Beruflich Dokumente
Kultur Dokumente
CT Simulator (A Review)
Hochgeladen von
Wahyu WidhiantoOriginalbeschreibung:
Originaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
CT Simulator (A Review)
Hochgeladen von
Wahyu WidhiantoCopyright:
Verfügbare Formate
The British Journal of Radiology, 75 (2002), 937–949 E 2002 The British Institute of Radiology
Review article
CT simulation for radiotherapy treatment planning
1
E G A AIRD, MSc, PhD, FIPEM and 2J CONWAY, BSc, PhD, MIPEM
1
Medical Physics Department, Mount Vernon Hospital, Rickmansworth Road, Northwood, Middlesex
HA6 2RN and 2 Department of Radiotherapy Physics, Weston Park Hospital, Whitham Road, Sheffield
S10 2SJ, UK
Abstract. The present status of CT simulation (CT sim) hardware, software and practice is
reviewed, particularly with regard to the changes that have taken place over the last 5 years. The
latest technology is discussed together with some recently developed techniques. The article
concludes with a discussion of virtual simulation vs physical (conventional) simulation; in
particular there is a review of the changes that have been made to the ‘‘Disadvantages table’’
presented by Conway and Robinson [1], which now make CT sim an attractive system for any
radiotherapy department.
The demands of modern radiotherapy planning positron emission tomography. These comple-
are quite different from those 20 years ago. Clini- mentary modalities and their uses will not be
cians now require to define the target volume considered here. However, it is important for the
more precisely, not just in two dimensions, but reader to be aware of the potentials and pitfalls of
also in three dimensions. It has therefore become these imaging techniques in oncology and that,
necessary to visualize anatomy in three dimen- generally, they are co-registered to CT in order to
sions to enable planning to conform the dose maintain geometric accuracy on the computer
around the target volume in order to irradiate the three-dimensional (3D) image of the patient.
tumour to as high a dose as possible, whilst saving It is the intention of this article to review the
the normal tissues. In order to achieve this the place of CT simulation (CT sim) in radiotherapy
following tools are necessary: planning as it has developed since the article by
Conway and Robinson in 1997 [1].
N Identification of critical structures using
advanced anatomical and functional imaging
methods.
N Visualization of treatment targets with respect CT planning development
to other structures in three dimensions. When CT became available to radiotherapy
N Efficient and accurate outlining of tumour patients in the 1970s, its role in treatment plan-
using contouring tools. ning was very quickly recognized [2] since the
N Addition of symmetrical or asymmetrical transverse cross-sections produced are exactly the
volumetric margins. sections required for isodose charting. However, it
N Beam’s eye view (BEV) of targets and struc- has taken many years of development to realise
tures. the full impact that CT can have in treatment
N Shaping fields around the target. planning, since it has been necessary to wait for
N Adding beams together. rapid scanning and very rapid computing power
N Dose volume histogram (DVH) generation. to implement the most important aspects of CT
N Tools for optimizing plans using forward or planning and develop these into CT sim.
inverse interactive techniques. The transfer of planning information (reference
N Export of plan to linear accelerator. marks, field entry point etc.) from CT sim to the
N Monitor unit calculations. patient prior to treatment is the most critical
N Export of digitally reconstructed radiographs, step; without an accurate and reliable method of
(DDRs — see below) to an image database for doing this, the usefulness of CT planning is
on-line assessment of treatment accuracy. greatly reduced and, indeed, may introduce error.
Some identification of tumour will be achieved The practice of virtual simulation (VSIM) relies
with modalities other than CT, such as MRI and on this concept being realisable. The two main
elements of VSIM essential to its accuracy and
Received 24 September 2001 and in revised form 2 April verification of an individual patient’s treatment
2002, accepted 27 June 2002. are: transfer of coordinates (marks identifying
The British Journal of Radiology, December 2002 937
E G A Aird and J Conway
beam centres, field edges, block positions etc. as 60–80 kV radiograph (simulator film filter), high
necessary); and the construction of DDRs [3]. energy, to simulate 6 MV portal image (port film
Goitein and Abrams [4] and Goitein et al [5] filter), customizable filters (window/level map-
discussed the development of CT planning from a ping) and special techniques, e.g. depth control/
system performing ‘‘almost none of the functions depth shading. Depth control or depth shading is
associated with a treatment simulator’’ to a sys- the reconstruction of a DRR for a limited range
tem where ‘‘the simulation of treatment by the of depths (a region of interest defined by the user)
computer can be much more comprehensive in which, say, the target lies. This produces an
and valuable’’. Goitein et al [5] developed the image that is very useful for checking margins. It is
concept of beam’s eye view (BEV) following superior to a conventional radiograph, particu-
the idea of McShan et al [6], and recognized the larly if bone overlies the region of interest.
importance of projecting through CT sections to A key feature to the efficient use of CT sim is
produce an image for verification purposes. It the speed of reconstruction of DRR. This used to
was, however, Sherouse et al [7] and Sherouse take a minute or more, however, it is now possible
and Chaney [8] who first used the terms virtual to move a beam and have the new DRR recal-
simulation and virtual simulator, and the concept culated and displayed almost in real time.
of the DRR was further developed by Sherouse Another feature of CT planning and VSIM
et al [9]. The DRR ‘‘traces rays from the X-ray recognized by early workers in this field was the
source through a 3-dimensional model of the use of non-coplanar beams [10]. These beams
patient made up of voxels determined from CT were already in use to treat patients, but verifi-
scans’’ [9]. This particular DRR software also cation using imaging could not generally be
separated photoelectron and Compton compo- achieved. The size of the image intensifier on
nents in order to compute either a DRR similar to the simulator often prevented positioning of the
a verification image on the simulator or a DRR beam with the correct geometry with respect to
that looked more like the high-energy portal the target and the patient. The image was also
difficult to interpret. Both of these problems could
radiograph taken on the linear accelerator. These
be overcome in VSIM. In particular, interpreta-
different images are produced using different
tion of the image became possible since not only
image processing techniques in the modern virtual
could it be processed to improve the quality of the
simulator.
image, but by looking at the set of transverse
Processing the DRR, particularly the use of
sections, it was possible to see the various organs
various types of filter to change the appearance of
and structures covered by the beam.
the image, is now considered to be a major asset
of VSIM. More information can be visualized
than in conventional radiography, even if some
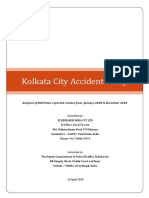
Specification of a CT simulator
detail is lost in the digital nature of the image with
(Figure 1)
its finite number of pixels (typically 5126512). The term CT sim is associated with ‘‘virtual
Standard filters include low energy, to simulate a simulation’’, a term coined by Sherouse et al [7] to
Laser system
CT
control
CT SIMULATOR
VIRTUAL SIMULATION
PLAN WORKSTATIONS
• Contouring
3D-RTP
• Virtual Fluoroscopy
• DRR Calculation
• Plan
optimization • Beam design
• Dose • Connectivity
IMAGE • Co-ordinate transfer to
calculation
• Connectivity laser system
RT IMAGE
DATABASE
Figure 1. Schematic of CT simulator
• SIM
• DRR and associated systems. DRR, digi-
• EPI tally reconstructed radiograph; EPI,
• CT
• MRI
electronic portal imaging; PET, posi-
• PET tron emmission tomography; RTP,
radiotherapy treatment planning.
