Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Activity 2 - Biochemical Processes (Revised 6.8.20)Dokument6 SeitenActivity 2 - Biochemical Processes (Revised 6.8.20)Sherma Sheikh karimNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Oxygen Concentrator Generator: Mayank Kumar Singh (2018016104) Aman Prakash (2019007968) Hamid Siddiqui (2019006342)Dokument6 SeitenOxygen Concentrator Generator: Mayank Kumar Singh (2018016104) Aman Prakash (2019007968) Hamid Siddiqui (2019006342)Rahul SaiNoch keine Bewertungen
- DABCO - Evonik Catalyst CatalogueDokument9 SeitenDABCO - Evonik Catalyst CataloguePhuong The Nguyen100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Functional Anatomy of Prokaryotic and Eukaryotic CellsDokument70 SeitenFunctional Anatomy of Prokaryotic and Eukaryotic CellsTrixie De GuzmanNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- SPT Mozley Desanding Hydrocyclones BrochureDokument2 SeitenSPT Mozley Desanding Hydrocyclones BrochureperrychemNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Formulation and Development of Taste Masked Ambroxol Hydrochloride Suspension Using Ion Exchange ResinsDokument4 SeitenFormulation and Development of Taste Masked Ambroxol Hydrochloride Suspension Using Ion Exchange ResinsAgung AtmajaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Vipel Chemical Resistance Guide: Corrosion Resistant Resins For The Harshest EnvironmentsDokument32 SeitenVipel Chemical Resistance Guide: Corrosion Resistant Resins For The Harshest EnvironmentsCésar AreinamoNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Test Bank For Clinical Laboratory Chemistry SunheimerDokument13 SeitenTest Bank For Clinical Laboratory Chemistry SunheimerWilbur Penny100% (36)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Impression Compounds and AlginatesDokument13 SeitenImpression Compounds and Alginatessourav dasNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Oxygen Family - Theory Notes With Illustrative Examples (Unlocked by WWW - Freemypdf.com)Dokument15 SeitenOxygen Family - Theory Notes With Illustrative Examples (Unlocked by WWW - Freemypdf.com)Imran Khan100% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Wilson - PhysioEx Exercise 1 Activity 5Dokument3 SeitenWilson - PhysioEx Exercise 1 Activity 5Hulwah ShalihahNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Acknowledgement: M.R. Head of Civil Engineering Department, For Inspiring Take This Project. I Also ExpressedDokument18 SeitenAcknowledgement: M.R. Head of Civil Engineering Department, For Inspiring Take This Project. I Also ExpressedRicky RickxNoch keine Bewertungen
- F2882-12 Standard Specification For Screws, Alloy Steel, Heat Treated, 170 Ksi Minimum Tensile StrengthDokument5 SeitenF2882-12 Standard Specification For Screws, Alloy Steel, Heat Treated, 170 Ksi Minimum Tensile StrengthhugoNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Tutorial QuestionsDokument8 SeitenTutorial QuestionsMaame Efua Neizer100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Workshop Transformer Residual Life EnhancementDokument4 SeitenWorkshop Transformer Residual Life EnhancementdevcharuNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- ElectrolysisDokument48 SeitenElectrolysisGina100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Laboratory Manual: 1 Lmbty360Dokument50 SeitenLaboratory Manual: 1 Lmbty360Rise from the ashes100% (1)
- Extraction and Analysis of Eugenol From Cloves: Jdefrancesco@luc - EduDokument9 SeitenExtraction and Analysis of Eugenol From Cloves: Jdefrancesco@luc - Edu01Syafira Khairunissa M100% (1)
- The Metabolic Map Carbohydrates Part One Illustration AtfDokument1 SeiteThe Metabolic Map Carbohydrates Part One Illustration AtfJoax Wayne SanchezNoch keine Bewertungen
- Safety Data Sheet - EN - (89985628) DIHYDRO-3 - (TETRAPROPENYL) FURAN-2,5-DIONE (26544-38-7)Dokument7 SeitenSafety Data Sheet - EN - (89985628) DIHYDRO-3 - (TETRAPROPENYL) FURAN-2,5-DIONE (26544-38-7)castasoftNoch keine Bewertungen
- 3rd - Year - PPT - Chapter 4 PDFDokument70 Seiten3rd - Year - PPT - Chapter 4 PDFtolerakukuleNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Chemistry Jan 2023 Paper 2 Regional Marking SchemeDokument14 SeitenChemistry Jan 2023 Paper 2 Regional Marking SchemeKenzyNoch keine Bewertungen
- Gong Et Al. - 2019 - The Impact-Tensile Behavior of Cementitious Composites Reinforced With Carbon Textile and Short Polymer Fibers (2) - AnnotatedDokument20 SeitenGong Et Al. - 2019 - The Impact-Tensile Behavior of Cementitious Composites Reinforced With Carbon Textile and Short Polymer Fibers (2) - AnnotatedMirza BasitNoch keine Bewertungen
- Eliminating Mercury From Chlorine Production Sep11 Web0Dokument10 SeitenEliminating Mercury From Chlorine Production Sep11 Web0pinitNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Testing Printing Ink Vehicles and Components Thereof: Standard Guide ForDokument4 SeitenTesting Printing Ink Vehicles and Components Thereof: Standard Guide Forgravity castNoch keine Bewertungen
- Chemistry - Chemical Equations WorksheetDokument2 SeitenChemistry - Chemical Equations WorksheetVasipalli Eshan AdityaNoch keine Bewertungen
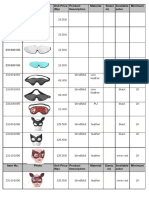
- Item No. Photo Unit Price (RP) Product Description Material Size (C M) Available Color MinimumDokument20 SeitenItem No. Photo Unit Price (RP) Product Description Material Size (C M) Available Color Minimumrobiyanto wandooNoch keine Bewertungen
- 13.09 Stream A AxensDokument27 Seiten13.09 Stream A AxensJorge Ariel QuipildorNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Lecture 16Dokument15 SeitenLecture 16Fabiha Shafi MimNoch keine Bewertungen
- Cat Hose and Fitting GuideDokument390 SeitenCat Hose and Fitting Guidegre29492% (24)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)