Asthma
Author: Michael J Morris, MD; Chief Editor: Zab Mosenifar, MD more... Updated: Jul 27, 2011
Background
Asthma is a common chronic disease worldwide and affects approximately 24 million persons in the United States. It is the most common chronic disease in childhood, affecting an estimated 7 million children, and it is a common cause of hospitalization for children in the United States. The pathophysiology of asthma is complex and involves airway inflammation, intermittent airflow obstruction, and bronchial hyperresponsiveness. The mechanism of inflammation in asthma may be acute, subacute, or chronic, and the presence of airway edema and mucus secretion also contributes to airflow obstruction and bronchial reactivity. Varying degrees of mononuclear cell and eosinophil infiltration, mucus hypersecretion, desquamation of the epithelium, smooth muscle hyperplasia, and airway remodeling are present.[1, 2] Airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to numerous exogenous and endogenous stimuli. The mechanisms involved include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness generally correlates with the clinical severity of asthma. Spirometry with postbronchodilator response should be obtained as the primary test to establish the asthma diagnosis. Pulse oximetry measurement is desirable in all patients with acute asthma to exclude hypoxemia. The chest radiograph remains the initial imaging evaluation in most individuals with symptoms of asthma, but in most patients with asthma, chest radiography findings are normal or may indicate hyperinflation. Exercise spirometry is the standard method for assessing patients with exercise-induced bronchospasm. Physical findings vary with the severity of the asthma and with the absence or presence of an acute episode and its severity. The severity of asthma is classified as intermittent, mild persistent, moderate persistent, or severe persistent. Patients with asthma of any level of severity may have mild, moderate, or severe exacerbations. Pharmacologic management includes the use of relief and control agents. Control agents include inhaled corticosteroids, inhaled cromolyn (Intal) or nedocromil (Tilade), long-acting bronchodilators, theophylline (Theo-24, Theochron, Uniphyl), leukotriene modifiers, and anti-IgE antibodies. Relief medications include short-acting bronchodilators, systemic corticosteroids, and ipratropium (Atrovent). With severe exacerbations, indications for hospitalization are based on findings after the patient receives 3 doses of an inhaled bronchodilator. In general, patients should be assessed every 1-6 months for asthma control.
Anatomy
The airways of the lungs consist of the cartilaginous bronchi, membranous bronchi, and gas-exchanging bronchi termed the respiratory bronchioles and alveolar ducts. While the first 2 types function mostly as anatomic dead space, they also contribute to airway resistance. The smallest non-gas-exchanging airways, the terminal bronchioles, are approximately 0.5 mm in diameter; airways are considered small if they are less than 2 mm in diameter.[3] Airway structure consists of the following: Mucosa, which is composed of epithelial cells that are capable of specialized mucous production and a transport apparatus Basement membrane A smooth-muscle matrix extending to the alveolar entrances Predominantly fibrocartilaginous or fibroelastic-supporting connective tissue.
Cellular elements include mast cells, which are involved in the complex control of releasing histamine and other mediators. Basophils, eosinophils, neutrophils, and macrophages also are responsible for extensive mediator release in the early and late stages of bronchial asthma. Stretch and irritant receptors reside in the airways, as do cholinergic motor nerves, which innervate the smooth muscle and glandular units. In bronchial asthma, smooth muscle contraction in an airway is greater than that expected for its size if it were functioning normally, and this contraction varies in its distribution.
Pathophysiology
The 2007 Expert Panel Report 3 (EPR-3) of the National Asthma Education and Prevention Program (NAEPP) noted several key changes in the understanding of the pathophysiology of asthma[4] : The critical role of inflammation has been further substantiated, but evidence is emerging for considerable variability in the pattern of inflammation, thus indicating phenotypic differences that may influence treatment responses Of the environmental factors, allergic reactions remain important. Evidence also suggests a key and expanding role for viral respiratory infections in these processes The onset of asthma for most patients begins early in life, with the pattern of disease persistence determined by early, recognizable risk factors including atopic disease, recurrent wheezing, and a parental history of asthma Current asthma treatment with anti-inflammatory therapy does not appear to prevent progression of the underlying disease severity The pathophysiology of asthma is complex and involves the following components: Airway inflammation Intermittent airflow obstruction Bronchial hyperresponsiveness
Airway inflammation
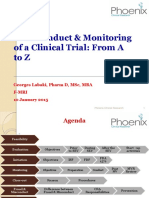
The mechanism of inflammation in asthma may be acute, subacute, or chronic, and the presence of airway edema and mucus secretion also contributes to airflow obstruction and bronchial reactivity. Varying degrees of mononuclear cell and eosinophil infiltration, mucus hypersecretion, desquamation of the epithelium, smooth muscle hyperplasia, and airway remodeling are present.[1] See the image below.
Asthma treatment. Asthma causes and symptoms. Antigen presentation by the dendritic cell w ith the lymphocyte and cytokine response leading to airw ay inflammation and asthma symptoms.
Some of the principal cells identified in airway inflammation include mast cells, eosinophils, epithelial cells, macrophages, and activated T lymphocytes. T lymphocytes play an important role in the regulation of airway inflammation through the release of numerous cytokines. Other constituent airway cells, such as fibroblasts, endothelial cells, and epithelial cells, contribute to the chronicity of the disease. Other factors, such as adhesion molecules (eg, selectins, integrins), are critical in directing the inflammatory changes in the airway. Finally, cellderived mediators influence smooth muscle tone and produce structural changes and remodeling of the airway. The presence of airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to numerous exogenous and endogenous stimuli. The mechanisms involved include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness generally correlates with the clinical severity of asthma.
A study by Balzar et al reported changes in airway resident mast cell populations from a large group of subjects with asthma and normal control subjects.[5] A greater proportion of chymase-positive mast cells in the airways and increased prostaglandin D2 levels were identified as important predictors of severe asthma as compared with other steroid-treated subjects with asthma. Chronic inflammation of the airways is associated with increased bronchial hyperresponsiveness, which leads to bronchospasm and typical symptoms of wheezing, shortness of breath, and coughing after exposure to allergens, environmental irritants, viruses, cold air, or exercise. In some patients with chronic asthma, airflow limitation may be only partially reversible because of airway remodeling (hypertrophy and hyperplasia of smooth muscle, angiogenesis, and subepithelial fibrosis) that occurs with chronic untreated disease. Airway inflammation in asthma may represent a loss of normal balance between two "opposing" populations of Th lymphocytes. Two types of Th lymphocytes have been characterized: Th1 and Th2. Th1 cells produce interleukin (IL)-2 and IFN-, which are critical in cellular defense mechanisms in response to infection. Th2, in contrast, generates a family of cytokines (IL-4, IL-5, IL-6, IL-9, and IL-13) that can mediate allergic inflammation. A study by Gauvreau et al found that IL-13 has a role in allergen-induced airway responses.[6] The current "hygiene hypothesis" of asthma illustrates how this cytokine imbalance may explain some of the dramatic increases in asthma prevalence in westernized countries.[7] This hypothesis is based on the concept that the immune system of the newborn is skewed toward Th2 cytokine generation (mediators of allergic inflammation). Following birth, environmental stimuli such as infections activate Th1 responses and bring the Th1/Th2 relationship to an appropriate balance.
Airflow obstruction
Airflow obstruction can be caused by a variety of changes, including acute bronchoconstriction, airway edema, chronic mucous plug formation, and airway remodeling. Acute bronchoconstriction is the consequence of immunoglobulin E-dependent mediator release upon exposure to aeroallergens and is the primary component of the early asthmatic response. Airway edema occurs 6-24 hours following an allergen challenge and is referred to as the late asthmatic response. Chronic mucous plug formation consists of an exudate of serum proteins and cell debris that may take weeks to resolve. Airway remodeling is associated with structural changes due to longstanding inflammation and may profoundly affect the extent of reversibility of airway obstruction.[8] Airway obstruction causes increased resistance to airflow and decreased expiratory flow rates. These changes lead to a decreased ability to expel air and may result in hyperinflation. The resulting overdistention helps maintain airway patency, thereby improving expiratory flow; however, it also alters pulmonary mechanics and increases the work of breathing.
Bronchial hyperresponsiveness
Hyperinflation compensates for the airflow obstruction, but this compensation is limited when the tidal volume approaches the volume of the pulmonary dead space; the result is alveolar hypoventilation. Uneven changes in airflow resistance, the resulting uneven distribution of air, and alterations in circulation from increased intra-alveolar pressure due to hyperinflation all lead to ventilation-perfusion mismatch. Vasoconstriction due to alveolar hypoxia also contributes to this mismatch. Vasoconstriction is also considered an adaptive response to ventilation/perfusion mismatch. In the early stages, when ventilation-perfusion mismatch results in hypoxia, hypercarbia is prevented by the ready diffusion of carbon dioxide across alveolar capillary membranes. Thus, patients with asthma who are in the early stages of an acute episode have hypoxemia in the absence of carbon dioxide retention. Hyperventilation triggered by the hypoxic drive also causes a decrease in PaCO2. An increase in alveolar ventilation in the early stages of an acute exacerbation prevents hypercarbia. With worsening obstruction and increasing ventilation-perfusion mismatch, carbon dioxide retention occurs. In the early stages of an acute episode, respiratory alkalosis results from hyperventilation. Later, the increased work of breathing, increased oxygen consumption, and increased cardiac output result in metabolic acidosis. Respiratory failure leads to respiratory acidosis.
Etiology
Factors that can contribute to asthma or airway hyperreactivity may include any of the following: Environmental allergens (eg, house dust mites; animal allergens, especially cat and dog; cockroach allergens; and fungi)
allergens; and fungi) Viral respiratory tract infections Exercise, hyperventilation Gastroesophageal reflux disease Chronic sinusitis or rhinitis Aspirin or nonsteroidal anti-inflammatory drug (NSAID) hypersensitivity, sulfite sensitivity Use of beta-adrenergic receptor blockers (including ophthalmic preparations) Obesity [9] Environmental pollutants, tobacco smoke Occupational exposure Irritants (eg, household sprays, paint fumes) Various high- and low-molecular-weight compounds (eg, insects, plants, latex, gums, diisocyanates, anhydrides, wood dust, and fluxes; associated with occupational asthma) Emotional factors or stress Perinatal factors (prematurity and increased maternal age; maternal smoking and prenatal exposure to tobacco smoke; breastfeeding has not been definitely shown to be protective)
Aspirin-induced asthma
The triad of asthma, aspirin sensitivity, and nasal polyps affects 5-10% of patients with asthma. Most patients experience symptoms during the third to fourth decade. A single dose can provoke an acute asthma exacerbation, accompanied by rhinorrhea, conjunctival irritation, and flushing of the head and neck. It can also occur with other nonsteroidal anti-inflammatory drugs and is caused by an increase in eosinophils and cysteinyl leukotrienes after exposure.[10] A study by Beasley et al demonstrated some epidemiological evidence that exposure to acetaminophen is associated with an increased risk of asthma.[11] However, no clinical studies have directly linked asthma symptoms with acetaminophen use. Primary treatment is avoidance of these medications, but leukotriene antagonists have shown promise in treatment, allowing these patients to take daily aspirin for cardiac or rheumatic disease.
