Das könnte Ihnen auch gefallen
- Varicose VainsDokument28 SeitenVaricose Vainssingireddi1revathi100% (1)
- Tibial and Femur FactrueDokument25 SeitenTibial and Femur Factruesingireddi1revathiNoch keine Bewertungen
- Community Health NursingDokument14 SeitenCommunity Health Nursingsingireddi1revathi100% (2)
- Ordinance & R.nursingDokument9 SeitenOrdinance & R.nursingsingireddi1revathiNoch keine Bewertungen
- Medical Surgical NursingDokument31 SeitenMedical Surgical Nursingsingireddi1revathi100% (3)
- Pathology SyllabusDokument15 SeitenPathology Syllabussingireddi1revathi100% (2)
- SociologyDokument5 SeitenSociologyRAJUNoch keine Bewertungen
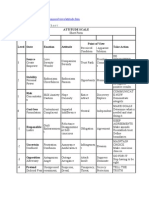
- Attitude ScaleDokument51 SeitenAttitude Scalesingireddi1revathi100% (3)
- Pathology and GeneticsDokument11 SeitenPathology and Geneticssingireddi1revathi33% (3)
- Acute Kidney Failure OverviewDokument13 SeitenAcute Kidney Failure Overviewsingireddi1revathiNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Influence of Irish Monks On Merovingian Diocesan Organization-Robbins BittermannDokument15 SeitenThe Influence of Irish Monks On Merovingian Diocesan Organization-Robbins BittermanngeorgiescuNoch keine Bewertungen
- Micro EvolutionDokument9 SeitenMicro EvolutionBryan TanNoch keine Bewertungen
- The Covenant Taken From The Sons of Adam Is The FitrahDokument10 SeitenThe Covenant Taken From The Sons of Adam Is The FitrahTyler FranklinNoch keine Bewertungen
- Lecture 14 Direct Digital ManufacturingDokument27 SeitenLecture 14 Direct Digital Manufacturingshanur begulaji0% (1)
- Business Plan in BDDokument48 SeitenBusiness Plan in BDNasir Hossen100% (1)
- TriPac EVOLUTION Operators Manual 55711 19 OP Rev. 0-06-13Dokument68 SeitenTriPac EVOLUTION Operators Manual 55711 19 OP Rev. 0-06-13Ariel Noya100% (1)
- The cardioprotective effect of astaxanthin against isoprenaline-induced myocardial injury in rats: involvement of TLR4/NF-κB signaling pathwayDokument7 SeitenThe cardioprotective effect of astaxanthin against isoprenaline-induced myocardial injury in rats: involvement of TLR4/NF-κB signaling pathwayMennatallah AliNoch keine Bewertungen
- Canon Powershot S50 Repair Manual (CHAPTER 4. PARTS CATALOG) PDFDokument13 SeitenCanon Powershot S50 Repair Manual (CHAPTER 4. PARTS CATALOG) PDFRita CaselliNoch keine Bewertungen
- 2022 Mable Parker Mclean Scholarship ApplicationDokument2 Seiten2022 Mable Parker Mclean Scholarship Applicationapi-444959661Noch keine Bewertungen
- ChatGpt PDFDokument19 SeitenChatGpt PDFsanx2014100% (1)
- Perancangan Crushing Plant Batu Andesit Di PT Nurmuda Cahaya Desa Batujajar Timur Kecamatan Batujajar Kabupaten Bandung Barat Provinsi Jawa BaratDokument8 SeitenPerancangan Crushing Plant Batu Andesit Di PT Nurmuda Cahaya Desa Batujajar Timur Kecamatan Batujajar Kabupaten Bandung Barat Provinsi Jawa BaratSutan AdityaNoch keine Bewertungen
- ECE Companies ListDokument9 SeitenECE Companies ListPolaiah Geriki100% (1)
- Delonghi Esam Series Service Info ItalyDokument10 SeitenDelonghi Esam Series Service Info ItalyBrko BrkoskiNoch keine Bewertungen
- MCI Approved Medical College in Uzbekistan PDFDokument3 SeitenMCI Approved Medical College in Uzbekistan PDFMBBS ABROADNoch keine Bewertungen
- FuzzingBluetooth Paul ShenDokument8 SeitenFuzzingBluetooth Paul Shen许昆Noch keine Bewertungen
- Tool Charts PDFDokument3 SeitenTool Charts PDFtebengz100% (2)
- Notes:: Reinforcement in Manhole Chamber With Depth To Obvert Greater Than 3.5M and Less Than 6.0MDokument1 SeiteNotes:: Reinforcement in Manhole Chamber With Depth To Obvert Greater Than 3.5M and Less Than 6.0Mسجى وليدNoch keine Bewertungen
- Mechanical Production Engineer Samphhhhhle ResumeDokument2 SeitenMechanical Production Engineer Samphhhhhle ResumeAnirban MazumdarNoch keine Bewertungen
- Building Services Planning Manual-2007Dokument122 SeitenBuilding Services Planning Manual-2007razanmrm90% (10)
- Meno's Paradox of Inquiry and Socrates' Theory of RecollectionDokument10 SeitenMeno's Paradox of Inquiry and Socrates' Theory of RecollectionPhilip DarbyNoch keine Bewertungen
- Man As God Created Him, ThemDokument3 SeitenMan As God Created Him, ThemBOEN YATORNoch keine Bewertungen
- UT Dallas Syllabus For Govt4396.002.08s Taught by Gregory Thielemann (Gregt)Dokument2 SeitenUT Dallas Syllabus For Govt4396.002.08s Taught by Gregory Thielemann (Gregt)UT Dallas Provost's Technology GroupNoch keine Bewertungen
- C2 - Conveyors Diagram: Peso de Faja Longitud de CargaDokument1 SeiteC2 - Conveyors Diagram: Peso de Faja Longitud de CargaIvan CruzNoch keine Bewertungen
- What's New in CAESAR II: Piping and Equipment CodesDokument1 SeiteWhat's New in CAESAR II: Piping and Equipment CodeslnacerNoch keine Bewertungen
- Dwnload Full Principles of Economics 7th Edition Frank Solutions Manual PDFDokument35 SeitenDwnload Full Principles of Economics 7th Edition Frank Solutions Manual PDFmirthafoucault100% (8)
- AMULDokument11 SeitenAMULkeshav956Noch keine Bewertungen
- My Mother at 66Dokument6 SeitenMy Mother at 66AnjanaNoch keine Bewertungen
- Chapter 23Dokument9 SeitenChapter 23Javier Chuchullo TitoNoch keine Bewertungen
- Physics Blue Print 1 Class XI Half Yearly 23Dokument1 SeitePhysics Blue Print 1 Class XI Half Yearly 23Nilima Aparajita SahuNoch keine Bewertungen
- HatfieldDokument33 SeitenHatfieldAlex ForrestNoch keine Bewertungen