Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Note For SmvelDokument17 SeitenNote For SmvelKumaravel SubramaniamNoch keine Bewertungen
- Desktop Fitting Guide Target 6.0Dokument11 SeitenDesktop Fitting Guide Target 6.0Abdul BaseerNoch keine Bewertungen
- HTM 08-01Dokument48 SeitenHTM 08-01Benjamín AlainNoch keine Bewertungen
- Clinical Examination Techniques in OtologyDokument44 SeitenClinical Examination Techniques in OtologyDr. T. Balasubramanian100% (2)
- Research Brief 1 The Importance of Fingerspelling For ReadingDokument8 SeitenResearch Brief 1 The Importance of Fingerspelling For Readingapi-360938444Noch keine Bewertungen
- Congenital Cytomegalovirus Infection Management and OutcomeDokument20 SeitenCongenital Cytomegalovirus Infection Management and Outcomegomitas21Noch keine Bewertungen
- Seminar ON Sensory Deprevation: Prepared By: P.Manojkumar. MSC (N) 1St Yr, VmconDokument29 SeitenSeminar ON Sensory Deprevation: Prepared By: P.Manojkumar. MSC (N) 1St Yr, VmconManoj Bala0% (1)
- Nayeli Torres - Final Essay-2Dokument9 SeitenNayeli Torres - Final Essay-2api-609565848Noch keine Bewertungen
- Template For Clil Unit Plan For Teyl SensesDokument31 SeitenTemplate For Clil Unit Plan For Teyl SensesSonia Felipe MartínezNoch keine Bewertungen
- From The Mute God To The Lesser GodDokument16 SeitenFrom The Mute God To The Lesser GodefunctionNoch keine Bewertungen
- Lenire User Experience Group Study - Report 1 - Cohort Analysis 20200131 PDFDokument55 SeitenLenire User Experience Group Study - Report 1 - Cohort Analysis 20200131 PDFAshish JainNoch keine Bewertungen
- Children With DisabilityDokument89 SeitenChildren With DisabilityMariakatrinuuhNoch keine Bewertungen
- Sign Language With People Who Are DeafDokument10 SeitenSign Language With People Who Are DeafMs.Aishwarya Nallamuthu, Dept. of SLHS, SRIHERNoch keine Bewertungen
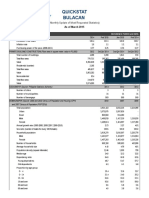
- Quickstat Bulacan: (Monthly Update of Most Requested Statistics)Dokument5 SeitenQuickstat Bulacan: (Monthly Update of Most Requested Statistics)ciryajamNoch keine Bewertungen
- Deaf Nondeaf Interpreter Teams and The C PDFDokument23 SeitenDeaf Nondeaf Interpreter Teams and The C PDFHelena Santiago VigataNoch keine Bewertungen
- Department of Empowerment of Persons With Disabilities (Divyangjan)Dokument31 SeitenDepartment of Empowerment of Persons With Disabilities (Divyangjan)Shabana AqilNoch keine Bewertungen
- Everybody Hates Noise PollutionDokument1 SeiteEverybody Hates Noise PollutionKeneth ValladaresNoch keine Bewertungen
- RS - EFs Cool en Niños Sordos (2022)Dokument16 SeitenRS - EFs Cool en Niños Sordos (2022)Tamara valverde garciaNoch keine Bewertungen
- Leiter-3 Appendix D New 2014Dokument6 SeitenLeiter-3 Appendix D New 2014Didenko MarinaNoch keine Bewertungen
- Ap Gramasachivalayam Village - Revenue - Officer - (GR - II)Dokument26 SeitenAp Gramasachivalayam Village - Revenue - Officer - (GR - II)ashNoch keine Bewertungen
- Simultaneous MaskingDokument58 SeitenSimultaneous MaskingbadshaolinNoch keine Bewertungen
- D 0116491 F Audibase 5 Operating ManualDokument76 SeitenD 0116491 F Audibase 5 Operating ManualRoa DanielNoch keine Bewertungen
- Bus Pass EligibilityDokument6 SeitenBus Pass EligibilityBilla Naganath0% (1)
- Oak Lodge SchoolDokument9 SeitenOak Lodge SchoolmarycballNoch keine Bewertungen
- Sped01 Task Sheets - Ac MalonzoDokument16 SeitenSped01 Task Sheets - Ac MalonzoAc MalonzoNoch keine Bewertungen
- Guide To Speech AudiometryDokument16 SeitenGuide To Speech Audiometrye_limantaraNoch keine Bewertungen
- Guidelines and Space Standards For Physically Disabled: Submitted byDokument32 SeitenGuidelines and Space Standards For Physically Disabled: Submitted byrenuNoch keine Bewertungen
- ENT Article - WuDokument29 SeitenENT Article - WuChang-Wei David HuangNoch keine Bewertungen
- 3-4 Micro PerspectiveDokument7 Seiten3-4 Micro PerspectiveJohnne Erika LarosaNoch keine Bewertungen
- Eisenson, 1968Dokument11 SeitenEisenson, 1968Cynthia Torres-GonzálezNoch keine Bewertungen