Gastroesophageal reflux disease
The presence of acid in the distal esophagus, mediated via vagal or other neural reflexes, can significantly increase airway resistance and airway reactivity. Patients with asthma are 3 times more likely to also have GERD.[12] Some people with asthma have significant gastroesophageal reflux without esophageal symptoms. Gastroesophageal reflux was found to be a definite asthma-causing factor (defined by a favorable asthma response to medical antireflux therapy) in 64% of patients; clinically silent reflux was present in 24% of all patients.[12]
Work-related asthma
Occupational factors are associated with 10-15% of adult asthma cases. More than 300 specific occupational agents have been associated with asthma. High-risk jobs include farming, painting, janitorial work, and plastics manufacturing. Given the prevalence of work-related asthma, the American College of Chest Physicians (ACCP) supports consideration of work-related asthma in all patients presenting with new-onset or worsening asthma. An ACCP consensus statement defines work-related asthmas as including occupational asthma (ie, asthma induced by sensitizer or irritant work exposures) and work-exacerbated asthma (ie, preexisting or concurrent asthma worsened by work factors).[13] Two types of occupational asthma are recognized: immune-related and non-immune-related. Immune-mediated asthma has a latency of months to years after exposure. Non-immune-mediated asthma, or irritant-induced asthma (reactive airway dysfunction syndrome), has no latency period and may occur within 24 hours after an accidental exposure to high concentrations of respiratory irritants. Pay careful attention to the patient's occupational history. Those with a history of asthma who report worsening of symptoms during the week and improvement during the weekends should be evaluated for occupational exposure. Peak-flow monitoring during work (optimally, at least 4 times a day) for at least 2 weeks and a similar period away from work is one recommended method to establish the diagnosis.[13] To see complete information on Allergic and Environmental Asthma, please go to the main article by clicking here.
Viral exposure in children
Evidence suggests that rhinovirus illness during infancy is a significant risk factor for the development of wheezing in preschool children and a frequent trigger of wheezing illnesses in children with asthma.[14] Human rhinovirus C (HRVC) is a newly identified genotype of HRV found in patients with respiratory tract infections. A study of children with acute asthma who presented to the emergency department found HRVC present in the majority of patients. The presence of HRVC was also associated with more severe asthma.[15] Approximately 80-85% of childhood asthma episodes are associated with prior viral exposure. Prior childhood pneumonia due to infection by respiratory syncytial virus, Mycoplasma pneumoniae, and/or Chlamydia species was found in more than 50% of a small sample of children aged 7-9 years who later had asthma.[16] Treatment with antibiotics appropriate for these organisms improves the clinical signs and symptoms of asthma.
Sinusitis
Of patients with asthma, 50% have concurrent sinus disease. Sinusitis is the most important exacerbating factor for asthma symptoms. Either acute infectious sinus disease or chronic inflammation may contribute to worsening airway symptoms. Treatment of nasal and sinus inflammation reduces airway reactivity. Treatment of acute sinusitis requires at least 10 days of antibiotics to improve asthma symptoms.[17]
Exercise-induced asthma
Exercise-induced asthma (EIA), or exercise-induced bronchospasm (EIB), is an asthma variant defined as a condition in which exercise or vigorous physical activity triggers acute bronchospasm in persons with heightened airway reactivity. It is observed primarily in persons who have asthma (exercise-induced bronchospasm in asthmatic persons) but can also be found in patients with normal resting spirometry findings with atopy, allergic rhinitis, or cystic fibrosis and even in healthy persons, many of whom are elite athletes (exercise-induced bronchospasm in athletes). Exercise-induced bronchospasm is often a neglected diagnosis, and the underlying asthma may be silent in as many as 50% of patients, except during exercise.[18, 19] The pathogenesis of exercise-induced bronchospasm is controversial. The disease may be mediated by water loss from the airway, heat loss from the airway, or a combination of both. The upper airway is designed to keep inspired air at 100% humidity and body temperature at 37C (98.6F). The nose is unable to condition the increased amount of air required for exercise, particularly in athletes who breathe through their mouths. The abnormal heat and water fluxes in the bronchial tree result in bronchoconstriction, occurring within minutes of completing exercise. Results from bronchoalveolar lavage studies have not demonstrated an increase in inflammatory mediators. These patients generally develop a refractory period, during which a second exercise challenge does not cause a significant degree of bronchoconstriction. Factors that contribute to exercise-induced bronchospasm symptoms (in both people with asthma and athletes) include the following: Exposure to cold or dry air Environmental pollutants (eg, sulfur, ozone) level of bronchial hyperreactivity Chronicity of asthma and symptomatic control Duration and intensity of exercise Allergen exposure in atopic individuals Coexisting respiratory infection The assessment and diagnosis of exercise-induced bronchospasm is made more often in children and young adults than in older adults and is related to high levels of physical activity. Exercise-induced bronchospasm can be observed in persons of any age based on the level of underlying airway reactivity and the level of physical exertion.
Genetics
Research on genetic mutations casts further light on the synergistic nature of multiple mutations in the pathophysiology of asthma. Polymorphisms in the gene that encodes platelet-activating factor hydrolase, an intrinsic neutralizing agent of platelet-activating factor in most humans, may play a role in susceptibility to asthma and asthma severity.[20] Evidence suggests that the prevalence of asthma is reduced in association with certain infections (Mycobacterium tuberculosis, measles, or hepatitis A); rural living; exposure to other children (eg, presence of older siblings and early enrollment in childcare); and less frequent use of antibiotics. Furthermore, the absence of these lifestyle
events is associated with the persistence of a Th2 cytokine pattern. Under these conditions, the genetic background of the child, with a cytokine imbalance toward Th2, sets the stage to promote the production of immunoglobulin E (IgE) antibody to key environmental antigens (eg, dust mites, cockroaches, Alternaria, and possibly cats). Therefore, a gene-by-environment interaction occurs in which the susceptible host is exposed to environmental factors that are capable of generating IgE, and sensitization occurs. A reciprocal interaction is apparent between the 2 subpopulations, in which Th1 cytokines can inhibit Th2 generation and vice versa. Allergic inflammation may be the result of an excessive expression of Th2 cytokines. Alternatively, recent studies suggest the possibility that the loss of normal immune balance arises from a cytokine dysregulation in which Th1 activity in asthma is diminished.[21] In addition, some studies highlight the importance of genotypes in children's susceptibility to asthma and response to specific antiasthma medications.[22, 23, 24, 25]
Obesity
A study by Cottrell et al explored the relationship between asthma, obesity, and abnormal lipid and glucose metabolism.[26] The study found that community-based data linked asthma, body mass, and metabolic variables in children. Specifically, these findings described a statistically significant association between asthma and abnormal lipid and glucose metabolism beyond body mass association.
Epidemiology
Asthma affects 5-10% of the population or an estimated 23.4 million persons, including 7 million children.[13] The overall prevalence rate of exercise-induced bronchospasm is 3-10% of the general population if persons who do not have asthma or allergy are excluded, but the rate increases to 12-15% of the general population if patients with underlying asthma are included. Asthma affects an estimated 300 million individuals worldwide. Annually, the World Health Organization (WHO) has estimated that 15 million disability-adjusted life-years are lost and 250,000 asthma deaths are reported worldwide.[27] In the United States, asthma prevalence, especially morbidity and mortality, is higher in blacks than in whites. Although genetic factors are of major importance in determining a predisposition to the development of asthma, environmental factors play a greater role than racial factors in asthma onset. A national concern is that some of the increased morbidity is due to differences in asthma treatment afforded certain minority groups. Larger asthmaassociated lung function deficits are reported in Hispanics, especially females.[28] Asthma is common in industrialized nations such as Canada, England, Australia, Germany, and New Zealand, where much of the asthma data have been collected. The prevalence rate of severe asthma in industrialized countries ranges from 2-10%. Trends suggest an increase in both the prevalence and morbidity of asthma, especially in children younger than 6 years. Factors that have been implicated include urbanization, air pollution, passive smoking, and change in exposure to environmental allergens. Asthma predominantly occurs in boys in childhood, with a male-to-female ratio of 2:1 until puberty, when the maleto-female ratio becomes 1:1. Asthma prevalence is greater in females after puberty, and the majority of adult-onset cases diagnosed in persons older than 40 years occur in females. Boys are more likely than girls to experience a decrease in symptoms by late adolescence. Asthma prevalence is increased in very young persons and very old persons because of airway responsiveness and lower levels of lung function.[29] Two thirds of all asthma cases are diagnosed before the patient is aged 18 years. Approximately half of all children diagnosed with asthma have a decrease or disappearance of symptoms by early adulthood.[30]
Prognosis
International asthma mortality is reported as high as 0.86 deaths per 100,000 persons in some countries. US asthma mortality rates in 2006 were reported at 1.2 deaths per 100,000 persons. Mortality is primarily related to lung function, with an 8-fold increase in patients in the lowest quartile, but mortality has also been linked with asthma management failure, especially in young persons. Other factors that impact mortality include age older than 40 years, cigarette smoking more than 20-pack years, blood eosinophilia, forced expiratory volume in one second (FEV1) of 40-69% predicted, and greater reversibility.[31]
The estimate of lost work and school time from asthma is approximately 100 million days of restricted activity. Approximately 500,000 annual hospitalizations (40.6% in individuals aged 18 y or younger) are due to asthma. Each year, an estimated 1.81 million people (47.8% of them aged 18 y or younger) require treatment in an emergency department.[32] For 2010, the annual expenditures for health and lost productivity due to asthma are projected to be $20.7 billion.[33] Nearly one half of children diagnosed with asthma have a decrease in symptoms and require less treatment by late adolescence or early adulthood. In a study of 900 children with asthma, 6% required no treatment after 1 year, and 39% only required intermittent treatment. Patients with poorly controlled asthma develop long-term changes over time (ie, with airway remodeling). This can lead to chronic symptoms and a significant irreversible component to their disease. Many patients who develop asthma at an older age also tend to have chronic symptoms.
Patient Education
The need for patient education about asthma and the establishment of a partnership between patient and clinician in the management of the disease was emphasized by EPR-3.[34] The key points of education include the following: Patient education should be integrated into every aspect of asthma care All members of the healthcare team, including nurses, pharmacists, and respiratory therapists, should provide education. Clinicians should teach patients asthma self-management based on basic asthma facts, self-monitoring techniques, the role of medications, inhaler use, and environmental control measures.[35, 36, 37] Treatment goals should be developed for the patient and family. A written, individualized, daily self-management plan should be developed. Several well-validated asthma action plans are now available and are key in the management of asthma and should therefore be reviewed: ACT (Asthma Control Test), ATAQ (Asthma Therapy Assessment Questionnaire), and ACQ (Asthma Control Questionnaire).[38] School-based asthma education programs improved knowledge of asthma, self-efficacy, and self-management behaviors in children aged 4-17 years, according to a systematic literature review by Coffman et al, but the programs had less effect on quality of life, days of symptoms, nights with symptoms, and school absences.[39] The 2009 Veterans Administration/Department of Defense (VA/DoD) clinical practice guideline for management of asthma in children and adults concurs with EPR-3 in recommending self-management education for both the patient and caregiver as part of the treatment program.[40] For excellent patient education resources, visit eMedicine's Asthma Center. Also, see eMedicine's patient education articles Asthma, Asthma FAQs, Asthma in Children, and Understanding Asthma Medications.
