Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Cleft Lip and Palate Surgery: The Day of SurgeryDokument4 SeitenCleft Lip and Palate Surgery: The Day of SurgeryBean GemboelzNoch keine Bewertungen
- Shock RosenDokument10 SeitenShock RosenJuan GallegoNoch keine Bewertungen
- Presentation 1Dokument21 SeitenPresentation 1Shekinah Ruth ManupacNoch keine Bewertungen
- Cerebral PalsyDokument27 SeitenCerebral PalsyAman SamNoch keine Bewertungen
- ConjunctivitisDokument25 SeitenConjunctivitisValentina bustamanteNoch keine Bewertungen
- LESSON PLAN BronchitisDokument3 SeitenLESSON PLAN BronchitisDiana Laura Lei100% (1)
- Chronic UrticariaDokument4 SeitenChronic UrticariaayukNoch keine Bewertungen
- Mood StabilizersDokument6 SeitenMood StabilizersLan FdzNoch keine Bewertungen
- Septic Shock Clinical Practice GuidelinesDokument21 SeitenSeptic Shock Clinical Practice GuidelinesprinsepejesseNoch keine Bewertungen
- Definition of Kidney StonesDokument4 SeitenDefinition of Kidney StonesArul MNoch keine Bewertungen
- This Is Known As Student DiversityDokument3 SeitenThis Is Known As Student DiversityAngela Marie Hilario PacursaNoch keine Bewertungen
- Barret's & Tumors of Esophagus, SR, April 20Dokument52 SeitenBarret's & Tumors of Esophagus, SR, April 20Tehreem NadeemNoch keine Bewertungen
- Cornea and External DiseaseDokument26 SeitenCornea and External Diseaserajeshwari saravananNoch keine Bewertungen
- Nursing Care of A Family Experiencing A Postpartal Complications PDFDokument9 SeitenNursing Care of A Family Experiencing A Postpartal Complications PDFTandingco, Olivia Mari H.Noch keine Bewertungen
- Nephrotic and Nephritic Syndrome: Med5010 LectureDokument65 SeitenNephrotic and Nephritic Syndrome: Med5010 LectureFreeburn Simunchembu100% (1)
- Surgery Pretest SummaryDokument9 SeitenSurgery Pretest SummaryPrince DuNoch keine Bewertungen
- NANDA Nursing DiagnosisDokument6 SeitenNANDA Nursing DiagnosisAlex HanNoch keine Bewertungen
- Van Duyn May 11, 2021 InspectionDokument12 SeitenVan Duyn May 11, 2021 InspectionJames MulderNoch keine Bewertungen
- Perioperative Care of A Pediatric Surgical PatientDokument60 SeitenPerioperative Care of A Pediatric Surgical Patienthabtsh habshaNoch keine Bewertungen
- Human Behavior Victimology 75 102 PDFDokument28 SeitenHuman Behavior Victimology 75 102 PDFAndales Melbert G.Noch keine Bewertungen
- Articol Medicina de TrimisDokument19 SeitenArticol Medicina de TrimisMoldovan TiberiuNoch keine Bewertungen
- Ocular Trauma Dr. As-Ali 2 OktoberDokument61 SeitenOcular Trauma Dr. As-Ali 2 OktoberYama Piniel FrimantamaNoch keine Bewertungen
- Icd-10 & Icd-9Dokument56 SeitenIcd-10 & Icd-9CASEMIX JUANDANoch keine Bewertungen
- Dapus ReferatDokument2 SeitenDapus Referataulia dnNoch keine Bewertungen
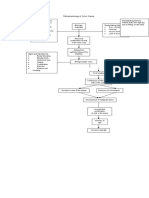
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDokument1 SeitePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiNoch keine Bewertungen
- Basic Cut Razor Sharp AbsDokument12 SeitenBasic Cut Razor Sharp AbsHelboy BautistaNoch keine Bewertungen
- Drug Study - AminophyllineDokument3 SeitenDrug Study - AminophyllineTrisha Lapid MatulaNoch keine Bewertungen
- 2009 Nec Hiv Dec Aidsreg2009Dokument3 Seiten2009 Nec Hiv Dec Aidsreg2009Jing CruzNoch keine Bewertungen
- Birt-Hogg-Dube Syndrome PDFDokument11 SeitenBirt-Hogg-Dube Syndrome PDFhNoch keine Bewertungen
- Numerology 1 - IntroductionDokument15 SeitenNumerology 1 - IntroductionReiki Kiran100% (3)