938 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
refer to the processes on a computer, using a 3D
CT patient data set, that allow full simulation and
verification of radiotherapy treatment. CT Sim5
physical CT scanning (patient required)+VSIM
(patient not required). The main item of equip-
ment needed is a CT scanner connected to a com-
puter containing a suite of programmes that allow
all the processes outlined above to be performed,
including virtual modelling of the radiotherapy
simulator process together with advanced DRR
production (many of these features of VSIM are
now built into the treatment planning system),
with the addition of moveable lasers driven under
computer control.
Specification of a typical CT scanner Figure 2. Large bore (85 cm physical aperture) oncol-
ogy CT scanner showing breast patient positioning
Table 1 shows the main features of a typical (photo reproduced by permission of Phillips Medical
CT scanner. The dedicated Philips AcQsim CT Systems).
scanner (Philips Medical Systems Ltd, Stevenage,
UK) (Figure 2), has some features that differ marking not just the centres of beams from any
slightly from those in Table 1. In particular, since direction, but also the field edges of irregular
it is a fourth generation scanner, it has a complete fields. This laser feature is an important addition,
ring of 2400 detectors, aperture is 85 cm and but does not need to be built into the CT scanner
minimum slice width is 2 mm. as in some of the early CT sims. This feature is
One of the other features installed by several now normally installed as a set of orthogonal
workers [11, 12] is a laser on the same rotating lasers mounted on the walls and ceiling of the
arm as the X-ray set, with the potential for room, or on a special rigid gantry. The ceiling
laser (sagittal line) must be able to move laterally
Table 1. Main features of a typical CT scanner
under computer control to allow the isocentre for
Feature Specification a particular plan to be marked; on some systems
it is also possible to move the other lasers to
Aperture At least 70 cm (see below)
Number of detectors 672–896 per row define the isocentre completely, instead of relying
X-ray tube 80–130 kV; 250 to 500 mA on longitudinal and vertical movement of the CT
depending on kV couch.
(typically 50–60 kW)
Heat capacity 6–7 MHU Virtual simulator software
Anode heat cooling 700–900 kHU min21
Minimum slice width 1 mm The most important features of the virtual
Patient support Table top identical to that simulator are fast CT scanning and reconstruction
used on treatment machine of transverse slices, fast reconstruction of any
Spatial resolution High Contrast: better than
13 line pairs cm21 (at section, automatic skin outlining, automatic lung/
0% MTF) bone outlining, semi-automatic outlining of cri-
Low contrast: 5 mm at 3% tical structures/vital organs, user friendly target
resolution outlining (accurate interpolation/ease of editing)
Acquisition time 1–2 slice/rev s21 (multislice and volumetric growing of margins using a true
4 or 8 slice/rev s21)
Covering a width of 3D volume growing algorithm.
20–32 mm at isocentre It should not be necessary to outline all features
Reconstruction time Few seconds up to 60 s total on all slices; interpolation is possible provided
time to end of 30 mm slice that the user does not leave too many gaps for the
Virtual simulation computer to fill in. Outlining the tumour volume,
DRR calculation Few seconds (tolerable),
sub-second (desirable) usually the gross tumour volume (GTV), is the
Capacity to store 12 000–60 000 uncompressed clinician’s responsibility. Again, some degree of
images on hard disc interpolation is possible provided that the con-
Laser accuracy ¡1 mm tours on the interpolated slices are checked for
Accuracy of ,1 mm accuracy. Methods of linear and non-linear
slice location
contour interpolation are combined with manual
DRR, digitally reconstructed radiograph; MHU, mega heat slice-by-slice checking and editing. The treatment
units; MTF, modulation transfer function. planner then grows the GTV to the planning
The British Journal of Radiology, December 2002 939
E G A Aird and J Conway
target volume (PTV) by a true 3D volume grow- Dedicated CT?
ing algorithm [13]; many planning systems now
The special requirements of a CT simulator
allow for different margins to be added in
suggest that a dedicated CT scanner designed to
different directions.
fit the demands of radiotherapy planning on CT is
3D display systems are continually improving.
required. However, many centres will also wish
These are vital features to any virtual simulator
to use their CT simulator for diagnostic work. As
since internal anatomy, beam geometry and dose
diagnostic scanners are developed for purposes
distributions need to be easily and accurately
other than radiotherapy, we may see a divergence
displayed and manipulated quickly. It is especially
in development between the two types of equip-
important that the PTV is seen by the planner in
three dimensions to be covered by the high dose ment. Each centre will need to specify its own
region and, conversely, that critical structures and requirements, provided that the computer net-
vital organs are in low dose regions. Of course, work connections can be made so that any CT
other tools within the planning system, e.g. dose– scanner can be linked to a computer with its
volume histograms (DVHs), assist this process, virtual simulator package (see below), with the
but generally these do not contain the geometrical need also to add a laser marking-up system.
and anatomical information given in the image
display. Several commercial systems offer addi-
tional features within their VSIM package, such Immobilization
as a virtual light field, which illuminates the skin
surface of the 3D image of the patient. Most sys- The importance of effective positioning of the
tems also have an image of the treatment machine patient to facilitate optimum treatment design and
together with a picture of the patient on the treat- the ability to re-establish this position on a daily
ment table. The gantry and table will move to basis are recognized as essential to accurate radio-
show the position of the beam chosen and par- therapy. Some of the early work [9] with CT sim
ticularly whether there is any possibility of a emphasized the difficulties of emulating the
collision. patient support and accessory attachments of a
linear accelerator on a CT scanner. After 10 years
of CT sim use, manufacturers have recognized the
Other aspects of CT sim need to provide a table top that is identical to the
top used on the treatment machine (previously it
Multislice CT scanners was standard practice to provide a flat-top couch
As multislice CT scanners become more insert to the conventional curved CT diagnostic
common in diagnostic radiology it will be impor- couch that could easily rotate slightly so that the
tant for the radiotherapy community to assess patient was no longer on a horizontal surface).
their role for VSIM. One issue is that of speed. An The CT therapy couch top should also be
8-slice scanner can scan 48 cm in 3–6 s at 1 cm slice designed to take the usual accessories needed to
width, or 48 cm in 15–30 s at 2 mm slice width. position the patient, for example breast boards
With older systems these times would nominally and head rests. These accessories significantly
be approximately eight times longer (the latter enhance positioning accuracy and patient comfort
time, at least 240 s, would require pauses for and reduce patient set-up time.
anode cooling, or would not be attempted).