Contributor Information and Disclosures
Author Michael J Morris, MD Clinical Assistant Professor, Pulmonary Disease/Critical Care Service, Department of Medicine, Brooke Army Medical Center; Associate Program Director, Internal Medicine Residency, San Antonio Uniformed Services Health Education Consortium Michael J Morris, MD is a member of the following medical societies: American Association for Respiratory Care, American College of Chest Physicians, American College of Physicians, American Thoracic Society, and Association of Military Surgeons of the US Disclosure: Nothing to disclose. Coauthor(s) Gregory J Argyros Col, MD Director, Education, Training, and Research, J7/Joint Task Force, National Capital Region Medical; Professor of Medicine, Uniformed Services University of the Health Sciences Gregory J Argyros Col, MD is a member of the following medical societies: Alpha Omega Alpha, American College of Chest Physicians, American College of Physicians-American Society of Internal Medicine, and
American Thoracic Society Disclosure: Nothing to disclose. Stephen G Batuello, MD Consulting Staff, Colorado ENT Specialists Stephen G Batuello, MD is a member of the following medical societies: American Academy of OtolaryngologyHead and Neck Surgery, American College of Physician Executives, American Medical Association, and Colorado Medical Society Disclosure: Nothing to disclose. Edward Bessman, MD Chairman, Department of Emergency Medicine, John Hopkins Bayview Medical Center; Assistant Professor, Department of Emergency Medicine, Johns Hopkins University School of Medicine Edward Bessman, MD is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Paul Blackburn, DO, FACOEP, FACEP Attending Physician, Department of Emergency Medicine, Maricopa Medical Center Paul Blackburn, DO, FACOEP, FACEP is a member of the following medical societies: American College of Emergency Physicians, American College of Osteopathic Emergency Physicians, American Medical Association, and Arizona Medical Association Disclosure: Nothing to disclose. Barry E Brenner, MD, PhD, FACEP Professor of Emergency Medicine, Professor of Internal Medicine, Program Director, Emergency Medicine, Case Medical Center, University Hospitals, Case Western Reserve University School of Medicine Barry E Brenner, MD, PhD, FACEP is a member of the following medical societies: Alpha Omega Alpha, American Academy of Emergency Medicine, American College of Chest Physicians, American College of Emergency Physicians, American College of Physicians, American Heart Association, American Thoracic Society, Arkansas Medical Society, New York Academy of Medicine, New York Academy of Sciences, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Praveen Buddiga, MD Physician, Allergy, Asthma and Immunology, Baz Allergy, Asthma and Sinus Center, Fresno, California Praveen Buddiga, MD, is a member of the following medical societies: American Academy of Allergy Asthma and Immunology and American College of Allergy, Asthma and Immunology Disclosure: Meda Honoraria Speaking and teaching; Teva Honoraria Speaking and teaching; AstraZeneca Honoraria Speaking and teaching Robert K Bush, MD Professor of Medicine (CHS, Emeritus), University of Wisconsin School of Medicine and Public Health; Chief of Allergy (retired), William S Middleton Veterans Affairs Hospital Robert K Bush, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology and American College of Physicians Disclosure: University of WI- Madison Emeritus- Reitred; Wm S. Middleton VA Hospital Retired Retired; Teva Pharmaceuticals IRA Holding None; Associate Editor Journal Allergy Clinical Immunology Honoraria None Michael R Bye, MD Professor of Clinical Pediatrics, Division of Pulmonary Medicine, Columbia University College of Physicians and Surgeons; Attending Physician, Pediatric Pulmonary Medicine, Morgan Stanley Children's Hospital of New York Presbyterian, Columbia University Medical Center
Michael R Bye, MD is a member of the following medical societies: American Academy of Pediatrics, American College of Chest Physicians, and American Thoracic Society Disclosure: Nothing to disclose. Charles Callahan, DO Professor, Deputy Chief of Clinical Services, Walter Reed Army Medical Center Charles Callahan, DO is a member of the following medical societies: American Academy of Pediatrics, American College of Chest Physicians, American College of Osteopathic Pediatricians, American Thoracic Society, Association of Military Surgeons of the US, and Christian Medical & Dental Society Disclosure: Nothing to disclose. Peter G Canaday, MD Private Practice, Consultant Radiologist, Dakota Dunes, SD Peter G Canaday, MD is a member of the following medical societies: American College of Chest Physicians, American College of Radiology, American Medical Association, American Roentgen Ray Society, Nebraska Medical Association, Radiological Society of North America, Society of Breast Imaging, and Society of Thoracic Radiology Disclosure: Nothing to disclose. G Patricia Cantwell, MD, FCCM Professor of Clinical Pediatrics, University of Miami, Leonard M Miller School of Medicine; Chief, Division of Pediatric Critical Care Medicine, Medical Manager, Urban Search & Rescue, South Florida TF-2, Medical Director, Holtz Children's Hospital Palliative Care Team, Medical Director, Tilli Kids Pediatric Initiative of Hospice Care of SE Florida, Director, Pediatric Critical Care Transport, Holtz Children's Hospital/Jackson Memorial Hospital G Patricia Cantwell, MD, FCCM is a member of the following medical societies: American Academy of Hospice and Palliative Medicine, American Academy of Pediatrics, American Heart Association, American Trauma Society, National Association of EMS Physicians, Society of Critical Care Medicine, and Wilderness Medical Society Disclosure: Nothing to disclose. Lanny Garth Close, MD Chair, Professor, Department of Otolaryngology-Head and Neck Surgery, Columbia University College of Physicians and Surgeons Lanny Garth Close, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngology-Head and Neck Surgery, American College of Physicians, American Laryngological Association, American Society for Head and Neck Surgery, and New York Academy of Medicine Disclosure: Nothing to disclose. Cheryl D Courtlandt, MD Faculty, Department of Pediatrics, University of North Carolina at Chapel Hill School of Medicine; Medical Director, Pediatric Asthma Program, Attending Physician, Department of Pediatrics, Levine Children's Hospital, Carolinas Medical Center Cheryl D Courtlandt, MD is a member of the following medical societies: Ambulatory Pediatric Association, American Academy of Pediatrics, and National Medical Association Disclosure: Nothing to disclose. Stephen C Dreskin, MD, PhD Professor of Medicine, Departments of Internal Medicine, Director of Allergy, Asthma, and Immunology Practice, University of Colorado Health Sciences Center Stephen C Dreskin, MD, PhD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology, American Association for the Advancement of Science, American Association of Immunologists, American College of Allergy, Asthma and Immunology, Clinical Immunology Society, and Joint Council of Allergy, Asthma and Immunology
Disclosure: Genentech Consulting fee Consulting; American Health Insurance Plans Consulting fee Consulting; Johns Hopkins School of Public Health Consulting fee Consulting; Array BioPharma Consulting fee Consulting Pamela L Dyne, MD Professor of Clinical Medicine/Emergency Medicine, University of California, Los Angeles, David Geffen School of Medicine; Attending Physician, Department of Emergency Medicine, Olive View-UCLA Medical Center Pamela L Dyne, MD is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Barry J Evans, MD Assistant Professor of Pediatrics, Temple University Medical School; Director of Pediatric Critical Care and Pulmonology, Associate Chair for Pediatric Education, Temple University Children's Medical Center Barry J Evans, MD is a member of the following medical societies: American Academy of Pediatrics, American College of Chest Physicians, American Thoracic Society, and Society of Critical Care Medicine Disclosure: Nothing to disclose. Michael R Filbin, MD Clinical Instructor, Department of Emergency Medicine, Massachusetts General Hospital Michael R Filbin, MD is a member of the following medical societies: American College of Emergency Physicians, Massachusetts Medical Society, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Joseph P Garry, MD, FACSM, FAAFP Associate Professor, Sports Medicine Faculty, Department of Family and Community Medicine, University of Minnesota Medical School Joseph P Garry, MD, FACSM, FAAFP is a member of the following medical societies: American Academy of Family Physicians, American College of Sports Medicine, American Heart Association, American Medical Society for Sports Medicine, and North American Primary Care Research Group Disclosure: Nothing to disclose. Murray Grossan, MD Consulting Staff, Tower Ear, Nose and Throat Murray Grossan, MD is a member of the following medical societies: American Medical Association, American Tinnitus Association, California Medical Association, and Los Angeles County Medical Association Disclosure: Hydro Med Inc Ownership interest Management position Payel Gupta, MD Department of Allergy and Immunology, ENT Faculty Practice Payel Gupta, MD is a member of the following medical societies: American College of Physicians Disclosure: Nothing to disclose. William F Kelly III, MD Assistant Professor of Medicine, Uniformed Services University of the Health Sciences; Staff Physician, Division of Pulmonary/Critical Care Medicine, Department of Medicine, Walter Reed Army Medical Center William F Kelly III, MD is a member of the following medical societies: Alpha Omega Alpha, American College of Chest Physicians, and American College of Physicians Disclosure: Nothing to disclose. Rick Kulkarni, MD Attending Physician, Department of Emergency Medicine, Cambridge Health Alliance, Division of Emergency Medicine, Harvard Medical School
