Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Leave Form CS Form No Version 1Dokument2 SeitenLeave Form CS Form No Version 1Michael ValdezNoch keine Bewertungen
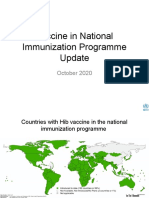
- Vaccine in National Immunization Programme Update: October 2020Dokument12 SeitenVaccine in National Immunization Programme Update: October 2020Michael ValdezNoch keine Bewertungen
- Quarter - : (Month) (Month) (Month) (Month) (Month) (Month)Dokument8 SeitenQuarter - : (Month) (Month) (Month) (Month) (Month) (Month)Michael ValdezNoch keine Bewertungen
- Central Luzon Doctors' Hospital Educational Institution, IncDokument2 SeitenCentral Luzon Doctors' Hospital Educational Institution, IncMichael ValdezNoch keine Bewertungen
- Organizational Politics and PowerDokument23 SeitenOrganizational Politics and PowerMichael Valdez100% (1)
- Ethical PrinciplesDokument7 SeitenEthical PrinciplesMichael ValdezNoch keine Bewertungen
- BIOETHICS Professional Issues HandoutsDokument2 SeitenBIOETHICS Professional Issues HandoutsMichael ValdezNoch keine Bewertungen
- CataractsDokument5 SeitenCataractsMichael ValdezNoch keine Bewertungen
- PulseoximetryDokument2 SeitenPulseoximetryRakshith NagarajaiahNoch keine Bewertungen
- Futuristic Nursing: - Sister Elizabeth DavisDokument14 SeitenFuturistic Nursing: - Sister Elizabeth DavisPhebeDimple100% (2)
- Diet's CardDokument8 SeitenDiet's CardJORGE ATRIANONoch keine Bewertungen
- Herbicides ToxicityDokument51 SeitenHerbicides ToxicityAdarshBijapurNoch keine Bewertungen
- 2014-1 Mag LoresDokument52 Seiten2014-1 Mag LoresLi SacNoch keine Bewertungen
- Coca Cola Fairlife CaseDokument4 SeitenCoca Cola Fairlife Caseapi-315994561Noch keine Bewertungen
- AM LOVE School Form 8 SF8 Learner Basic Health and Nutrition ReportDokument4 SeitenAM LOVE School Form 8 SF8 Learner Basic Health and Nutrition ReportLornaNirzaEnriquezNoch keine Bewertungen
- 2018 Overview Digestive System HandoutDokument11 Seiten2018 Overview Digestive System HandoutdraganNoch keine Bewertungen
- Eular References For Website 2015Dokument240 SeitenEular References For Website 2015Antonio BernalNoch keine Bewertungen
- Kardiomed-700-User ManualDokument87 SeitenKardiomed-700-User ManualJulia TimakovaNoch keine Bewertungen
- WEEK 2 ILP Grade 4Dokument5 SeitenWEEK 2 ILP Grade 4jean arriolaNoch keine Bewertungen
- Social Science Class 10 Understanding Economic DevelopmentDokument93 SeitenSocial Science Class 10 Understanding Economic DevelopmentkannansesNoch keine Bewertungen
- 23 Medicinal Plants The Native Americans Used On A Daily Basis - MSYCDokument15 Seiten23 Medicinal Plants The Native Americans Used On A Daily Basis - MSYCLeandro RodriguesNoch keine Bewertungen
- Checking Vital SighnDokument14 SeitenChecking Vital SighnAdimas AnggaraNoch keine Bewertungen
- Pork TocinoDokument1 SeitePork TocinoMaria Ivz ElborNoch keine Bewertungen
- JPNC 02 00096Dokument9 SeitenJPNC 02 00096Catalina StoicescuNoch keine Bewertungen
- Module 7. Presented - The Phil Health Program On Degenerative Diseases 93Dokument105 SeitenModule 7. Presented - The Phil Health Program On Degenerative Diseases 93Roma ClaireNoch keine Bewertungen
- Et CareDokument15 SeitenEt CarePaulo GarciaNoch keine Bewertungen
- Osteoarthritis of The Hip and Knee Flowchart PDFDokument2 SeitenOsteoarthritis of The Hip and Knee Flowchart PDFsilkofosNoch keine Bewertungen
- Esmeron 10 MG/ML Solution For Injection Rocuronium Bromide Prescribing InformationDokument3 SeitenEsmeron 10 MG/ML Solution For Injection Rocuronium Bromide Prescribing InformationVeeta Ruchi LieNoch keine Bewertungen
- BNMHGDokument34 SeitenBNMHGAnonymous lt2LFZHNoch keine Bewertungen
- Anemia in PregnancyDokument5 SeitenAnemia in PregnancySandra GabasNoch keine Bewertungen
- Know About Dengue FeverDokument11 SeitenKnow About Dengue FeverKamlesh SanghaviNoch keine Bewertungen
- Dokumen - Tips Biology Investigatory Project 561e79b91f5a0Dokument17 SeitenDokumen - Tips Biology Investigatory Project 561e79b91f5a0Upendra LalNoch keine Bewertungen
- Action Plan GPPDokument3 SeitenAction Plan GPPMa Rk AntonioNoch keine Bewertungen
- Secondary P.E. 10 Q3Dokument9 SeitenSecondary P.E. 10 Q3Jayzi VicenteNoch keine Bewertungen
- Platelet Analysis - An Overview: HistoryDokument7 SeitenPlatelet Analysis - An Overview: HistoryPieter Du Toit-EnslinNoch keine Bewertungen
- Cultural Landscape An Introduction To Human Geography 11th Edition Rubenstein Solutions ManualDokument16 SeitenCultural Landscape An Introduction To Human Geography 11th Edition Rubenstein Solutions Manualheathergarciafbqedgosyp100% (13)
- Climbing Training Log - TemplateDokument19 SeitenClimbing Training Log - TemplateKam Iqar ZeNoch keine Bewertungen
- Feeding Norms Poultry76Dokument14 SeitenFeeding Norms Poultry76Ramesh BeniwalNoch keine Bewertungen