Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Margaret Sanger's Role in Population Control AgendaDokument11 SeitenMargaret Sanger's Role in Population Control AgendaBlackShadowSnoopy100% (1)
- ICAEW Professional Level Business Planning - Taxation Question & Answer Bank March 2016 To March 2020Dokument382 SeitenICAEW Professional Level Business Planning - Taxation Question & Answer Bank March 2016 To March 2020Optimal Management SolutionNoch keine Bewertungen
- Certificate: Portfolio For Self Dircted Learning For Major Project WorkDokument22 SeitenCertificate: Portfolio For Self Dircted Learning For Major Project WorkRaja ManeNoch keine Bewertungen
- Numerical Reasoning Practice Test Answers: de Roza Education and Research 2016Dokument2 SeitenNumerical Reasoning Practice Test Answers: de Roza Education and Research 2016johnNoch keine Bewertungen
- Play and Communication TheoryDokument21 SeitenPlay and Communication Theoryroberto100% (2)
- TV Commercials Depicting MothersDokument2 SeitenTV Commercials Depicting MothersClarence TumabiaoNoch keine Bewertungen
- ATEX Guidelines for the Valve IndustryDokument49 SeitenATEX Guidelines for the Valve Industryio1_roNoch keine Bewertungen
- APA Style Guide For StudentsDokument18 SeitenAPA Style Guide For StudentsTeacher Jorge Omar NievesNoch keine Bewertungen
- ARSA 2010 International Conference Proceeding - Volume IIDokument540 SeitenARSA 2010 International Conference Proceeding - Volume IICholnapa AnukulNoch keine Bewertungen
- Composite Fish Culture PDFDokument2 SeitenComposite Fish Culture PDFHanumant JagtapNoch keine Bewertungen
- Material Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDokument6 SeitenMaterial Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationHazama HexNoch keine Bewertungen
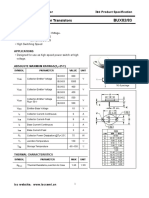
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDokument2 SeitenIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCNoch keine Bewertungen
- Child Development: Resilience & Risk, A Course SyllabusDokument17 SeitenChild Development: Resilience & Risk, A Course SyllabusJane GilgunNoch keine Bewertungen
- All India Test Series (2023-24)Dokument22 SeitenAll India Test Series (2023-24)Anil KumarNoch keine Bewertungen
- EP820 User Guide (V100R003C00 - 05) (PDF) - ENDokument47 SeitenEP820 User Guide (V100R003C00 - 05) (PDF) - ENchineaNoch keine Bewertungen
- Pride and Prejudice ScriptDokument25 SeitenPride and Prejudice ScriptLaura JaszczNoch keine Bewertungen
- PST - Module 2 - Career Stage 2 Breakout Room Discussion Summary Table (g5)Dokument3 SeitenPST - Module 2 - Career Stage 2 Breakout Room Discussion Summary Table (g5)Isidro PalomaresNoch keine Bewertungen
- CHEMIST LICENSURE EXAM TABLEDokument8 SeitenCHEMIST LICENSURE EXAM TABLEJasmin NewNoch keine Bewertungen
- SerieventilacionDokument37 SeitenSerieventilacionCaexvenNoch keine Bewertungen
- M M M V V V N N N δ δ: Client: Date: Author: Job #: Project: Subject: B1 ReferencesDokument12 SeitenM M M V V V N N N δ δ: Client: Date: Author: Job #: Project: Subject: B1 ReferencesAndrew ArahaNoch keine Bewertungen
- Bams 1st Rachna Sharir Joints and Their Classification 16-05-2020Dokument15 SeitenBams 1st Rachna Sharir Joints and Their Classification 16-05-2020Sanjana SajjanarNoch keine Bewertungen
- ASTM Liquid-in-Glass Thermometers: Standard Specification ForDokument64 SeitenASTM Liquid-in-Glass Thermometers: Standard Specification ForAnonh AdikoNoch keine Bewertungen
- Dentwiton Company Profile (En) 20221019-V2.1Dokument20 SeitenDentwiton Company Profile (En) 20221019-V2.1BRAIS FREIRÍA LORENZONoch keine Bewertungen
- Pectin-Based Bioplastics from Passion Fruit RindDokument3 SeitenPectin-Based Bioplastics from Passion Fruit RindDyna Lou Jane CatanNoch keine Bewertungen
- ParaphrasingDokument20 SeitenParaphrasingPlocios JannNoch keine Bewertungen
- Life Skills Unit PlanDokument15 SeitenLife Skills Unit PlanLindy McBratneyNoch keine Bewertungen
- TuflineLinedBallValve 332148 2-07Dokument12 SeitenTuflineLinedBallValve 332148 2-07Marcio NegraoNoch keine Bewertungen
- Ig2 of Bikas 00691520 x123Dokument20 SeitenIg2 of Bikas 00691520 x123Engr. Imran Hasan Pathan100% (4)
- Narcos 1x01 - DescensoDokument53 SeitenNarcos 1x01 - DescensoBirdy NumnumsNoch keine Bewertungen
- sm2000 GBDokument4 Seitensm2000 GBRikky ChaniagoNoch keine Bewertungen