Rick Kulkarni, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy of Emergency Medicine, American College of Emergency Physicians, American Medical Association, American Medical Informatics Association, Phi Beta Kappa, and Society for Academic Emergency Medicine Disclosure: WebMD Salary Employment Eugene C Lin, MD Consulting Radiologist, Virginia Mason Medical Center; Clinical Assistant Professor of Radiology, University of Washington School of Medicine Eugene C Lin, MD is a member of the following medical societies: American College of Nuclear Medicine, American College of Radiology, Radiological Society of North America, and Society of Nuclear Medicine Disclosure: Nothing to disclose. Markus Little, MD Resident Physician, Department of Emergency Medicine, State University of New York Downstate Medical Center Disclosure: Nothing to disclose. Jeffrey A Miller, MD Associate Adjunct Professor of Clinical Radiology, University of Medicine and Dentistry of New Jersey; Faculty, Department of Radiology, Veterans Affairs of New Jersey Health Care System Jeffrey A Miller, MD is a member of the following medical societies: American Roentgen Ray Society, Society for Health Services Research in Radiology, and Society of Thoracic Radiology Disclosure: Nothing to disclose. Daniel R Neuspiel, MD, MPH, FAAP Director of Ambulatory Pediatrics, Levine Children's Hospital, Carolinas Medical Center; Adjunct Clinical Professor of Pediatrics, University of North Carolina School of Medicine Daniel R Neuspiel, MD, MPH, FAAP is a member of the following medical societies: American Academy of Pediatrics, American College of Physician Executives, American Public Health Association, New York Academy of Medicine, and Phi Beta Kappa Disclosure: Nothing to disclose. John D Newell Jr, MD Professor of Radiology, Head, Division of Radiology, National Jewish Health; Professor, Department of Radiology, University of Colorado School of Medicine John D Newell Jr, MD is a member of the following medical societies: American College of Chest Physicians, American College of Radiology, American Roentgen Ray Society, American Thoracic Society, Association of University Radiologists, Radiological Society of North America, and Society of Thoracic Radiology Disclosure: Siemens Medical Grant/research funds Consulting; Vida Corporation Ownership interest Board membership; TeraRecon Grant/research funds Consulting; eMedicine Honoraria Consulting; Humana Press Honoraria Other John J Oppenheimer, MD Clinical Associate Professor, Department of Medicine, University of Medicine and Dentistry of New Jersey; Director of Clinical Research, Pulmonary and Allergy Associates, PA John J Oppenheimer, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology and American College of Allergy, Asthma and Immunology Disclosure: AZ Consulting fee Consulting; AZ Grant/research funds Independent contractor; Glaxo Consulting fee Consulting; Glaxo Grant/research funds Independent contractor; Merck Consulting fee Consulting; Merck Grant/research funds Independent contractor; SRXA Consulting Stephen Rosenfeld, MD Professor Emeritus, Department of Medicine, Allergy, Immunology and Rheumatology Unit, University of Rochester School of Medicine and Dentistry Stephen Rosenfeld, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology, American Association of Immunologists, American Federation for Clinical Research, Clinical Immunology Society, and Medical Society of the State of New York
Immunology Society, and Medical Society of the State of New York Disclosure: Nothing to disclose. Constantine K Saadeh, MD President, Allergy ARTS, LLP; Principal Investigator, Amarillo Center for Clinical Research, Ltd Constantine K Saadeh, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology, American College of Rheumatology, American Medical Association, Southern Medical Association, and Texas Medical Association Disclosure: Nothing to disclose. Anthony J Saglimbeni, MD President, South Bay Sports and Preventive Medicine Associates; Private Practice; Team Internist, San Francisco Giants; Team Internist, West Valley College; Team Physician, Bellarmine College Prep; Team Physician, Presentation High School; Team Physician, Santa Clara University; Consultant, University of San Francisco, Academy of Art University, Skyline College, Foothill College, De Anza College Anthony J Saglimbeni, MD, is a member of the following medical societies: California Medical Association and Santa Clara County Medical Association Disclosure: Nothing to disclose. Assaad J Sayah, MD Chief, Department of Emergency Medicine, Cambridge Health Alliance Assaad J Sayah, MD is a member of the following medical societies: National Association of EMS Physicians Disclosure: Nothing to disclose. Thomas Scanlin, MD Chief, Division of Pulmonary Medicine and Cystic Fibrosis Center, Department of Pediatrics, University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School Thomas Scanlin, MD is a member of the following medical societies: American Association for the Advancement of Science, American Society for Biochemistry and Molecular Biology, American Thoracic Society, Society for Pediatric Research, and Society for Pediatric Research Disclosure: Nothing to disclose. Adam J Schwarz, MD Consulting Staff, Critical Care Division, Pediatric Subspecialty Faculty, Children's Hospital of Orange County Adam J Schwarz, MD is a member of the following medical societies: American Academy of Pediatrics and Phi Beta Kappa Disclosure: Nothing to disclose. Girish D Sharma, MD Associate Professor of Pediatrics, Rush Medical College; Director, Section of Pediatric Pulmonology and Rush Cystic Fibrosis Center, Rush University Medical Center Girish D Sharma, MD is a member of the following medical societies: American Academy of Pediatrics, American College of Chest Physicians, American Thoracic Society, and Royal College of Physicians of Ireland Disclosure: Nothing to disclose. Richard H Sinert, DO Associate Professor of Emergency Medicine, Clinical Assistant Professor of Medicine, Research Director, State University of New York College of Medicine; Consulting Staff, Department of Emergency Medicine, Kings County Hospital Center Richard H Sinert, DO is a member of the following medical societies: American College of Physicians and Society for Academic Emergency Medicine Disclosure: Nothing to disclose.
William W Storms, MD Clinical Professor, University of Colorado Health Sciences Center; Private Practice, The William Storms Allergy Clinic, Colorado Springs, Colorado Disclosure: Amgen Grant/research funds None; AstraZeneca Honoraria Consulting; AstraZeneca Honoraria Speaking and teaching; Consumer Reports/Consumer Union Honoraria Consulting; Genentech Grant/research funds None; Genentech Honoraria Consulting; Genentech Speaking and teaching; Meda Grant/research funds None; Meda Honoraria Consulting; Meda Honoraria Speaking and teaching Russell D White, MD Professor of Medicine, Professor of Orthopedic Surgery, Director of Sports Medicine Fellowship Program, Medical Director, Sports Medicine Center, Head Team Physician, University of MissouriKansas City Intercollegiate Athletic Program, Department of Community and Family Medicine, University of Missouri-Kansas City School of Medicine, Truman Medical Center-Lakewood Russell D White, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy of Family Physicians, American Association of Clinical Endocrinologists, American College of Sports Medicine, American Diabetes Association, and American Medical Society for Sports Medicine Disclosure: Nothing to disclose. Craig C Young, MD Professor, Departments of Orthopedic Surgery and Community and Family Medicine, Medical Director of Sports Medicine, Director of Primary Care Sports Medicine Fellowship, Medical College of Wisconsin Craig C Young, MD is a member of the following medical societies: American Academy of Family Physicians, American College of Sports Medicine, American Medical Society for Sports Medicine, and Phi Beta Kappa Disclosure: Nothing to disclose. Mark Zwanger, MD, MBA Assistant Professor, Department of Emergency Medicine, Jefferson Medical College of Thomas Jefferson University Mark Zwanger, MD, MBA is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, and American Medical Association Disclosure: Nothing to disclose. Specialty Editor Board Michael A Kaliner, MD Clinical Professor of Medicine, George Washington University School of Medicine; Chief, Section of Allergy and Immunology, Washington Hospital Center; Medical Director, Institute for Asthma and Allergy Michael A Kaliner, MD is a member of the following medical societies: American Academy of Allergy Asthma and Immunology, American Association of Immunologists, American College of Allergy, Asthma and Immunology, American Society for Clinical Investigation, American Thoracic Society, and Association of American Physicians Disclosure: Alcon Consulting fee Consulting; Greer Consulting fee Consulting; Sanofi Consulting fee Consulting; Schering/Merck Consulting fee Consulting; Teva Consulting fee Consulting; Meda Honoraria Speaking and teaching; Ista Consulting Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Medscape Salary Employment Robert E O'Connor, MD, MPH Professor and Chair, Department of Emergency Medicine, University of Virginia Health System Robert E O'Connor, MD, MPH is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, American College of Physician Executives, American Heart Association, American Medical Association, Medical Society of Delaware, National Association of EMS Physicians, Society for Academic Emergency Medicine, and Wilderness Medical Society
Disclosure: Nothing to disclose. Arlen D Meyers, MD, MBA Professor, Department of Otolaryngology-Head and Neck Surgery, University of Colorado School of Medicine Arlen D Meyers, MD, MBA is a member of the following medical societies: American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngology-Head and Neck Surgery, and American Head and Neck Society Disclosure: Covidien Corp Consulting fee Consulting; US Tobacco Corporation Unrestricted gift Unknown; Axis Three Corporation Ownership interest Consulting; Omni Biosciences Ownership interest Consulting; Sentegra Ownership interest Board membership; Syndicom Ownership interest Consulting; Oxlo Consulting; Medvoy Ownership interest Management position; Cerescan Imaging Honoraria Consulting; GYRUS ACMI Honoraria Consulting Chief Editor Zab Mosenifar, MD Director, Division of Pulmonary and Critical Care Medicine, Director, Women's Guild Pulmonary Disease Institute, Professor and Executive Vice Chair, Department of Medicine, Cedars Sinai Medical Center, University of California, Los Angeles, David Geffen School of Medicine Zab Mosenifar, MD is a member of the following medical societies: American College of Chest Physicians, American College of Physicians, American Federation for Medical Research, and American Thoracic Society Disclosure: Nothing to disclose. Acknowledgments The authors and editors of eMedicine gratefully acknowledge the contributions of previous authors Michael Goldman, MD, Jan Malacara, PA-C, Rohit K Katial, MD, A Antoine Kazzi, MD, Araz Marachelian, MD, and Jannette Collins, MD, MEd, FCCP, to the development and writing of the source articles.
References
1. Busse WW, Calhoun WF, Sedgwick JD. Mechanism of airway inflammation in asthma. Am Rev Respir Dis. Jun 1993;147(6 Pt 2):S20-4. [Medline]. 2. Horwitz RJ, Busse WW. Inflammation and asthma. Clin Chest Med. Dec 1995;16(4):583-602. [Medline]. 3. Murray JF, Nadel JA. Structure of the lungs relative to their principal function. In: Textbook of Respiratory Medicine. WB Saunders Co; 1988:15-20. 4. National Heart, Lung, and Blood Institute. Global Strategy for Asthma Management and Prevention. NIH Publication; 2008. 5. Balzar S, Fajt ML, Comhair SA, Erzurum SC, Bleecker E, Busse WW, et al. Mast cell phenotype, location, and activation in severe asthma: data from the severe asthma research program. Am J Respir Crit Care Med. Feb 1 2011;183(3):299-309. [Medline]. [Full Text]. 6. Gauvreau GM, Boulet LP, Cockcroft DW, et al. Effects of Interleukin-13 Blockade on Allergen-induced Airway Responses in Mild Atopic Asthma. Am J Respir Crit Care Med. Apr 15 2011;183(8):1007-14. [Medline]. 7. Anderson WJ, Watson L. Asthma and the hygiene hypothesis. N Engl J Med. May 24 2001;344(21):16434. [Medline]. 8. Sears MR. Consequences of long-term inflammation. The natural history of asthma. Clin Chest Med. Jun 2000;21(2):315-29. [Medline]. 9. Camargo CA Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med. Nov 22 1999;159(21):2582-8. [Medline]. 10. Henderson WR Jr. Role of leukotrienes in asthma. Ann Allergy. Mar 1994;72(3):272-8. [Medline].