Fast scan times are advantageous in reducing
motion artefacts, but there will be a question as to Aperture
which phase of breathing has been scanned. With
the older single slice systems there is some blur- The constraints of a 70 cm aperture on radio-
ring of images owing to patient movement. This therapy patient positioning are obvious for some
has been accepted since the patient is treated with treatments, such as breast and mantle techniques.
beam-on times similar to CT scanning times, and The move to more dedicated oncology CT scan-
it has been assumed that any effects of movement ners has led to designs that can accommodate
would be averaged out. However, now that more these set ups using a larger aperture. One com-
centres are beginning to address the problem of mercial system is available, the Marconi AcQsim
motion, both on the CT scanner and on treat- CT Scanner (Philips Medical Systems Ltd,
ment, the faster scanners may be an enormous Stevenage, UK), with an aperture of 85 cm
advantage. (Figure 2). At the present time, potential purcha-
Multislice scanners will also need to be assessed sers wishing to decide which system to choose
for their accuracy since the off-axis slices need will need to explore the compromise that has to
to be reconstructed from ray paths travelling be made between aperture size and image quality
obliquely through the patient. and the possible need to modify set-up techniques.
940 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
Display systems the typical features for conventional and
conformal planning include:
A modern virtual simulator system will have
many options to display all the required features N beam position/rapid editing of position, size,
in colour/colour wash/line drawing, or to remove wedge, weight;
features as required. It is usually possible to view N adding further beams using copy/position
all sections, namely axial, coronal or sagittal, in facilities;
multiple windows on the same computer page. N auto-beam positions according to a stored
Other features will include 3D views with appro- protocol (beam configuration library);
priate CT slices superimposed and rotation of the N auto-shaping for the multileaf collimator/
3D view. blocks including optimization of collimator
angle;
CT sim to radiotherapy treatment planning
N accurate 3D calculation of dose from each
beam using a complex dose calculation algo-
system connectivity rithm, taking 3D scatter and inhomogeneities
The importance of efficient and accurate into account;
connectivity between CT sim and radiotherapy N display of complete dose distribution; and
treatment planning system (RTPS) radiotherapy N calculation of monitor units for each beam.
treatment planning systen cannot be over-
emphasized. Many of the problems associated with
having two separate computer systems, one CT sim/VSIM process
providing the function of a simulator and the
other providing a dose calculation engine, are due General
to theincompatibilities between common para- This process may vary depending on local
meter transfer protocols. Standards such as procedures adopted to suit the working conditions
Digital Imaging and Communications in Medicine of a particular department. The ultimate aim is to
DICOMv3, and the standard image transfer achieve the same level of treatment simulation as
protocol for radiotherapy (DICOM-RT) can be conventional physical methods but with the added
highly complex to implement and can vary in features that are available from 3D visualization.
interpretation. The advent of DICOM-RT enables Significant advantage is gained through the
export of radiotherapy images, treatment plans reduced visits required by the patient and the
and structure sets (contours). However, this flexibility offered through tasks, such as contour
standard is not always fully implemented and marking, that can be undertaken after the patient
can have exclusions, e.g. dynamic treatment data, has left.
that can limit functionality. Problems may be A general discussion of the CT VSIM process
encountered when transferring data, even between follows, with an indication of alternative methods
systems from the same manufacturer. Transfer and options where appropriate.
protocols should be fully tested for all conditions The patient is positioned on the flat-top couch
and any inconsistencies reported. of a CT scanner in the treatment position. Align-
Most CT sim systems are configured as single ment of the patient is made with lateral wall lasers
virtual simulator workstations interfaced to a CT and sagittal laser. Opaque catheters may be used
scanner. Problems arise when additional VSIM as visual markers. A prior simulator visit is not
stations are added to accommodate increased usually required. A pilot (scout view) scan is made
workload, with multiple copies of patient data to determine the region over which axial slices
and lack of synchronization between these files. will be scanned. These slices are then made
Future systems must incorporate patient images, according to the particular protocol for the site
structures and treatment files in a database that to be treated, e.g. prostate. A single visit to the
enables multi-user access with full data protec- CT simulator is usually preferred. Two methods
tion, e.g. file locked while in use to avoid can be adopted. The first requires the oncologist
secondary access. to be present to identify the target volume and
isocentre from the scan information while the
patient remains in the treatment position. In the
Treatment charting (dosimetry)
second method the operator identifies a reference
Modern VSIM software packages also contain slice containing a reference point from the scan
many of the features of a treatment planning study and target definition is then undertaken
system, with the exception of the calculation of when the oncologist is available. In both methods
dose distribution. Correspondingly, modern treat- the patient is ‘‘marked’’ where the laser projection
ment planning systems are now available with illuminates the skin and finally the patient is
VSIM software. For VSIM or treatment planning removed from the couch. In the second method
The British Journal of Radiology, December 2002 941
E G A Aird and J Conway
Figure 3. Localization: a suitable ‘‘patient origin’’ (isocentre) is marked as the centre of the purple triangle (mark-
up). These coordinates are sent to the laser system and the patient marked. All plan isocentres are related to this
mark in terms of ‘‘shift coordinates’’.
the isocentre is eventually defined in terms of lated in real time (Figure 4) for all the beams that
‘‘shift coordinates from the reference point’’ will be used at portal verification on the accel-
(Figure 3). erator. In some cases, e.g. prostate, only anterior
The remaining parts of the VSIM process and lateral beam DRRs are necessary to allow
depend on whether beam calculation is required. effective reconciliation with film or electronic
Dose calculation will usually be undertaken by a portal imaging device portal images.
system designed with a high quality beam model. In some situations the patient may have to
The data from the virtual simulator must be return to the conventional simulator. Examples
accurately and seamlessly transferred to this are where the staff at a centre are not sufficiently
system and eventually returned to the virtual confident with CT VSIM; VSIM cannot demon-
simulator for verification. Some planning systems strate definitely that the fields that have been
may be capable of producing high resolution chosen can be given by the particular treatment
DRRs that may negate this return process. Plans machine; the DRRs are not sufficiently good com-
that do not require dose calculation, such as pared with conventional simulator images; and
simple parallel pairs, can have their plan optim- problems with the patient’s treatment cannot be
ization and verification achieved by the virtual resolved using virtual methods that would neces-
simulator. Many of these plan optimization tools sitate a repeat CT scan.
