Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Warsaw Pact: Warsaw Treaty Organization of Friendship, Cooperation, and Mutual AssistanceDokument8 SeitenWarsaw Pact: Warsaw Treaty Organization of Friendship, Cooperation, and Mutual Assistancejbahalkeh7570Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Dokument22 Seiten400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkeh7570Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Opportunism and The Collapse of The Second International: V. I. LeninDokument5 SeitenOpportunism and The Collapse of The Second International: V. I. Leninjbahalkeh7570Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Zakaria Dont Rush To War With IranDokument1 SeiteZakaria Dont Rush To War With Iranjbahalkeh7570Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Berlin - THE PURPOSE OF PHILOSOPHYDokument8 SeitenBerlin - THE PURPOSE OF PHILOSOPHYjbahalkeh7570Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Henry II of FranceDokument42 SeitenHenry II of Francejbahalkeh7570Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Dokument118 Seiten400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkeh7570Noch keine Bewertungen
- Miller 7th Ed Chapter I HistoryDokument35 SeitenMiller 7th Ed Chapter I Historyjbahalkeh7570Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- HX of Surgery Owen WangensteenDokument5 SeitenHX of Surgery Owen Wangensteenjbahalkeh7570Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- APPI Endorses Helsinki UpdatesDokument2 SeitenAPPI Endorses Helsinki Updatesjbahalkeh7570Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Evidence-Based Screening Criteria For Retinopathy of PrematurityDokument7 SeitenEvidence-Based Screening Criteria For Retinopathy of Prematurityjbahalkeh7570Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Evidence Based Practice in Primary Care (ILLUSTRATED)Dokument217 SeitenEvidence Based Practice in Primary Care (ILLUSTRATED)lmjeksoreNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Checklist For Appraising An Article On TreatmentDokument4 SeitenChecklist For Appraising An Article On Treatmentjbahalkeh7570Noch keine Bewertungen
- Shri Fa 4Dokument44 SeitenShri Fa 4Veena H NayakNoch keine Bewertungen
- Telmisartan, ISMNDokument8 SeitenTelmisartan, ISMNDenise EspinosaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- E2870-13 Standard Test Method For Evaluating RelativDokument6 SeitenE2870-13 Standard Test Method For Evaluating RelativA MusaverNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Bioclim MaxentDokument9 SeitenBioclim MaxentNicolás FrutosNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Flares & VentsDokument29 SeitenFlares & VentsSonu Kaka KakaNoch keine Bewertungen
- Rolling Fig Q A AnalysisDokument11 SeitenRolling Fig Q A AnalysisRavinder Antil100% (9)
- Fujifilm X-E4 SpecificationsDokument5 SeitenFujifilm X-E4 SpecificationsNikonRumorsNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Pakistan PresentationDokument17 SeitenPakistan PresentationYaseen Khan100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Brochure E-AIR T400-900 WEG APP 2958 1020 02 ENDokument3 SeitenBrochure E-AIR T400-900 WEG APP 2958 1020 02 ENDaniel BravoNoch keine Bewertungen
- Improving Performance, Proxies, and The Render CacheDokument13 SeitenImproving Performance, Proxies, and The Render CacheIOXIRNoch keine Bewertungen
- Kitchen Colour Ide1Dokument6 SeitenKitchen Colour Ide1Kartik KatariaNoch keine Bewertungen
- Clinical Science of Guilen Barren SyndromeDokument2 SeitenClinical Science of Guilen Barren SyndromemanakimanakuNoch keine Bewertungen
- Examination Speaking Assignments Term III - 2021Dokument2 SeitenExamination Speaking Assignments Term III - 2021Khrystyna ShkilniukNoch keine Bewertungen
- IBRO News 2004Dokument8 SeitenIBRO News 2004International Brain Research Organization100% (1)
- Action Plan Gulayan Sa PaaralanDokument2 SeitenAction Plan Gulayan Sa PaaralanAntonio ArienzaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Std9thMathsBridgeCourse (4) (001-040) .MR - enDokument40 SeitenStd9thMathsBridgeCourse (4) (001-040) .MR - ensilent gamerNoch keine Bewertungen
- Prepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentDokument11 SeitenPrepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentwaqasNoch keine Bewertungen
- Sales Training Deck Updated July 2022Dokument40 SeitenSales Training Deck Updated July 2022Thanh MinhNoch keine Bewertungen
- Drypix 6000 12eDokument501 SeitenDrypix 6000 12eraj_meditech100% (1)
- Zeolites and Ordered Porous Solids - Fundamentals and ApplicationsDokument376 SeitenZeolites and Ordered Porous Solids - Fundamentals and ApplicationsHenrique Souza100% (1)
- BS en 6100-3-2 Electromagnetic Compatibility (EMC)Dokument12 SeitenBS en 6100-3-2 Electromagnetic Compatibility (EMC)Arun Jacob CherianNoch keine Bewertungen
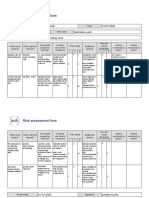
- Risk Assessment Project Iosh - MsDokument2 SeitenRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Line CodingDokument27 SeitenLine CodingshridonNoch keine Bewertungen
- Hipertensiunea Arteriala - Cauze Si TratamenteDokument25 SeitenHipertensiunea Arteriala - Cauze Si TratamenteClaudia MurguNoch keine Bewertungen
- Relay Identification: Example CDG31FF002SACHDokument5 SeitenRelay Identification: Example CDG31FF002SACHRohit RanaNoch keine Bewertungen
- IoT & WSN - Module 5 - 2018 by Prof - SVDokument43 SeitenIoT & WSN - Module 5 - 2018 by Prof - SVVignesh MJ83% (6)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jurnal Semi FowlerDokument6 SeitenJurnal Semi FowlerHartina RolobessyNoch keine Bewertungen
- Portable Load Banks: CressallDokument1 SeitePortable Load Banks: CressallYashveer26Noch keine Bewertungen
- Elevator ControlDokument3 SeitenElevator ControlNATHANNoch keine Bewertungen
- RT Offer L-Seam-14.01.2023Dokument1 SeiteRT Offer L-Seam-14.01.2023Eswar Enterprises QcNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)