11. Beasley RW, Clayton TO, Crane J, Lai CK, Montefort SR, Mutius E, et al. Acetaminophen use and risk of asthma, rhinoconjunctivitis, and eczema in adolescents: international study of asthma and allergies in childhood phase three. Am J Respir Crit Care Med. Jan 15 2011;183(2):171-8. [Medline]. 12. Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med. Jul 2000;162(1):34-9. [Medline]. 13. Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, et al. Diagnosis and management of work-related asthma: American College Of Chest Physicians Consensus Statement. Chest. Sep 2008;134(3 Suppl):1S-41S. [Medline]. 14. Lemanske RF Jr, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, et al. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol. Sep 2005;116(3):571-7. [Medline]. 15. Bizzintino J, Lee WM, Laing IA, Vang F, Pappas T, Zhang G, et al. Association between human rhinovirus C and severity of acute asthma in children. Eur Respir J. May 2011;37(5):1037-42. [Medline]. [Full Text]. 16. Martin RJ, Kraft M, Chu HW, Berns EA, Cassell GH. A link between chronic asthma and chronic infection. J Allergy Clin Immunol. Apr 2001;107(4):595-601. [Medline]. 17. Hamilos DL. Gastroesophageal reflux and sinusitis in asthma. Clin Chest Med. Dec 1995;16(4):683-97. [Medline]. 18. McFadden ER Jr. Exercise-induced airway obstruction. Clin Chest Med. Dec 1995;16(4):671-82. [Medline]. 19. Randolph C. Exercise-induced asthma: update on pathophysiology, clinical diagnosis, and treatment. Curr Probl Pediatr. Feb 1997;27(2):53-77. [Medline]. 20. Ito S, Noguchi E, Shibasaki M, Yamakawa-Kobayashi K, Watanabe H, Arinami T. Evidence for an association between plasma platelet-activating factor acetylhydrolase deficiency and increased risk of childhood atopic asthma. J Hum Genet. 2002;47(2):99-101. [Medline]. 21. Bousquet J, Jeffery PK, Busse WW, Johnson M, Vignola AM. Asthma. From bronchoconstriction to airways inflammation and remodeling. Am J Respir Crit Care Med. May 2000;161(5):1720-45. [Medline]. 22. Zucker, M. Asthma phenotype, genotype may guide future therapies. Available at http://www.pulmonaryreviews.com/jun03/pr_jun03_phenotype.html. Accessed June 8, 2003. 23. Drazen JM, Yandava CN, Dube L, Szczerback N, Hippensteel R, Pillari A, et al. Pharmacogenetic association between ALOX5 promoter genotype and the response to anti-asthma treatment. Nat Genet. Jun 1999;22(2):168-70. [Medline]. 24. Thompson EE, Pan L, Ostrovnaya I, Weiss LA, Gern JE, Lemanske RF Jr, et al. Integrin beta 3 genotype influences asthma and allergy phenotypes in the first 6 years of life. J Allergy Clin Immunol. Jun 2007;119(6):1423-9. [Medline]. 25. Wechsler ME, Lehman E, Lazarus SC, Lemanske RF Jr, Boushey HA, Deykin A, et al. beta-Adrenergic receptor polymorphisms and response to salmeterol. Am J Respir Crit Care Med. Mar 1 2006;173(5):51926. [Medline]. [Full Text]. 26. Cottrell L, Neal WA, Ice C, Perez MK, Piedimonte G. Metabolic abnormalities in children with asthma. Am J Respir Crit Care Med. Feb 15 2011;183(4):441-8. [Medline]. [Full Text]. 27. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. Jan 2008;31(1):143-78. [Medline]. [Full Text]. 28. Zhang Y, McConnell R, Gilliland F, Berhane K. Ethnic differences in the effect of asthma on pulmonary function in children. Am J Respir Crit Care Med. Mar 1 2011;183(5):596-603. [Medline]. [Full Text]. 29. Burrows B, Barbee RA, Cline MG, Knudson RJ, Lebowitz MD. Characteristics of asthma among elderly adults in a sample of the general population. Chest. Oct 1991;100(4):935-42. [Medline].
30. Martin AJ, Landau LI, Phelan PD. Lung function in young adults who had asthma in childhood. Am Rev Respir Dis. Oct 1980;122(4):609-16. [Medline]. 31. Sly RM. Changing asthma mortality. Ann Allergy. Sep 1994;73(3):259-68. [Medline]. 32. Moorman JE, Rudd RA, Johnson CA, King M, Minor P, Bailey C, et al. National surveillance for asthma-United States, 1980-2004. MMWR Surveill Summ. Oct 19 2007;56(8):1-54. [Medline]. 33. National Heart, Lung, and Blood Institute Chartbook on Cardiovascular, Lung, and BloodDiseases, U.S. Department of Health and Human Services, et al. 2009. Available at http://www.nhlbi.nih.gov/resources/docs/2009_ChartBook.pdf. 34. [Guideline] Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of AsthmaSummary Report 2007. J Allergy Clin Immunol. Nov 2007;120(5 Suppl):S94-138. [Medline]. 35. Bailey WC, Richards JM Jr, Brooks CM, Soong SJ, Windsor RA, Manzella BA. A randomized trial to improve self-management practices of adults with asthma. Arch Intern Med. Aug 1990;150(8):1664-8. [Medline]. 36. Ignacio-Garcia JM, Gonzalez-Santos P. Asthma self-management education program by home monitoring of peak expiratory flow. Am J Respir Crit Care Med. Feb 1995;151(2 Pt 1):353-9. [Medline]. 37. Kotses H, Bernstein IL, Bernstein DI, Reynolds RV, Korbee L, Wigal JK, et al. A self-management program for adult asthma. Part I: Development and evaluation. J Allergy Clin Immunol. Feb 1995;95(2):529-40. [Medline]. 38. Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. Jan 2004;113(1):59-65. [Medline]. 39. [Best Evidence] Coffman JM, Cabana MD, Yelin EH. Do school-based asthma education programs improve self-management and health outcomes?. Pediatrics. Aug 2009;124(2):729-42. [Medline]. [Full Text]. 40. Management of Asthma Working Group. VA/DoD clinical practice guideline for management of asthma in children and adults. Washington (DC): Department of Veteran Affairs, Department of Defense; 2009:[Full Text]. 41. Font-Ribera L, Villanueva CM, Nieuwenhuijsen MJ, et al. Swimming pool attendance, asthma, allergies, and lung function in the Avon Longitudinal Study of Parents and Children cohort. Am J Respir Crit Care Med. Mar 1 2011;183(5):582-8. [Medline]. [Full Text]. 42. From the Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) 2010. Available at http://www.ginasthma.org. 43. Shao W, Chung T, Berdon WE, Mellins RB, Griscom NT, Ruzal-Shapiro C, et al. Fluoroscopic diagnosis of laryngeal asthma (paradoxical vocal cord motion). AJR Am J Roentgenol. Nov 1995;165(5):1229-31. [Medline]. 44. Morris MJ, Deal LE, Bean DR, Grbach VX, Morgan JA. Vocal cord dysfunction in patients with exertional dyspnea. Chest. Dec 1999;116(6):1676-82. [Medline]. 45. Nastasi KJ, Howard DA, Raby RB, Lew DB, Blaiss MS. Airway fluoroscopic diagnosis of vocal cord dysfunction syndrome. Ann Allergy Asthma Immunol. Jun 1997;78(6):586-8. [Medline]. 46. Wynn SR, O'Connell EJ, Frigas E, Payne WS, Sachs MI. Exercise-induced "asthma" as a presentation of bronchial carcinoid. Ann Allergy. Aug 1986;57(2):139-41. [Medline]. 47. Rolfe LM, Rayner CF. A wheezy man with a bony abnormality. Postgrad Med J. Aug 1999;75(886):503-4. [Medline]. [Full Text]. 48. Tucker GF Jr. Pulmonary migraine. Ann Otol Rhinol Laryngol. Sep-Oct 1977;86(5 Pt 1):671-6. [Medline]. 49. Isselbacher KJ. Harrison's Principles of Internal Medicine. In: Braunwald E, Wilson JD, et al. Heart failure. 13th. McGraw-Hill; 1994:1001.
50. Kim YW, Han SK, Shim YS, Kim KY, Han YC, Seo JW, et al. The first report of diffuse panbronchiolitis in Korea: five case reports. Intern Med. May 1992;31(5):695-701. [Medline]. 51. Bevelaqua F, Schicchi JS, Haas F, Axen K, Levin N. Aortic arch anomaly presenting as exercise-induced asthma. Am Rev Respir Dis. Sep 1989;140(3):805-8. [Medline]. 52. Newman LJ, Platts-Mills TA, Phillips CD, Hazen KC, Gross CW. Chronic sinusitis. Relationship of computed tomographic findings to allergy, asthma, and eosinophilia. JAMA. Feb 2 1994;271(5):363-7. [Medline]. 53. Shapiro GG, Christie DL. Gastroesophageal reflux and asthma. Clin Rev Allergy. Mar 1983;1(1):39-56. [Medline]. 54. Cuevas Hernndez MM, Arias Hernndez RM. [Pulmonary gammagraphy study in asthmatic children with gastroesophageal reflux]. Rev Alerg Mex. Nov-Dec 2008;55(6):229-33. [Medline]. 55. Bacci E, Cianchetti S, Bartoli M, Dente FL, Di Franco A, Vagaggini B, et al. Low sputum eosinophils predict the lack of response to beclomethasone in symptomatic asthmatic patients. Chest. Mar 2006;129(3):565-72. [Medline]. 56. Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, et al. Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet. Nov 30 2002;360(9347):1715-21. [Medline]. 57. Woods AQ, Lynch DA. Asthma: an imaging update. Radiol Clin North Am. Mar 2009;47(2):317-29. [Medline]. 58. Teel GS, Engeler CE, Tashijian JH, duCret RP. Imaging of small airways disease. Radiographics. Jan 1996;16(1):27-41. [Medline]. 59. Enright PL, Lebowitz MD, Cockroft DW. Physiologic measures: pulmonary function tests. Asthma outcome. Am J Respir Crit Care Med. Feb 1994;149(2 Pt 2):S9-18; discussion S19-20. [Medline]. 60. Ali SS, O'Connell C, Kass L, Graff G. Single-breath counting: a pilot study of a novel technique for measuring pulmonary function in children. Am J Emerg Med. Jan 2011;29(1):33-6. [Medline]. 61. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. Jan 2000;161(1):309-29. [Medline]. 62. Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med. May 26 2005;352(21):2163-73. [Medline]. 63. Rossi OV, Lhde S, Laitinen J, Huhti E. Contribution of chest and paranasal sinus radiographs to the management of acute asthma. Int Arch Allergy Immunol. Sep 1994;105(1):96-100. [Medline]. 64. Pratter MR, Curley FJ, Dubois J, Irwin RS. Cause and evaluation of chronic dyspnea in a pulmonary disease clinic. Arch Intern Med. Oct 1989;149(10):2277-82. [Medline]. 65. Irwin RS. Chronic cough due to gastroesophageal reflux disease: ACCP evidence-based clinical practice guidelines. Chest. Jan 2006;129(1 Suppl):80S-94S. [Medline]. 66. Price D, Musgrave SD, Shepstone L, et al. Leukotriene antagonists as first-line or add-on asthmacontroller therapy. N Engl J Med. May 5 2011;364(18):1695-707. [Medline]. 67. Bruzzese JM, Sheares BJ, Vincent EJ, et al. Effects of a School-based Intervention for Urban Adolescents with Asthma: A Controlled Trial. Am J Respir Crit Care Med. Apr 15 2011;183(8):998-1006. [Medline]. [Full Text]. 68. National Heart, Lung, and Blood Institute. Education for a partnership in asthma care. Expert panel report 3: guidelines for the diagnosis and management of asthma. National Asthma Education and Prevention Program (NAEPP). Aug 2007. 69. Berridge MS, Lee Z, Heald DL. Pulmonary distribution and kinetics of inhaled [11C]triamcinolone acetonide. J Nucl Med. Oct 2000;41(10):1603-11. [Medline].