are features of most planning systems. In the early
stages of implementing CT VSIM, some centres
may wish to continue with physical simulation Examples of CT sim practice
until confident of the accuracy of the process. The CT sim process depends on defining a
This will necessitate another patient session prior relationship between the CT image coordinates
to treatment but may avoid problems when com- (patient) and the treatment coordinates (machine)
mencing treatment with the inevitable impact on that allows a precise transformation from the
machine throughput. DRRs can usually be calcu- localization setup to radiotherapy treatment
942 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
Figure 4. Verification: the ‘‘shift coordinates’’ represent the relationship between the isocentre and the ‘‘patient
marked origin’’ to be used for treatment setup. All field digitally reconstructed radiographs are exported for
portal verification on the linear accelerator.
coordinate space. The methods of achieving this design of the board. Use of large aperture CT
are dependent on local equipment and working will allow more flexibility in patient positioning.
practices. Inherent in all successful CT sim The scan protocol is typically a slice thickness
techniques is the appropriate immobilization of of 5 mm with a spiral pitch of 1.5, which will
the patient that is compatible with the constraints give 50–60 slices in the study. Slice parameters
of the CT scanner. For some sites radiotherapy set larger than this may result in poor DRRs.
techniques will have to be adapted to accommo- Movement of the chest during slice acquisition
date these constraints. can also result in visible discontinuities in sagittal
Successful CT sim practice will require changes reconstruction.
to working practice that will allow similar patient Radio-opaque catheters can be used to mark
throughput to a conventional simulator. This superior, inferior, medial and lateral extents of
may require flexible working of the oncologists the volume. The patient is scanned to include
involved in defining treatment volumes. The superior and inferior extents (from the pilot scan)
advantages of CT sim over conventional simula- and external contouring of those slices contain-
tion, such as one planning session visit for the ing the catheters are performed (purple lines in
patient, volume mark-up without the patient Figure 5a).
present and minimal patient wait, can only be A reference mark is set to the medial catheter
realised if working practice is tailored to the on the central slice, midway between the superior
system. and inferior marked slices, and this is defined as
The following is a discussion about some site- the ‘‘patient origin’’. The patient is marked using
specific CT sim procedures. the patient origin coordinates transferred to the
CT sim couch and lasers. The patient session is
Breast (Figure 5a) now finished.
Stage 1. Localization is usually undertaken Stage 2. VSIM planning requires the glanc-
with the patient positioned on a purpose designed ing fields to be positioned in BEV so that the
‘‘breast board’’. The patient’s arms must not posterior field edges pass through the medial and
impede free movement of the CT couch and lateral catheters. Adjustments are made to mini-
therefore careful thought must be given to the mize encompassed lung, this can be visualized by
The British Journal of Radiology, December 2002 943
E G A Aird and J Conway
Figure 5. (a) Virtual simulation planning of tangential breast fields. Collimator and table angle to provide match-
ing borders are obtained from multiple window views.
altering the CT window and level for lung and order to emulate exactly the patient positioning
soft tissues. Field parameters are selected accord- on the treatment machine. Careful consideration
ing to the breast protocol to be used and the plan should be given to the design of the head fixation
is passed to the RTPS for calculation and dose device to enable compatibility between the CT
optimization. The plan, including the final iso- and accelerator table supports.
centre coordinates, which may have changed The scanning parameters are usually a trade-
during plan optimization, is exported back to off between maximizing DRR resolution and
the virtual simulator for verification using DRRs. keeping the number of slices to a manageable
The shift coordinates are printed from the size (typically 3 mm slice thickness and 1.5 spiral
relationship between the plan isocentre and pitch). The scanning extent is determined from the
patient origin coordinates. These are transferred pilot (scout) view and the external contours are
to the treatment machine with the plan details. often produced at a remote VSIM workstation
Worksheets and DRRs are printed [14, 15]. while previewing the scanned slices.
A reference slice plane is selected (purple
Head and neck (Figure 5b) contour in Figure 5b) and the patient origin
Stage 1. Localization requires the immobiliza- coordinates created and transferred to the CT
tion shell to be attached to the flat CT couch in couch and laser. The CT longitudinal couch,
944 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
Figure 5. (b) Virtual verification of a carcinoma of the tongue. The purple triangle represents the plane containing
the ‘‘patient origin’’ reference point from which the position of the isocentre gives the ‘‘shift coordinates’’.
vertical couch and sagittal laser positions are set Bronchus (Figure 5c)
to define the patient origin, and the patient is Stage 1. Localization of the patient is in
marked. The patient session is now finished. the supine position with arms overhead clasping
Stage 2. VSIM requires marking of the GTV, arm-poles attached to an indexed radiotherapy
CTV, PTV and organs at risk. The isocentre and couch top. The scan length is customized for each
field parameters can then be defined using the patient by visual inspection within the CT aper-
virtual simulator or the RTPS. The plan is sent ture and from the pilot (scout) view, but generally
for calculation and optimization to the RTPS and covers the whole chest. The scan protocol is the
exported back to the virtual simulator for same as for the breast. Localization and planning
verification. The DRRs for all fields are printed procedures are similar to those used for head and
(laser imager) and approved by the oncologist. neck with the exception of palliative bronchus
Shift coordinates are printed from the relation- treatments. For these cases the definition of field
ship between the isocentre and patient origin size position and shielding can be performed by
coordinates. These are transferred to the treat- direct marking of the DRRs, being analogous to
ment machine with the plan details. Worksheets conventional physical simulation. This technique
and DRRs are printed (Figure 5b) [16]. has been termed ‘‘virtual fluoroscopy’’ [17]. The
The British Journal of Radiology, December 2002 945
E G A Aird and J Conway
Figure 5. (c) Localization of a chest lesion using virtual fluoroscopy. Anteroposterior and lateral virtual radio-
graphs (digitally reconstructed radiographs) show the isocentre in simulator and CT views.
effect of diaphragm movement in these cases, Table 2. Acceptance tests for CT sim
which cannot be easily assessed by CT sim, must
Parameter Acceptance Tolerance
be allowed for in the target margins, if a breath test
hold protocol is not used.
