assignment Kidney DiseasessyamosNoch keine Bewertungen
- SociologyDokument5 SeitenSociologyRAJUNoch keine Bewertungen
- Pathology SyllabusDokument15 SeitenPathology Syllabussingireddi1revathi100% (2)
- SociologyDokument5 SeitenSociologyRAJUNoch keine Bewertungen
- SociologyDokument5 SeitenSociologyRAJUNoch keine Bewertungen
- Packrat 3-21-14 AnswerDokument40 SeitenPackrat 3-21-14 AnswerChristina Ly100% (1)
- IDEXX CBC Chem ExplainedDokument38 SeitenIDEXX CBC Chem Explainedmmatthew74Noch keine Bewertungen
- Renal Failure NoteDokument27 SeitenRenal Failure Notechiemerieagana3Noch keine Bewertungen
- BubreDokument10 SeitenBubreharryNoch keine Bewertungen
- Chronic Kidney DiseaseDokument8 SeitenChronic Kidney DiseaseAyiessa_AJNoch keine Bewertungen
- Kidney Failure FactsDokument19 SeitenKidney Failure Factss.khan9211rediffmail.comNoch keine Bewertungen
- Kidney FailureDokument2 SeitenKidney Failuredanee しNoch keine Bewertungen
- What Is Kidney MalfunctioningDokument7 SeitenWhat Is Kidney MalfunctioningPooja SinghNoch keine Bewertungen
- Picture of The Kidneys: Kidney ConditionsDokument2 SeitenPicture of The Kidneys: Kidney ConditionsEarl Jay UayanNoch keine Bewertungen
- Normal Kidneys and Their Function: Chronic Kidney Disease OverviewDokument12 SeitenNormal Kidneys and Their Function: Chronic Kidney Disease OverviewLouie Collado100% (1)
- Kidney Conditions: PyelonephritisDokument3 SeitenKidney Conditions: PyelonephritiskenNoch keine Bewertungen
- What Are The KidneysDokument4 SeitenWhat Are The KidneysKathiresan KathirNoch keine Bewertungen
- Rajashree 12Dokument13 SeitenRajashree 12Rakesh BarmanNoch keine Bewertungen
- Chronic Renal FailureDokument26 SeitenChronic Renal FailureRemington Thomas II100% (5)
- IntroductionDokument3 SeitenIntroductionDoaa AskerNoch keine Bewertungen
- Chronic Kidney Disease OverviewDokument28 SeitenChronic Kidney Disease Overviewomie22100% (9)
- What Are The Kidneys?: Kidney FailureDokument9 SeitenWhat Are The Kidneys?: Kidney FailureNurfarhanim Akmal Mohd KhalidNoch keine Bewertungen
- Chronic Kidney Disease OverviewDokument15 SeitenChronic Kidney Disease Overviewjames100% (1)
- By3 Safaa Mohammed Abd-Elghany: V Nder SupervisionDokument13 SeitenBy3 Safaa Mohammed Abd-Elghany: V Nder SupervisiontrrdsNoch keine Bewertungen
- Acute Renal FailureDokument25 SeitenAcute Renal Failurebkbaljeet116131Noch keine Bewertungen
- BIOLOGY (Autosaved)Dokument16 SeitenBIOLOGY (Autosaved)Prithika ShankarNoch keine Bewertungen
- Acute Kidney FailureDokument8 SeitenAcute Kidney FailureRaidis PangilinanNoch keine Bewertungen
- Kidney DisorderDokument5 SeitenKidney DisorderTWINKLE MAE EGAYNoch keine Bewertungen
- Chronic Kidney Disease OverviewDokument12 SeitenChronic Kidney Disease OverviewHalles Beverlyn Crisostomo GeraldeNoch keine Bewertungen
- Renal Diseaseppt2789Dokument112 SeitenRenal Diseaseppt2789Sundeep SharmaNoch keine Bewertungen
- Pa Tho PhysiologyDokument14 SeitenPa Tho PhysiologyPatricia LeonorNoch keine Bewertungen
- College of Nursing: Civil HospitalDokument15 SeitenCollege of Nursing: Civil HospitalDipal Jignesh PatelNoch keine Bewertungen
- DialysisDokument34 SeitenDialysisAntonio Junior CastroNoch keine Bewertungen
- Acute Kidney Failure OverviewDokument4 SeitenAcute Kidney Failure OverviewchichauskyNoch keine Bewertungen
- End-Stage Renal DiseaseDokument7 SeitenEnd-Stage Renal Diseasemarvin de castroNoch keine Bewertungen
- SN Allen F. RojasDokument22 SeitenSN Allen F. Rojaskane1978Noch keine Bewertungen
- L.10 Kidney HealthDokument37 SeitenL.10 Kidney HealthMunira SulimanNoch keine Bewertungen