70. Nelson HS. Advair: combination treatment with fluticasone propionate/salmeterol in the treatment of asthma. J Allergy Clin Immunol. Feb 2001;107(2):398-416. [Medline]. 71. McCormack MC, Breysse PN, Matsui EC, et al. Indoor particulate matter increases asthma morbidity in children with non-atopic and atopic asthma. Ann Allergy Asthma Immunol. Apr 2011;106(4):308-15. [Medline]. 72. Tung KY, Tsai CH, Lee YL. Microsomal epoxide hydroxylase genotypes/diplotypes, traffic air pollution, and childhood asthma. Chest. Apr 2011;139(4):839-48. [Medline]. 73. Sheikh A, Hurwitz B, Shehata Y. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. Jan 24 2007;CD001563. [Medline]. 74. Abramson MJ, Puy RM, Weiner JM. Allergen immunotherapy for asthma. Cochrane Database Syst Rev. 2003;CD001186. [Medline]. 75. Abramson MJ, Puy RM, Weiner JM. Is allergen immunotherapy effective in asthma? A meta-analysis of randomized controlled trials. Am J Respir Crit Care Med. Apr 1995;151(4):969-74. [Medline]. 76. Bruggenjurgen B, Reinhold T, Brehler R, Laake E, Wiese G, Machate U, et al. Cost-effectiveness of specific subcutaneous immunotherapy in patients with allergic rhinitis and allergic asthma. Ann Allergy Asthma Immunol. Sep 2008;101(3):316-24. [Medline]. 77. Marcus P. Incorporating anti-IgE (omalizumab) therapy into pulmonary medicine practice: practice management implications. Chest. Feb 2006;129(2):466-74. [Medline]. 78. Busse WW, Morgan WJ, Gergen PJ, et al. Randomized trial of omalizumab (anti-IgE) for asthma in innercity children. N Engl J Med. Mar 17 2011;364(11):1005-15. [Medline]. [Full Text]. 79. Hanania NA, Alpan O, Hamilos DL, et al. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann Intern Med. May 3 2011;154(9):573-82. [Medline]. 80. [Best Evidence] Castro M, Rubin AS, Laviolette M, Fiterman J, De Andrade Lima M, Shah PL, et al. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir Crit Care Med. Jan 15 2010;181(2):116-24. [Medline]. 81. O'Byrne PM, Pedersen S, Carlsson LG, et al. Risks of pneumonia in patients with asthma taking inhaled corticosteroids. Am J Respir Crit Care Med. Mar 1 2011;183(5):589-95. [Medline]. 82. Dhuper S, Chandra A, Ahmed A, et al. Efficacy and cost comparisons of bronchodilatator administration between metered dose inhalers with disposable spacers and nebulizers for acute asthma treatment. J Emerg Med. Mar 2011;40(3):247-55. [Medline]. 83. Rowe BH, Keller JL, Oxman AD. Effectiveness of steroid therapy in acute exacerbations of asthma: a meta-analysis. Am J Emerg Med. Jul 1992;10(4):301-10. [Medline]. 84. Rowe BH, Edmonds ML, Spooner CH, Diner B, Camargo CA Jr. Corticosteroid therapy for acute asthma. Respir Med. Apr 2004;98(4):275-84. [Medline]. 85. Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budesonide on adult height in children with asthma. N Engl J Med. Oct 12 2000;343(15):1064-9. [Medline]. 86. Tastepe AI, Kuzucu A, Demircan S, Liman ST, Demirag F. Surgical treatment of tracheal hamartoma. Scand Cardiovasc J. 1998;32(4):239-41. [Medline]. 87. [Best Evidence] Guilbert TW, Morgan WJ, Zeiger RS, Mauger DT, Boehmer SJ, Szefler SJ, et al. Longterm inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med. May 11 2006;354(19):1985-97. [Medline]. 88. van den Berge M, ten Hacken NH, Cohen J, Douma WR, Postma DS. Small airway disease in asthma and COPD: clinical implications. Chest. Feb 2011;139(2):412-23. [Medline]. 89. Kingston HG, Hirshman CA. Perioperative management of the patient with asthma. Anesth Analg. Sep 1984;63(9):844-55. [Medline].
90. Peters SP, Kunselman SJ, Icitovic N, Moore WC, Pascual R, Ameredes BT, et al. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med. Oct 28 2010;363(18):1715-26. [Medline]. [Full Text]. 91. Abdullah AK, Danial BH, Zeid A, Chaikhouni A, Ejeckam GC. Solitary bronchial papilloma presenting with recurrent dyspnea attacks: case report with computed tomography findings. Respiration. 1991;58(1):62-4. [Medline]. 92. Altes TA, Powers PL, Knight-Scott J, Rakes G, Platts-Mills TA, de Lange EE, et al. Hyperpolarized 3He MR lung ventilation imaging in asthmatics: preliminary findings. J Magn Reson Imaging. Mar 2001;13(3):378-84. [Medline]. 93. Braman SS, Davis SM. Wheezing in the elderly. Asthma and other causes. Clin Geriatr Med. May 1986;2(2):269-83. [Medline]. 94. Chen Q, Jakob PM, Griswold MA, Levin DL, Hatabu H, Edelman RR. Oxygen enhanced MR ventilation imaging of the lung. MAGMA. Dec 1998;7(3):153-61. [Medline]. 95. Corren J, Tashkin DP. Evaluation of efficacy and safety of flunisolide hydrofluoroalkane for the treatment of asthma. Clin Ther. Mar 2003;25(3):776-98. [Medline]. 96. Current Asthma Population Estimates -- in thousands by Age, United States: National Health Interview Survey, 2008. Available at http://www.cdc.gov/asthma/nhis/08/table3-1.htm. Accessed March 25, 2010. 97. de Lange EE, Altes TA, Patrie JT, Battiston JJ, Juersivich AP, Mugler JP 3rd, et al. Changes in regional airflow obstruction over time in the lungs of patients with asthma: evaluation with 3He MR imaging. Radiology. Feb 2009;250(2):567-75. [Medline]. 98. de Lange EE, Mugler JP 3rd, Brookeman JR, Knight-Scott J, Truwit JD, Teates CD, et al. Lung air spaces: MR imaging evaluation with hyperpolarized 3He gas. Radiology. Mar 1999;210(3):851-7. [Medline]. 99. Devadason SG, Huang T, Walker S, Troedson R, Le Souf PN. Distribution of technetium-99m-labelled QVAR delivered using an Autohaler device in children. Eur Respir J. Jun 2003;21(6):1007-11. [Medline]. 100. Dolovich MB. Measuring total and regional lung deposition using inhaled radiotracers. J Aerosol Med. 2001;14 Suppl 1:S35-44. [Medline]. 101. [Guideline] Dombrowski MP, Schatz M. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 90, February 2008: asthma in pregnancy. Obstet Gynecol. Feb 2008;111(2 Pt 1):457-64. [Medline]. 102. FDA Announces. New Safety Controls for Long-Acting Beta Agonists, Medications Used to Treat Asthma. Available at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm200931.htm. Accessed March 25, 2010. 103. Hatch RT, Parker JM, Engler RJ. Wheezing, hypoxia, and dyspnea in a 62-year-old woman. Ann Allergy. May 1993;70(5):363-7. [Medline]. 104. Hirst PH, Pitcairn GR, Weers JG, Tarara TE, Clark AR, Dellamary LA, et al. In vivo lung deposition of hollow porous particles from a pressurized metered dose inhaler. Pharm Res. Mar 2002;19(3):258-64. [Medline]. 105. Hirst RH, Newman SR, Clark DA, Hertog MG. Lung deposition of budesonide from the novel dry powder inhaler Airmax. Respir Med. Jun 2002;96(6):389-96. [Medline]. 106. Janahi I, Fan LL. Bronchogenic cyst masquerading as asthma. J Pediatr. Jul 1998;133(1):166. [Medline]. 107. Jones HA, Marino PS, Shakur BH, Morrell NW. In vivo assessment of lung inflammatory cell activity in patients with COPD and asthma. Eur Respir J. Apr 2003;21(4):567-73. [Medline]. 108. Kaya M, Salan A, Tabakoglu E, Aydogdu N, Berkarda S. The bronchoalveolar epithelial permeability in house painters as determined by Tc-99m DTPA aerosol scintigraphy. Ann Nucl Med. Jun 2003;17(4):3058. [Medline]. 109. Khanijo V, Del Giacco DR, Poggi JA, Hussain MN, Harris TM. Left mainstem bronchus narrowing in an
asthmatic patient. Chest. May 1982;81(5):635-6. [Medline]. 110. King GG, Muller NL, Pare PD. Evaluation of airways in obstructive pulmonary disease using highresolution computed tomography. Am J Respir Crit Care Med. Mar 1999;159(3):992-1004. [Medline]. 111. Long-term effects of budesonide or nedocromil in children with asthma. The Childhood Asthma Management Program Research Group. N Engl J Med. Oct 12 2000;343(15):1054-63. [Medline]. 112. Martin RJ. Therapeutic significance of distal airway inflammation in asthma. J Allergy Clin Immunol. Feb 2002;109(2 Suppl):S447-60. [Medline]. 113. [Best Evidence] Nair P, Pizzichini MM, Kjarsgaard M, Inman MD, Efthimiadis A, Pizzichini E, et al. Mepolizumab for prednisone-dependent asthma with sputum eosinophilia. N Engl J Med. Mar 5 2009;360(10):985-93. [Medline]. 114. Nayak A. A review of montelukast in the treatment of asthma and allergic rhinitis. Expert Opin Pharmacother. Mar 2004;5(3):679-86. [Medline]. 115. Neeld DA, Goodman LR, Gurney JW, Greenberger PA, Fink JN. Computerized tomography in the evaluation of allergic bronchopulmonary aspergillosis. Am Rev Respir Dis. Nov 1990;142(5):1200-5. [Medline]. 116. [Best Evidence] Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM. The Salmeterol Multicenter Asthma Research Trial: a comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest. Jan 2006;129(1):15-26. [Medline]. 117. Newman SP. Can lung deposition data act as a surrogate for the clinical response to inhaled asthma drugs?. Br J Clin Pharmacol. Jun 2000;49(6):529-37. [Medline]. [Full Text]. 118. Newman SP, Pitcairn GR, Adkin DA, Vidgren MT, Silvasti M. Comparison of beclomethasone dipropionate delivery by easyhaler dry powder inhaler and pMDI plus large volume spacer. J Aerosol Med. Summer 2001;14(2):217-25. [Medline]. 119. Ohno Y, Chen Q, Hatabu H. Oxygen-enhanced magnetic resonance ventilation imaging of lung. Eur J Radiol. Mar 2001;37(3):164-71. [Medline]. 120. Olazbal F Jr, Romn-Irizarry LA, Oms JD, Conde L, Marchand EJ. Pulmonary emboli masquerading as asthma. N Engl J Med. May 2 1968;278(18):999-1001. [Medline]. 121. Park SS, Shin DH, Lee DH, Jeon SC, Lee JH, Lee JD. Tracheopathia osteoplastica simulating asthmatic symptoms. Diagnosis by bronchoscopy and computerized tomography. Respiration. 1995;62(1):43-5. [Medline]. 122. Perol M, Brun P, Arnouk H, Bayle JY, Guerin JC. [Bronchospasm disclosing pulmonary embolism]. Rev Pneumol Clin. 1990;46(5):225-8. [Medline]. 123. Reittner P, Muller NL. Tracheal hamartoma: CT findings in two patients. J Comput Assist Tomogr. NovDec 1999;23(6):957-8. [Medline]. 124. Saari SM, Vidgren MT, Herrala J, Turjanmaa VM, Koskinen MO, Nieminen MM. Possibilities of formoterol to enhance the peripheral lung deposition of the inhaled liposome corticosteroids. Respir Med. Dec 2002;96(12):999-1005. [Medline]. 125. Shirakawa T, Takenaka S, Matsumoto T, Hirata N, Nishimura S, Fukuda K, et al. [A case of leiomyoma of the trachea]. Nihon Kyobu Shik k an Gak k ai Zasshi. Nov 1991;29(11):1464-8. [Medline]. 126. Spivey CG Jr, Walsh RE, Perez-Guerra F, Harkleroad LE. Central airway obstruction. Report of seven cases. JAMA. Dec 3 1973;226(10):1186-9. [Medline]. 127. Weiner DJ, Weatherly RA, DiPietro MA, Sanders GM. Tracheal schwannoma presenting as status asthmaticus in a sixteen-year-old boy: airway considerations and removal with the CO2 laser. Pediatr Pulmonol. Jun 1998;25(6):393-7. [Medline]. 128. Yuksel H, Yuksel D, Demir E, Tanac R, Kayaliodlu M. Effect of inhaled steroid therapy on distribution of Tc-99m DTPA radioaerosol in asthmatic children. Allergy Asthma Proc. Nov-Dec 2000;21(6):361-5. [Medline].