Target Contouring ,1 pixel
localization accuracy
Isocentre
Quality assurance for CT sim calculation
DRR Divergence Ray-line angular
The accuracy of a conventional simulator relies accuracy test displacement 0.1 ˚
on the very tight tolerances of several mechanical
features, including gantry, collimator and field DDR, digitally reconstructed radiograph.
wires. In contrast, CT sim is highly dependent on
the accuracy of the image from the CT scanner links between systems are particularly important
and alignment of the supporting hardware. It is during commissioning and following software
still vital to perform geometric tests of the laser revision.
system, couch alignment and mechanical toler- The quality control procedures can be split
ances under load. Checks of the various network into daily and monthly procedures and those
946 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
performed at acceptance and then yearly. Accep- in set-up errors between the two techniques and
tance tests are shown in Table 2 [18]. Special concluded that physical verification could be
phantoms to perform these tests have been omitted from the CT-based planning process.
designed [19]. McJury et al [21] considered 86 patients under-
Daily tests should include the following laser going palliative radiotherapy using parallel-
tests to ensure that all positions and distances are opposed fields to the chest, all patients had CT
within ¡1 mm: VSIM and physical simulation but patients in
each group of the study received treatment using
N Alignment of external vertical and horizontal
either the CT sim or physical simulation plan.
lasers and their position with respect to the
virtual isocentre of the CT simulator. Results indicated that setup errors were typically
N Accuracy and linearity of the sagittal laser, 2–3 mm for both patient groups and there were
no significant differences in terms of accuracy.
driven by computer or manually set.
N Alignment of the internal laser within CT (b) Do VSIM methods result in significant
differences in target volume definition compared
aperture with respect to the scan plane.
N Couch position, vertical and longitudinal, with physical simulation? The primary objective of
this double-blind randomized trial by McJury et
registration.
al [21] was to determine the differences in target
Monthly tests, or following software upgrade, volumes contoured using both techniques. Com-
should include the following: paring fields defined in each study arm, there was a
N Distance between known points in the image major or complete mismatch in coverage between
plane. fields in 70% of cases. The use of VSIM resulted
N Left/right registration. in field sizes on average 25% smaller than physical
N CT number/electron density verification. simulation. Senan et al [22] also found that the
N Noise on CT number in uniform phantom. use of CT sim allowed for smaller planning target
N Reconstructed slice location. volumes in radical lung cancer.
N Image transfer protocols, e.g. Dicom-RT, (c) Does VSIM cause problems with regard to
using standard plans. patient throughput owing to changes in length of
procedure times? Comparing the relative time
expended for CT sim and physical simulation
requires an assessment of procedure time invol-
Which to choose: CT sim or physical ving the patient and radiotherapy staff. A number
simulation? of centres have published data on time compar-
isons. Buchali et al [23] have reported a study of
Although attempting to replicate the same task,
conventional and virtual simulators are very 23 patients having tangential breast irradiation.
different systems with major differences in hard- The use of CT sim resulted in a mean saving of
ware. Most significantly, VSIM has a different 22 min in the whole treatment planning process
approach to providing the clinician with inform- compared with physical simulation. This reduced
ation to define the target volume, which can the time interval between CT and first treatment
result in significantly different treatments (beam by 31%, mainly due to the omission of conven-
arrangements and target volumes). tional simulator verification from the 3D planning
A comparison of virtual vs physical simulation process. For those centres with increasing patient
aims at answering a number of questions. The workloads, this economy can have a significant
answers to these questions are fundamental to deci- effect on patient throughput. However, a check by
sions on equipment selection when either replac- the physician is still required.
ing an existing simulator or providing additional Raga et al [24] have reported that the phy-
resources. Each question will be addressed based sician’s time involved in the planning process can
on published investigations and according to the be significantly reduced using CT sim, typically
authors’ own experiences and opinions. from 25 min to 5 min per patient (brain and
(a) Do VSIM methods lead to the same level of prostate).
treatment accuracy as physical simulation? Two Mah et al [25] used CT sim for craniospinal
recent randomised trials have compared simula- paediatric patients, where time efficiency can
tion techniques. 75 patients undergoing four- improve patient comfort and increase accuracy.
field conformal prostate treatment in a study by On average patient involvement and immobiliza-
Valicenti et al [20] had CT sim, with one group tion time during simulation could be reduced
having physical simulation prior to treatment. from 45 min to 20 min when using CT sim instead
Both patient groups had their port films reviewed of physical simulation.
to quantify the differences between the two tech- These results suggest that the use of CT sim
niques. Results indicated no significant difference with omission of conventional simulation may
The British Journal of Radiology, December 2002 947
E G A Aird and J Conway
improve the efficiency of the treatment planning Advantages and disadvantages
process without compromizing accuracy. Raga
Many of the advantages of CT sim have been
et al [24] report that 60% of their planned patients
discussed in the preceding sections but can be
were suitable for CT sim, whereas some early
summarized as:
work by Nagata et al [26] indicated that this
figure could be as high as 70%. One author’s (JC) N full 3D simulation allowing unique verifica-
own experience indicates that 65% of planned tion of beam coverage and avoidance in three
patients are selected for CT sim. dimensions,
N beams can be simulated and verified that are
not possible with conventional simulation, e.g.
Table 3. Disadvantages of CT simulation [1] vertex fields,
Disadvantage Comment N the verification images, DRRs can contain
more information than conventional simula-
1. A large number of Now easily and quickly tion and can be manipulated to enhance
CT slices are often achievable. Sometimes
required at ¡3 mm 5 mm slices are
tumour visualization, and
thickness …..for unavoidable where N there is a much closer connection to diagnostic
optimal DRR large volumes are to information with CT sim, allowing integration
resolution. be scanned. of multimodality images.
2. State-of-the-art Now achieved.
hardware is required When examining the disadvantages of CT sim,
for interactive it is interesting to use the table from Conway and
capabilities. Robinson, 1997 [1], which probably represented
3. DRRs do not provide This can be resolved
information about partially by multiple the state-of-the-art in CT-sim 1 or 2 years earlier,
patient movement or fast scans that can be as a point of comparison with the present
anatomical movement registered at different situation (Table 3).
that may be necessary breath hold positions
for accurate field or slow scanning to
coverage. blur movements and
registration with Conclusion
fast scans.
4. DRR resolution is Resolution now Modern CT sim allows full 3D viewing and
unlikely to equal entirely acceptable planning of the patient, together with verification
radiographic film for most uses.
resolution. images that can be used for comparison with
5. Field portal Now available on many portal images.
visualisation on systems using room’s The entire simulation of the patient, ensuring
the patient’s skin eye view. all beams are achievable and safe, makes use of
not available.
room’s eye view and anti-collision software
6. Patients may have to Scan times are now very
be immobilised for much shorter and algorithms.
extended periods planning methods can CT sim enables doctors and dosimetrists to
during the virtual be adapted to reduce work at their convenience while minimizing
simulation procedure. the requirement for patient attendance. However, for some palliative
the patient’s physical
presence. treatments the planning process using CT sim
7. The radiotherapist Still true, but procedure might be prolonged compared with physical
needs to be present now speeded up with simulation.
for extended periods effective editing The adoption of CT VSIM in favour of con-
to mark target systems. Mark-up can ventional simulation is recommended where small
volume. be done post-scan
and utilise reference oncology departments have a requirement for
marking only. only one simulator while expanding their 3D
8. Correcting (shifts) to Still true and still a treatment planning methods. For larger depart-
the marked isocentre concern in terms ments the retention of conventional simulation
may be required before of the potential for
the plan is finalized. error. Portal imaging would seem advantageous, and a ratio of two CT
on the treatment set sim units to one physical simulation unit would
provides final check; provide the balance of resources for the precision
this step becomes required in a modern radiotherapy department.
more important.