- Genitourinary System FinalDokument8 SeitenGenitourinary System FinalKristian DolletonNoch keine Bewertungen
- Acute Renal FailureDokument2 SeitenAcute Renal FailureLaura BodeaNoch keine Bewertungen
- Presentation Patho Nurs2012Dokument49 SeitenPresentation Patho Nurs2012shannonsamlal2021Noch keine Bewertungen
- What Is Kidney (Renal) Failure?: Female Urinary TractDokument6 SeitenWhat Is Kidney (Renal) Failure?: Female Urinary TractthenameisvijayNoch keine Bewertungen
- KIdney FailureDokument5 SeitenKIdney FailureLillabinNoch keine Bewertungen
- Renal FailureDokument4 SeitenRenal FailureMunish DograNoch keine Bewertungen
- Continue RENALDokument8 SeitenContinue RENALLeofe CorregidorNoch keine Bewertungen
- End Stage Renal DiseaseDokument6 SeitenEnd Stage Renal DiseaseLeiNoch keine Bewertungen
- Acute Kidney InjuryDokument6 SeitenAcute Kidney Injurytherese BNoch keine Bewertungen
- Renal Pathophysiology by GPTDokument3 SeitenRenal Pathophysiology by GPTphilipcNoch keine Bewertungen
- Acute Kidney FailureDokument8 SeitenAcute Kidney Failureanimesh pandaNoch keine Bewertungen
- Chronic Kidney DiseaseDokument7 SeitenChronic Kidney Diseasekzbreakerr100% (1)
- Acute and Chronic Renal FailureDokument21 SeitenAcute and Chronic Renal FailureStephina ImmaculateNoch keine Bewertungen
- Chronic Kidney FailureDokument21 SeitenChronic Kidney FailurePatrick John AsperillaNoch keine Bewertungen
- Chronic Kidney DiseaseDokument11 SeitenChronic Kidney DiseaseMah AlfaroNoch keine Bewertungen
- Stages of Chronic Kidney Disease Stage Description GFR Ml/min/1.73mDokument4 SeitenStages of Chronic Kidney Disease Stage Description GFR Ml/min/1.73mMegan SamsonNoch keine Bewertungen
- Renal FailuireDokument39 SeitenRenal FailuireAmbroseNoch keine Bewertungen
- KidneyDokument3 SeitenKidneyAngelicaNoch keine Bewertungen
- Acute Tubular Necrosis PuputDokument7 SeitenAcute Tubular Necrosis Puputganesa ekaNoch keine Bewertungen
- Kidney FailureDokument8 SeitenKidney FailureКатя ДементьеваNoch keine Bewertungen
- The Kidneys GRADE 4Dokument16 SeitenThe Kidneys GRADE 4Yvonne OrellanaNoch keine Bewertungen
- Case Analysis FinDokument64 SeitenCase Analysis Finlhiamdm1208Noch keine Bewertungen
- Frequently Asked Questions About Kidney Health (English) : Question: What Are The Signs and Symptoms of Kidney Disorder?Dokument6 SeitenFrequently Asked Questions About Kidney Health (English) : Question: What Are The Signs and Symptoms of Kidney Disorder?Arjay NeivaNoch keine Bewertungen
- ACUTE AND CHRONIC RENAL FailureDokument15 SeitenACUTE AND CHRONIC RENAL Failuremaggayj11100% (1)
- Problems of The Excretory System: Why Drink Water?Dokument4 SeitenProblems of The Excretory System: Why Drink Water?Adeeb ChoudhuryNoch keine Bewertungen
- The Facts About Chronic Kidney Disease (CKD) : Back To TopDokument9 SeitenThe Facts About Chronic Kidney Disease (CKD) : Back To Top2netvelasquezNoch keine Bewertungen
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Varicose VainsDokument28 SeitenVaricose Vainssingireddi1revathi100% (1)
- Community Health NursingDokument14 SeitenCommunity Health Nursingsingireddi1revathi100% (2)
- CommunicationDokument9 SeitenCommunicationsingireddi1revathiNoch keine Bewertungen
- Tibial and Femur FactrueDokument25 SeitenTibial and Femur Factruesingireddi1revathiNoch keine Bewertungen
- Course of Instruction Second Year B. SCDokument3 SeitenCourse of Instruction Second Year B. SCsingireddi1revathiNoch keine Bewertungen
- Medical Surgical NursingDokument31 SeitenMedical Surgical Nursingsingireddi1revathi100% (3)
- Ordinance & R.nursingDokument9 SeitenOrdinance & R.nursingsingireddi1revathiNoch keine Bewertungen