Das könnte Ihnen auch gefallen
- Asthma: A. Practice EssentialsDokument8 SeitenAsthma: A. Practice EssentialsCandha NurcahyaNoch keine Bewertungen
- ASTHMADokument17 SeitenASTHMAvinda astri permatasariNoch keine Bewertungen
- Rudy Haynes - Deep Voice Mastery 2nd EdDokument36 SeitenRudy Haynes - Deep Voice Mastery 2nd EdIram Rana100% (2)
- Cestodes (Table)Dokument3 SeitenCestodes (Table)Marelle M. Yamzon87% (15)
- AsthmaDokument46 SeitenAsthmaHafiz Muhammad AeymonNoch keine Bewertungen
- Acute Severe AsthmaDokument5 SeitenAcute Severe AsthmaRizsa Aulia DanestyNoch keine Bewertungen
- 7B Reproduction WorksheetDokument11 Seiten7B Reproduction WorksheetSuttada0% (1)
- Asthma + COPD (Full)Dokument115 SeitenAsthma + COPD (Full)selamsew alemuNoch keine Bewertungen
- Bronchial AsthmaDokument34 SeitenBronchial AsthmaFabb NelsonNoch keine Bewertungen
- Zrad The Necromancer SpellsDokument2 SeitenZrad The Necromancer SpellsstarnilNoch keine Bewertungen
- Clinical Trial Conduct and MonitoringDokument129 SeitenClinical Trial Conduct and MonitoringDnyanesh LimayeNoch keine Bewertungen
- Chapter 10 Interstitial Lung DiseaseDokument10 SeitenChapter 10 Interstitial Lung DiseaseAleksandar Tasic100% (1)
- Bronchial Asthma I. Objectives: A. U: - Espiratory InfectionsáDokument5 SeitenBronchial Asthma I. Objectives: A. U: - Espiratory InfectionsáEnah EvangelistaNoch keine Bewertungen
- The Lesser Writings of Von Boenninghausen 1000055197Dokument361 SeitenThe Lesser Writings of Von Boenninghausen 1000055197Frank NavaNoch keine Bewertungen
- Asthma: Practice EssentialsDokument12 SeitenAsthma: Practice EssentialsIda WilonaNoch keine Bewertungen
- Pathophysiology of AsthmaDokument71 SeitenPathophysiology of AsthmaChin ChanNoch keine Bewertungen
- BackgroundDokument18 SeitenBackgroundsanasharNoch keine Bewertungen
- Asthma: Signs and SymptomsDokument57 SeitenAsthma: Signs and SymptomsAjp Ryuzaki CaesarNoch keine Bewertungen
- Asthma 1Dokument8 SeitenAsthma 1Salman KhanNoch keine Bewertungen
- The Potential of Biologics For The Treatment of Asthma: Girolamo Pelaia, Alessandro Vatrella and Rosario MaselliDokument15 SeitenThe Potential of Biologics For The Treatment of Asthma: Girolamo Pelaia, Alessandro Vatrella and Rosario MaselliSanjeev SaxenaNoch keine Bewertungen
- Sam CD Asthma ReciveredDokument36 SeitenSam CD Asthma ReciveredDr. Muha. Hasan Mahbub-Ur-RahmanNoch keine Bewertungen
- Asthma Bahan Bacaan LengkapDokument18 SeitenAsthma Bahan Bacaan LengkapBambang PutraNoch keine Bewertungen
- Asma Bronkial CUTE 2018 Dr. TeguhDokument50 SeitenAsma Bronkial CUTE 2018 Dr. TeguhAthari AdityaNoch keine Bewertungen
- Case Vignette Analysis (Pediatric Case) I. QuestionsDokument2 SeitenCase Vignette Analysis (Pediatric Case) I. QuestionsMadelaine EvangelioNoch keine Bewertungen
- An Assignment On Pathophysiology and Drug Therapy of Respiratory Disorders. byDokument34 SeitenAn Assignment On Pathophysiology and Drug Therapy of Respiratory Disorders. byShaik ShoaibNoch keine Bewertungen
- Content On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YearDokument11 SeitenContent On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YeargopscharanNoch keine Bewertungen
- Astm SeverDokument18 SeitenAstm SeverCristian GrigorasNoch keine Bewertungen
- Update On Severe Asthma: What We Know and What We NeedDokument8 SeitenUpdate On Severe Asthma: What We Know and What We Needtaksim2011Noch keine Bewertungen
- Pathophysiology of Asthma - StatPearls - NCBI BookshelfDokument7 SeitenPathophysiology of Asthma - StatPearls - NCBI BookshelfJEAN CERNA SOLISNoch keine Bewertungen
- Neutrophils and Asthma: J MonteseirínDokument15 SeitenNeutrophils and Asthma: J MonteseirínRupa2811Noch keine Bewertungen
- Allergy-Asthma ConnectionDokument11 SeitenAllergy-Asthma ConnectionLaras Bani WasesoNoch keine Bewertungen
- Zhu 18 05Dokument8 SeitenZhu 18 05ABNoch keine Bewertungen
- BCP 0372 PDFDokument8 SeitenBCP 0372 PDFPoetri LaelahNoch keine Bewertungen
- Immunology of Asthma and Chronic Obstructive Pulmonary DiseaseDokument10 SeitenImmunology of Asthma and Chronic Obstructive Pulmonary DiseaseClaudio Luis VenturiniNoch keine Bewertungen
- Bronchial AsthmaDokument84 SeitenBronchial AsthmaNavnik NaithikNoch keine Bewertungen
- Pa Tho Physiology of AsthmaDokument18 SeitenPa Tho Physiology of AsthmaNeil-Vince ConejosNoch keine Bewertungen
- Manejo de Status AsmaticoDokument17 SeitenManejo de Status Asmaticobuqmir6977Noch keine Bewertungen
- Ajprm v9 Id1085Dokument8 SeitenAjprm v9 Id1085Maira IrshadNoch keine Bewertungen
- NCM 64 Care of Client For Feb 14Dokument12 SeitenNCM 64 Care of Client For Feb 14ampalNoch keine Bewertungen
- Definisi AsmaDokument12 SeitenDefinisi AsmaDayu Punik ApsariNoch keine Bewertungen
- Treatment of AsthmaDokument22 SeitenTreatment of AsthmaMedranoReyesLuisinNoch keine Bewertungen
- AsthmaDokument5 SeitenAsthmaabenezer isayasNoch keine Bewertungen
- AshtmaDokument95 SeitenAshtmaObsa JemalNoch keine Bewertungen
- Pone 0062827Dokument12 SeitenPone 0062827Tiffany NurzamanNoch keine Bewertungen
- Asthma Case PresentationDokument3 SeitenAsthma Case Presentationfernandezrachelle44Noch keine Bewertungen
- AsthmaDokument79 SeitenAsthmaraj patel100% (1)
- Airway Inflammation and Remodelling in Asthma - Cause and Effect?Dokument13 SeitenAirway Inflammation and Remodelling in Asthma - Cause and Effect?Pauroosh KaushalNoch keine Bewertungen
- Child Hood Asthma: Kussia .A (MD)Dokument45 SeitenChild Hood Asthma: Kussia .A (MD)Yemata HailuNoch keine Bewertungen
- Asthma Thesis TopicsDokument5 SeitenAsthma Thesis Topicsgjfcp5jb100% (1)
- Immunology of Asthma and ChronicDokument10 SeitenImmunology of Asthma and ChronicMeldaNoch keine Bewertungen
- New Insights Into The Relationship Between Airway Inflammation and AsthmaDokument11 SeitenNew Insights Into The Relationship Between Airway Inflammation and Asthmaapi-3736350Noch keine Bewertungen
- Obstructive Lung Diseases - Slides English-1Dokument24 SeitenObstructive Lung Diseases - Slides English-1Baqir BroNoch keine Bewertungen
- Bronchial Asthma: Mrs. Smitha. M Associate Professor Vijaya College of Nursing KottarakkaraDokument8 SeitenBronchial Asthma: Mrs. Smitha. M Associate Professor Vijaya College of Nursing KottarakkaraSobha ajoNoch keine Bewertungen
- Chronic Obstructive Pulmonary DiseasesDokument7 SeitenChronic Obstructive Pulmonary DiseasesGeoffreyNoch keine Bewertungen
- Status AsthmaticusDokument11 SeitenStatus AsthmaticussuluckyimonaunguumNoch keine Bewertungen
- Asthama - Pathology and PathophysiologyDokument5 SeitenAsthama - Pathology and PathophysiologyTejal ParulkarNoch keine Bewertungen
- Chapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPDokument19 SeitenChapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPgireeshsachinNoch keine Bewertungen
- Status AsthmaticsDokument12 SeitenStatus AsthmaticsYash RamawatNoch keine Bewertungen
- The Role of Cytokines in Atopic AsthmaDokument13 SeitenThe Role of Cytokines in Atopic AsthmaDyan TonyNoch keine Bewertungen
- Asthma: Review Open AccessDokument9 SeitenAsthma: Review Open AccessKarthik VelletiNoch keine Bewertungen
- Concise Clinical Review: Role of Biologics in AsthmaDokument13 SeitenConcise Clinical Review: Role of Biologics in AsthmaHossam HamzaNoch keine Bewertungen
- Up To Date. Asthma PathogenesisDokument22 SeitenUp To Date. Asthma PathogenesisGuardito PequeñoNoch keine Bewertungen
- Jurnal CDCDokument9 SeitenJurnal CDCPutri WafiroNoch keine Bewertungen
- AsthmaDokument3 SeitenAsthmabholuNoch keine Bewertungen