9. Some patient positions Still true, but dedicated
may not be possible. CT scanners with
large apertures may References
eliminate this problem.
1. Conway J, Robinson MH. CT virtual simulation.
DRR, digitally reconstructed radiograph. Br J Radiol 1997;70(Suppl.):S106–18.
948 The British Journal of Radiology, December 2002
Review article: CT sim for radiotherapy treatment planning
2. Dobbs HJ, Parker RP. The respective roles of the 18. McGee KP, Das IJ. Commissioning, acceptance
simulator and computed tomography in radio- testing and quality assurance of a CT simulator. In:
therapy planning: a review. Clin Radiol 1984; Coia LR, Schultheiss TE, Hanks GE. A Practical
35:433–9. Guide to CT Simulation. Madison, WI: Advanced
3. Cheng CW, Chin LM, Kijewski PK. A coordinate Medical Publishing, 1995:5–23.
transfer of anatomical information from CT to 19. Craig TC, Brochu D, Van Dyk J. A quality
treatment simulation. Int J Radiat Oncol Biol Phys assurance phantom for three-dimensional radiation
1987;13:1559–69. treatment planning. Int J radiat Oncol Biol Phys
4. Goitein M, Abrams M. Multi-dimensional treat- 1999;44:955–66.
ment planning: 1. Delineation of anatomy. Int J 20. Valicenti RK, Waterman FM, Corn BW, Curran
Radiat Oncol Biol Phys 1983;9:777–87. WJ. A prospective, randomized study addressing
5. Goitein M, Abrams M, Rowell D, Pollari H, Wiles the need for physical simulation following virtual
J. Multi-dimensional treatment planning: II. Beam’s simulation. Int J Radiat Oncol Biol Phys 1997;
eye view, back projection, and projection through 39:1131–5.
CT sections. Int J Radiat Oncol Biol Phys 1983; 21. McJury M, Fisher PM, Pledge S, Brown G,
9:789–97. Anthony C, Hatton MQ, et al. The impact of
6. McShan DL, Silverman A, Lanza D, Reinstein L, virtual simulation in palliative radiotherapy for
Glicksman A. Three dimensional radiation treat- non-small cell lung cancer. Radiother Oncol
ment planning and dose display utilizing interactive 2001;59:311–8.
colorgraphics. Br J Radiol 1979;52:478–81. 22. Senan S, van Sornsen de Kose J, de Boer J, et al.
7. Sherouse GW, Mosher CE, Novins KL, The use of CT simulation in digitally reconstructed
Rosenmann JG, Chaney EL. Virtual simulation: radiographs (DRRs) in set-up verification allows for
concept and implementation. In: Bruinvis IAD, van
smaller planning target volumes in lung cancer.
der Giessen PH, van Kleffens HJ, Wittkamper FW
Lung Cancer 2000;20(Suppl 1):162.
(editors). Ninth International Conference on the
23. Buchali A, Geismar D, Hinkelbein M, Schlenger L,
Use of Computers in Radiation Therapy.
Zinner K, Budach V. Virtual simulation in patients
Amsterdam, The Netherlands: North Holland
with breast cancer. Radiother Oncol 2001;59:
Publishing Co., 1987:433–6.
267–72.
8. Sherouse GW, Chaney EL. The portable virtual
24. Raga DP, Forman JD, He T, Mesina CF. Clinical
simulator. Int J Radiat Oncol Biol Phys 1991;
21:475–81. results of computerised tomography-based simula-
9. Sherouse GW, Novins KL, Chaney EL. Com- tion with laser patient marking. Int J Radiat Oncol
putation of digitally reconstructed radiographs Biol Phys 1996;34:691–5.
for use in radiotherapy treatment design. Int J 25. Mah K, Danjoux CE, Manship S, Makhani N,
Radiat Oncol Biol Phys 1990;18:651–8. Cardosos M, Sixel KE. Computed tomographic
10. Mohan R. 3-D radiation treatment planning. Int J simulation of craniospinal fields in paediatric
Radiat Oncol Biol Phys 1988;15:481–95. patients: improved treatment accuracy and patient
11. Galvin J, Heidtman B, Cheng E, Block P, comfort. Int J Radiat Oncol Biol Phys 1998;41:
Goodman R. The use of a CT scanner specially 997–1003.
designed to perform the function of a radiation 26. Nagata Y, Nishidai T, Abe M, Takahashi M,
therapy treatment unit simulator. Med Phys Okajima K, Yamaoka N, et al. CT simulator: a new
1982;9:615. 3-D planning and simulating system for radio-
12. Nishidai T, Nagata Y, Takahashi M, Abe M, therapy: Part 2. Clinical application. Int J Radiat
Yamaoka N, Ishoihara H, et al. CT simulator: a Oncol Biol Phys 1990;18:505–13.
new 3-D planning and simulating system for
radiotherapy: Part 1. Description of system. Int J
Radiat Oncol Biol Phys 1990;18:499–504.
13. Neal AJ, Sivewright G, Bently R. Evaluation of a Futher reading
region growing algorithm for segmenting pelvic CT
images during radiotherapy planning. Br J Radiol 1. Van Dyk J, Taylor JS. CT simulators. Van Dyk J
1994;67:392–5. (editor). The Modern Technology of Radiation
14. Butker EK, Helton DJ, Keller JW, Hughes LL, Oncology. Madison, WI: Medical Physics Publishing,
Crenshaw T, Davis LW. A totally integrated simu- 1999.
lation technique for three-field breast treatment 2. Galvin JM. The CT-simulator and the Simulator-
using a CT simulator. Med Phys 1996;23:1809–14. CT: advantages, disadvantages and future develop-
15. Das IJ, Cheng EC, Freedman G, Fowble B. Lung ments. Smith AR (editor). Radiation Therapy
and heart dose volume analyses with CT simulator Physics. Berlin, Heidelberg, New York: Springer
in radiation treatment of breast cancer. Int J Radiat Verlag, 1995:19–32.