- Pathology and GeneticsDokument11 SeitenPathology and Geneticssingireddi1revathiNoch keine Bewertungen
- Pathology and GeneticsDokument11 SeitenPathology and Geneticssingireddi1revathi33% (3)
- Final Infection Contro AssignementDokument24 SeitenFinal Infection Contro Assignementsingireddi1revathiNoch keine Bewertungen
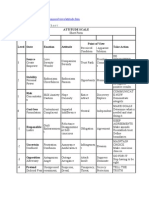
- Attitude ScaleDokument51 SeitenAttitude Scalesingireddi1revathi100% (3)
- An Introduction To Alternative and Complementary MedicineDokument13 SeitenAn Introduction To Alternative and Complementary Medicinesingireddi1revathiNoch keine Bewertungen
- Counseling 2Dokument39 SeitenCounseling 2singireddi1revathiNoch keine Bewertungen
- 6 Acute Kidney InjuryDokument36 Seiten6 Acute Kidney InjuryyaminmuhNoch keine Bewertungen
- Nursing Care of Patients With Kidney DisordersDokument23 SeitenNursing Care of Patients With Kidney DisordersYAMINIPRIYANNoch keine Bewertungen
- PI e UREA 15Dokument2 SeitenPI e UREA 15dewi asnaniNoch keine Bewertungen
- Renal PathologyDokument49 SeitenRenal PathologyQusaiBadrNoch keine Bewertungen
- Renal FailureDokument27 SeitenRenal FailureMae DacerNoch keine Bewertungen
- Non-Protein Nitrogenous Compounds (NPN'S) : Reman A. Alingasa, RMTDokument47 SeitenNon-Protein Nitrogenous Compounds (NPN'S) : Reman A. Alingasa, RMTLoulou ApolloNoch keine Bewertungen
- CC Lab 6 TransesDokument6 SeitenCC Lab 6 TransesCiara PamonagNoch keine Bewertungen
- Acute Kidney InjuryDokument8 SeitenAcute Kidney InjuryRohitKumarNoch keine Bewertungen
- PI AmiparenDokument4 SeitenPI AmiparenDietisien MHKNNoch keine Bewertungen
- (F3) Clinical Pathology DR KitsDokument15 Seiten(F3) Clinical Pathology DR KitsBryan Nartatez BautistaNoch keine Bewertungen
- Case Study On ARFDokument33 SeitenCase Study On ARFKaku ManishaNoch keine Bewertungen
- Hopkins Medicine Review NephrologyDokument35 SeitenHopkins Medicine Review NephrologyMuhammad Bilal50% (2)
- Acute Tubular NecrosisDokument38 SeitenAcute Tubular Necrosisganesa ekaNoch keine Bewertungen
- Acute Tubular NecrosisDokument60 SeitenAcute Tubular NecrosisYedesney C. LinaresNoch keine Bewertungen
- Care of The Patient With Renal and Urinary Disorders - HandoutDokument52 SeitenCare of The Patient With Renal and Urinary Disorders - HandoutAaron Ramirez LuNoch keine Bewertungen
- Article 1 PDFDokument4 SeitenArticle 1 PDFSally TareqNoch keine Bewertungen
- Renal Disease of Small AnimalsDokument46 SeitenRenal Disease of Small AnimalsTahir KasimNoch keine Bewertungen
- Discussion 1 NPNDokument53 SeitenDiscussion 1 NPNFaith TambongNoch keine Bewertungen
- Blood Urea Nitrogen: "BUN" Redirects Here. For Other Uses, SeeDokument4 SeitenBlood Urea Nitrogen: "BUN" Redirects Here. For Other Uses, Seeshikha_5j20062002Noch keine Bewertungen
- Renal Function TestsDokument43 SeitenRenal Function TestsAbdulelah MurshidNoch keine Bewertungen
- Obstruksi Uropati IrfanDokument43 SeitenObstruksi Uropati IrfanirfanNoch keine Bewertungen
- CC1 Lab Manual FinalDokument14 SeitenCC1 Lab Manual FinalMelody PardilloNoch keine Bewertungen
- Prevalence and Clinical Significance of The Medullary Rim Sign Identified On Ultrasound of Feline KidneysDokument7 SeitenPrevalence and Clinical Significance of The Medullary Rim Sign Identified On Ultrasound of Feline Kidneysantonio arteagaNoch keine Bewertungen
- Acute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidentDokument48 SeitenAcute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidenterikaNoch keine Bewertungen
- Non-Protein Nitrogen (NPN) CompoundsDokument34 SeitenNon-Protein Nitrogen (NPN) CompoundsAhmed GaberNoch keine Bewertungen