- Feline Asthma: A Pathophysiologic Basis of TherapyDokument5 SeitenFeline Asthma: A Pathophysiologic Basis of TherapyEnnur NufianNoch keine Bewertungen
- Diagnosis and Treatment of Chronic CoughVon EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNoch keine Bewertungen
- Bachelor of Science in Pharmed (Pharmaceutical and Medical Sciences) / Medical SciencesDokument2 SeitenBachelor of Science in Pharmed (Pharmaceutical and Medical Sciences) / Medical SciencesDnyanesh LimayeNoch keine Bewertungen
- Flyer PharmaDokument2 SeitenFlyer PharmaDnyanesh LimayeNoch keine Bewertungen
- CAHS I CardDokument1 SeiteCAHS I CardDnyanesh LimayeNoch keine Bewertungen
- Flyer PharmaDokument2 SeitenFlyer PharmaDnyanesh LimayeNoch keine Bewertungen
- Centre For Advancement in Health SciencesDokument2 SeitenCentre For Advancement in Health SciencesDnyanesh LimayeNoch keine Bewertungen
- Group 5 Pubmed Accepted Results PDFDokument683 SeitenGroup 5 Pubmed Accepted Results PDFDnyanesh LimayeNoch keine Bewertungen
- CDP - Design Decisions & Trial Design - 4-Jul-10Dokument67 SeitenCDP - Design Decisions & Trial Design - 4-Jul-10Dnyanesh LimayeNoch keine Bewertungen
- Bachelor of Science in Pharmed (Pharmaceutical and Medical Sciences) / Medical SciencesDokument2 SeitenBachelor of Science in Pharmed (Pharmaceutical and Medical Sciences) / Medical SciencesDnyanesh LimayeNoch keine Bewertungen
- Phamacist and Renal DiseaseDokument11 SeitenPhamacist and Renal DiseaseDnyanesh Limaye100% (1)
- CDP - Design Decisions & Trial Design - 4-Jul-10Dokument67 SeitenCDP - Design Decisions & Trial Design - 4-Jul-10Dnyanesh LimayeNoch keine Bewertungen
- Copyrform DLDokument1 SeiteCopyrform DLDnyanesh LimayeNoch keine Bewertungen
- Bio-Business in Brief: The Challenges of Clinical TrialsDokument9 SeitenBio-Business in Brief: The Challenges of Clinical TrialsDnyanesh LimayeNoch keine Bewertungen
- Pharmacist and Oral DiseaseDokument10 SeitenPharmacist and Oral DiseaseDnyanesh LimayeNoch keine Bewertungen
- Apartment BookingDokument1 SeiteApartment BookingDnyanesh LimayeNoch keine Bewertungen
- Medication History Group 5Dokument1 SeiteMedication History Group 5Dnyanesh LimayeNoch keine Bewertungen
- Pharmacist and Medication History GR 5Dokument1 SeitePharmacist and Medication History GR 5Dnyanesh LimayeNoch keine Bewertungen
- Hahyp: Hsh123 Versus Abc456 in Treatment of HypertensionDokument15 SeitenHahyp: Hsh123 Versus Abc456 in Treatment of HypertensionDnyanesh LimayeNoch keine Bewertungen
- Advertisement Review Checklist: CompanyDokument1 SeiteAdvertisement Review Checklist: CompanyDnyanesh LimayeNoch keine Bewertungen
- Guntur Projects StatusDokument1 SeiteGuntur Projects StatusDnyanesh LimayeNoch keine Bewertungen
- Important Websites DailyDokument1 SeiteImportant Websites DailyDnyanesh LimayeNoch keine Bewertungen
- Knowledge, Attitudes, and Perception Towards Human Papilloma Virus Among University Students in Mumbai, IndiaDokument6 SeitenKnowledge, Attitudes, and Perception Towards Human Papilloma Virus Among University Students in Mumbai, IndiaDnyanesh LimayeNoch keine Bewertungen
- Cover DLDokument1 SeiteCover DLDnyanesh LimayeNoch keine Bewertungen
- Final Name Attachment FileDokument7 SeitenFinal Name Attachment FileDnyanesh LimayeNoch keine Bewertungen
- Protocol Outline TemplateDokument18 SeitenProtocol Outline TemplateDnyanesh LimayeNoch keine Bewertungen
- Anxiety, Insomnia and Excessive Daytime Sleepiness in Sleep Bruxism PatientsDokument6 SeitenAnxiety, Insomnia and Excessive Daytime Sleepiness in Sleep Bruxism PatientsDnyanesh LimayeNoch keine Bewertungen
- IJAM-1430 Invoice Oral CancerDokument1 SeiteIJAM-1430 Invoice Oral CancerDnyanesh LimayeNoch keine Bewertungen
- Ijcmph-3266 o 20062018 PDFDokument14 SeitenIjcmph-3266 o 20062018 PDFDnyanesh LimayeNoch keine Bewertungen
- Odds Ratio Vs Prevalence RatioDokument6 SeitenOdds Ratio Vs Prevalence RatioDnyanesh LimayeNoch keine Bewertungen
- 5853c4c9864675832b25ba492dhandbook of Urban StatisticsDokument7 Seiten5853c4c9864675832b25ba492dhandbook of Urban StatisticsPairri RaajshekharNoch keine Bewertungen
- High Risk Newborn2Dokument15 SeitenHigh Risk Newborn2Catherine Villanueva Sta Monica100% (1)
- The Digestive System: Chapter 23 - Lecture NotesDokument77 SeitenThe Digestive System: Chapter 23 - Lecture NotesJonalyn ChewacheoNoch keine Bewertungen
- Level+5+wordlist+12+3+12 RRDokument148 SeitenLevel+5+wordlist+12+3+12 RRELISA GALINDO GUERRANoch keine Bewertungen
- BioOutsource Virus TestingDokument2 SeitenBioOutsource Virus TestingAxiaer SolutionsNoch keine Bewertungen
- Minerva Anestesiol 2017 GruenewaldDokument15 SeitenMinerva Anestesiol 2017 GruenewaldMarjorie Lisseth Calderón LozanoNoch keine Bewertungen
- Chapter 6 - Tissues Revision NotesDokument4 SeitenChapter 6 - Tissues Revision NotesAbhishek100% (1)
- Testicular Diseases Orchitis Epididymitis Testicular Torsion Aricocele Hydrocele Anorchidism HydroceleDokument2 SeitenTesticular Diseases Orchitis Epididymitis Testicular Torsion Aricocele Hydrocele Anorchidism HydroceleDani PhilipNoch keine Bewertungen
- Epigenetics of Chimps and HumansDokument2 SeitenEpigenetics of Chimps and Humanseustoque2668Noch keine Bewertungen
- Citrasate: Product ManualDokument30 SeitenCitrasate: Product ManualfidabimeeNoch keine Bewertungen
- Biology ProjectDokument27 SeitenBiology Projectravifact0% (2)
- Jump To Navigation Jump To Search: For Other Uses, SeeDokument19 SeitenJump To Navigation Jump To Search: For Other Uses, SeeDanny FentomNoch keine Bewertungen
- Form SPK Dan RKK Dokter Umum-1Dokument4 SeitenForm SPK Dan RKK Dokter Umum-1Vivin Mai diatyNoch keine Bewertungen
- Soni Clinic & Pathology Center Chanda: Address:-Front of TVS AgencyDokument1 SeiteSoni Clinic & Pathology Center Chanda: Address:-Front of TVS AgencyVishalNoch keine Bewertungen
- 02.1 Cell Theory WorksheetDokument9 Seiten02.1 Cell Theory WorksheetJoelle PoweNoch keine Bewertungen
- PDHPE Yearly NotesDokument11 SeitenPDHPE Yearly NotesAnjaliNoch keine Bewertungen
- Scientific Signs of Qur'an & SunnahDokument26 SeitenScientific Signs of Qur'an & SunnahISLAMICULTURE100% (11)
- Food Borne Diseases and Its PreventionDokument181 SeitenFood Borne Diseases and Its Preventionapi-19916399Noch keine Bewertungen
- Co-Occurance of Potentially Preventable Factors in 246 Dog Bite-Related FatalitiesDokument11 SeitenCo-Occurance of Potentially Preventable Factors in 246 Dog Bite-Related FatalitiesRay StillNoch keine Bewertungen
- Jatharagni and Thairoid GlandDokument8 SeitenJatharagni and Thairoid Glandshenali nadeeshaNoch keine Bewertungen
- Venous Obstruction Abdominal Wall Venous Collaterals: The Latent Clinical Sign For Central ChronicDokument3 SeitenVenous Obstruction Abdominal Wall Venous Collaterals: The Latent Clinical Sign For Central ChronicSzekeres-Csiki KatalinNoch keine Bewertungen
- CPCDokument32 SeitenCPCBaihaqi ReadsNoch keine Bewertungen
- TRANS Porno MyocardialDokument3 SeitenTRANS Porno MyocardialChristy Joy AvilaNoch keine Bewertungen
- NEMATODESDokument4 SeitenNEMATODESAbby VillamuchoNoch keine Bewertungen
- Crude Fat, Hexanes Extraction, in Feed, Cereal Grain, and Forage (Randall/Soxtec/Submersion Method) : Collaborative StudyDokument10 SeitenCrude Fat, Hexanes Extraction, in Feed, Cereal Grain, and Forage (Randall/Soxtec/Submersion Method) : Collaborative StudyIshtiaque IshtiNoch keine Bewertungen
- Alpha Fetoprotein Test - 2020Dokument3 SeitenAlpha Fetoprotein Test - 2020Orl TrinidadNoch keine Bewertungen