Oncol Biol Phys 1998;42:11–9. 3. Petschen I, Perez-Calatayud J, Tormo A, Lliso F,
16. Lohr F, Schramm O, Schraube P, et al. Simulation Badel MD, Caromona V, et al. Virtual Simulation
of 3D-treatment plans in head and neck tumor in radiation therapy planning. Report of five-year
aided by matching of digitally reconstructed radio- experience. Revista de Oncologia 2000;2:213–22.
graphs (DRR) and on-line distortion corrected 4. Coia LW, Schultheiss TE, Hanks GE (editors). A
simulator images. Radiother Oncol 1997;39:1131–5. Practical Guide to CT Simulation. Madison, WI:
17. Forster KM. The use of spiral CT to access Advanced Medical Publishing, 1995.
internal-motion target volume margins for thoracic
and abdominal tumour. 7th annual Oncology
Symposium, Boston 2000.
The British Journal of Radiology, December 2002 949
Das könnte Ihnen auch gefallen
- Learn C++ Programming LanguageDokument322 SeitenLearn C++ Programming LanguageAli Eb100% (8)
- Skin Reaction in RadiotherapyDokument3 SeitenSkin Reaction in RadiotherapyAhmad DiabNoch keine Bewertungen
- Augmented FeedbackDokument54 SeitenAugmented FeedbackAhmad KhuwarizmyNoch keine Bewertungen
- Radiology PDFDokument81 SeitenRadiology PDFrawaNoch keine Bewertungen
- MRI Safety Guidelines V2Dokument36 SeitenMRI Safety Guidelines V2perapanNoch keine Bewertungen
- Magnetic Resonance Imaging: Physical PrinciplesDokument35 SeitenMagnetic Resonance Imaging: Physical PrinciplesBERVIN KINGSNoch keine Bewertungen
- Diagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoireDokument5 SeitenDiagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoiretheijesNoch keine Bewertungen
- MRI Safety Study GuideDokument49 SeitenMRI Safety Study GuideJeremiah A.Noch keine Bewertungen
- Chapter 15 Special Techniques PDFDokument259 SeitenChapter 15 Special Techniques PDFSrinivas VenkataramanNoch keine Bewertungen
- Cell Survival Curve 2Dokument16 SeitenCell Survival Curve 2Ahmed Ridwan OladotunNoch keine Bewertungen
- MRP Configuration GuideDokument12 SeitenMRP Configuration Guideofaofa1Noch keine Bewertungen
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTVon EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 1: Brain and Neck: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTNoch keine Bewertungen
- Iaea TRS 430Dokument302 SeitenIaea TRS 430Alvaro Hermosilla ManríquezNoch keine Bewertungen
- Guide To Right Dose 03508199Dokument172 SeitenGuide To Right Dose 03508199Antonio GligorievskiNoch keine Bewertungen
- Chapter 13 BrachytherapyDokument82 SeitenChapter 13 Brachytherapyzulvan aviviNoch keine Bewertungen
- Principles of SpectDokument31 SeitenPrinciples of Spectinvaap100% (1)
- IMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DDokument3 SeitenIMRT Basics: R. Alfredo C. Siochi, Ph.D. Juan Carlos Celi, PH.DSantanu SamantaNoch keine Bewertungen
- IMRT Part 2 BJRDokument6 SeitenIMRT Part 2 BJRsusdoctorNoch keine Bewertungen
- Radiology Notes (1-36)Dokument83 SeitenRadiology Notes (1-36)el spin artifactNoch keine Bewertungen
- Dynamic Postioning SystemDokument50 SeitenDynamic Postioning Systempraveen_meo1Noch keine Bewertungen
- Understanding BrachytherapyDokument28 SeitenUnderstanding Brachytherapyqwertu132Noch keine Bewertungen
- New Techniques in Radiation TherapyDokument102 SeitenNew Techniques in Radiation Therapyapi-3726116100% (3)
- Multi-Slice CT: Principles and PerspectivesDokument64 SeitenMulti-Slice CT: Principles and PerspectivesMuksinUcinNoch keine Bewertungen
- Basic radiobiology: fractionation, 5 Rs, α/β ratio, QUANTEC: ESO Masterclass in Oncology Basics for BeginnersDokument32 SeitenBasic radiobiology: fractionation, 5 Rs, α/β ratio, QUANTEC: ESO Masterclass in Oncology Basics for BeginnersAji PatriajatiNoch keine Bewertungen
- Radiation Oncology A Physicists Eye ViewDokument332 SeitenRadiation Oncology A Physicists Eye Viewquyen2012100% (1)
- Brachytherapy in Cancer CervixDokument65 SeitenBrachytherapy in Cancer CervixSatyesh NadellaNoch keine Bewertungen
- 05-4d CT Lung PlanningDokument104 Seiten05-4d CT Lung PlanningchanmamaNoch keine Bewertungen
- 2005 Therapy Part II TypeDokument8 Seiten2005 Therapy Part II TypeDyhoiNoch keine Bewertungen
- IMRT by Musaib MushtaqDokument44 SeitenIMRT by Musaib MushtaqDr. Musaib MushtaqNoch keine Bewertungen
- ICRU 38 Interstitial ReportingDokument42 SeitenICRU 38 Interstitial ReportingLaura MDNoch keine Bewertungen
- New Advanced in RadiotherapyDokument49 SeitenNew Advanced in RadiotherapyIndonesian Journal of CancerNoch keine Bewertungen
- Hospital Class FFFDokument27 SeitenHospital Class FFFFrancisco HernandezNoch keine Bewertungen
- ICRU Reporte 38Dokument30 SeitenICRU Reporte 38Marco Herrera100% (1)
- Normal CT ChestDokument81 SeitenNormal CT ChestRahmat SyahiliNoch keine Bewertungen
- RayStation Brochure Ver3WEBDokument12 SeitenRayStation Brochure Ver3WEBSonik AlexNoch keine Bewertungen
- TG-43 ArDokument68 SeitenTG-43 ArCecilia Querebalu Garcia0% (1)
- 5&6.LinearAccelrators 1314thmay2013 ImranPatelDokument99 Seiten5&6.LinearAccelrators 1314thmay2013 ImranPatelAmr MuhammedNoch keine Bewertungen
- Photon SpectraDokument8 SeitenPhoton SpectraSrinivas VenkataramanNoch keine Bewertungen
- Lecture 5 Brachytherapy Implantation - 6-18 FinalDokument10 SeitenLecture 5 Brachytherapy Implantation - 6-18 FinalArcrije JerezNoch keine Bewertungen
- Icru 58Dokument45 SeitenIcru 58Zoran MirkovNoch keine Bewertungen
- 3D Dose Computation AlgorithmsDokument10 Seiten3D Dose Computation AlgorithmsHashir SaeedNoch keine Bewertungen
- LINAC PrincipleDokument13 SeitenLINAC PrincipleMehrdadNoch keine Bewertungen
- Image Guided Radiotherapy Technique - IGRTDokument13 SeitenImage Guided Radiotherapy Technique - IGRTbadusha vpNoch keine Bewertungen
- Plan EvaluationDokument56 SeitenPlan EvaluationSidhartha DevNoch keine Bewertungen
- Part 2 Week 9 - Treatment PlanningDokument50 SeitenPart 2 Week 9 - Treatment PlanningdanNoch keine Bewertungen
- CT SimulatorDokument7 SeitenCT SimulatorRaras HanifatunnisaNoch keine Bewertungen
- Radiotherapy SARP PDFDokument5 SeitenRadiotherapy SARP PDFskNoch keine Bewertungen
- SBRT PDFDokument14 SeitenSBRT PDFrubenNoch keine Bewertungen
- MR Pulse SequencesDokument125 SeitenMR Pulse SequencesdrphducNoch keine Bewertungen
- Medical Physics ResourcesDokument10 SeitenMedical Physics ResourceschanderNoch keine Bewertungen
- P8-9 CoverStory CT-HistoryDokument2 SeitenP8-9 CoverStory CT-Historyalem87Noch keine Bewertungen
- Nuclear MedicineDokument2 SeitenNuclear MedicineRadlinkSingaporeNoch keine Bewertungen
- Independent Dose Calculations Concepts and ModelsDokument104 SeitenIndependent Dose Calculations Concepts and ModelsMuhammad Nauman UsmaniNoch keine Bewertungen
- Rtog 0813 Marina CousinsDokument22 SeitenRtog 0813 Marina Cousinsapi-426094285Noch keine Bewertungen
- Experience in Commissioning The Halcyon Linac: Medical Physics July 2019Dokument19 SeitenExperience in Commissioning The Halcyon Linac: Medical Physics July 2019Michelle LEINoch keine Bewertungen
- Gamma CameraDokument68 SeitenGamma CameraSafwan ShaikhNoch keine Bewertungen
- IMRT Part 1 BJRDokument9 SeitenIMRT Part 1 BJRsusdoctorNoch keine Bewertungen
- Sources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3Von EverandSources, Fields, Measurements, and Applications: Radiation Dosimetry, Vol. 3Frank H. AttixNoch keine Bewertungen
- PetDokument8 SeitenPetTsetsaNoch keine Bewertungen
- Estro - Practical Guide in Brachytherapy Qa PDFDokument270 SeitenEstro - Practical Guide in Brachytherapy Qa PDFanamariatornero50% (2)
- Icru 38Dokument14 SeitenIcru 38Ronald Koeman Casique Useche100% (2)
- Csi Plan Writeup Portion Turn in PDFDokument13 SeitenCsi Plan Writeup Portion Turn in PDFapi-481226212Noch keine Bewertungen
- Week 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84Dokument84 SeitenWeek 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84chicken66Noch keine Bewertungen
- Materi Pak ARIEF LAGA PUTRADokument32 SeitenMateri Pak ARIEF LAGA PUTRAUnggul Febrian PangestuNoch keine Bewertungen
- Semi-Conductor Laboratory - MohaliDokument4 SeitenSemi-Conductor Laboratory - MohalimanjnderNoch keine Bewertungen
- Computer Graphics Question For Final ExamDokument3 SeitenComputer Graphics Question For Final ExamMd Rifat BhuiyanNoch keine Bewertungen
- Kina23744ens 002-Seisracks1Dokument147 SeitenKina23744ens 002-Seisracks1Adrian_Condrea_4281Noch keine Bewertungen
- Protein Dot BlottingDokument4 SeitenProtein Dot BlottingstcosmoNoch keine Bewertungen
- Gender InequalityDokument9 SeitenGender InequalityRhzNoch keine Bewertungen
- Bab 4 Ba501 Pecahan SeparaDokument24 SeitenBab 4 Ba501 Pecahan SeparaPrince ShanNoch keine Bewertungen
- 8 - Energy Balance of Solar CollectorsDokument27 Seiten8 - Energy Balance of Solar Collectorsftsebeek6164Noch keine Bewertungen
- KRAWIEC, Representations of Monastic Clothing in Late AntiquityDokument27 SeitenKRAWIEC, Representations of Monastic Clothing in Late AntiquityDejan MitreaNoch keine Bewertungen
- Lesson 2 (Locating Main Ideas)Dokument18 SeitenLesson 2 (Locating Main Ideas)Glyneth Dela TorreNoch keine Bewertungen
- Non-Display Industrial Computers: User ManualDokument100 SeitenNon-Display Industrial Computers: User ManualJason100% (1)
- Practice Problems in ADSORPTION and ION EXCHANGE - SolutionsDokument8 SeitenPractice Problems in ADSORPTION and ION EXCHANGE - SolutionsJenna Brasz100% (2)
- Strong PasswordDokument2 SeitenStrong PasswordluciangeNoch keine Bewertungen
- New Text Document 22Dokument90 SeitenNew Text Document 22Marija SerifovskaNoch keine Bewertungen
- I. Objectives: A. Power Point PresentationDokument3 SeitenI. Objectives: A. Power Point PresentationJohn Brad Angelo LacuataNoch keine Bewertungen
- Oracle Database Administrator TasksDokument2 SeitenOracle Database Administrator TasksPratik GandhiNoch keine Bewertungen
- UCOL Online Style GuideDokument8 SeitenUCOL Online Style GuideucoledtechNoch keine Bewertungen
- Vertical Axis Wind Turbine ProjDokument2 SeitenVertical Axis Wind Turbine Projmacsan sanchezNoch keine Bewertungen
- Assignment Diffraction 2016Dokument3 SeitenAssignment Diffraction 2016Ritesh MeelNoch keine Bewertungen
- Contoh RefleksiDokument7 SeitenContoh RefleksiIzzat HanifNoch keine Bewertungen
- Marine BiomesDokument27 SeitenMarine BiomesJe Ssica100% (1)
- Kolkata City Accident Report - 2018Dokument48 SeitenKolkata City Accident Report - 2018anon_109699702Noch keine Bewertungen
- Agents SocializationDokument4 SeitenAgents Socializationinstinct920% (1)
- Global 1 Syllabus Fall 2014Dokument5 SeitenGlobal 1 Syllabus Fall 2014Henry WangNoch keine Bewertungen
- Philosophy 101Dokument8 SeitenPhilosophy 101scribd5846Noch keine Bewertungen
- GAT General - Sample PaperDokument10 SeitenGAT General - Sample PaperAltaf AhmadNoch keine Bewertungen