Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- GX Annular Blowout PreventerDokument2 SeitenGX Annular Blowout PreventerCarlos Munizaga100% (1)
- Physical Fitness: Group 3 Members: Ali, Mycah Therese Hibuton, Jessa Sanguila, Aminah Canque, Nicole Ombawa, OmayyahDokument13 SeitenPhysical Fitness: Group 3 Members: Ali, Mycah Therese Hibuton, Jessa Sanguila, Aminah Canque, Nicole Ombawa, OmayyahjessaNoch keine Bewertungen
- The BBTT Program REV PDFDokument40 SeitenThe BBTT Program REV PDFBianca Lacramioara Florea100% (3)
- Encyclopaedia of Chess OpeningsDokument4 SeitenEncyclopaedia of Chess OpeningsAdi Susanto56% (9)
- Champions League: UEFA Champions League Anthem (With SATB. Choir Parts)Dokument3 SeitenChampions League: UEFA Champions League Anthem (With SATB. Choir Parts)charles camilo67% (3)
- RMAX Instruction ManualDokument40 SeitenRMAX Instruction ManualGuille Gimeno100% (1)
- Velocity, Distance & Acceleration 1 QPDokument11 SeitenVelocity, Distance & Acceleration 1 QPsarkodie kwameNoch keine Bewertungen
- Pendraken Catalogue Jan 2021Dokument61 SeitenPendraken Catalogue Jan 2021GrumpyOldManNoch keine Bewertungen
- King of Ears Torture DemonDokument1 SeiteKing of Ears Torture DemonMatt AmorosoNoch keine Bewertungen
- Hitachi C12LC Compound Saw Parts ListDokument10 SeitenHitachi C12LC Compound Saw Parts Listwindsurferke007Noch keine Bewertungen
- Botvinnik-Bronstein WCC Match (Moscow 1951)Dokument10 SeitenBotvinnik-Bronstein WCC Match (Moscow 1951)navaro kastigiasNoch keine Bewertungen
- Hand Goniometry 1565417609716Dokument19 SeitenHand Goniometry 1565417609716AVIMANNU SINGHNoch keine Bewertungen
- Gameweek 2 28 September 2021 PSG Manchester CityDokument24 SeitenGameweek 2 28 September 2021 PSG Manchester CityBen SaadNoch keine Bewertungen
- K91.11 Soft Seated Ball Valve, Fully Welded or Threaded BodyDokument4 SeitenK91.11 Soft Seated Ball Valve, Fully Welded or Threaded BodyadrianioantomaNoch keine Bewertungen
- Manual of Arms With m1Dokument7 SeitenManual of Arms With m1hgbpaNoch keine Bewertungen
- One Horse Town ChordsDokument2 SeitenOne Horse Town ChordselbersenNoch keine Bewertungen
- Loves Theme. Barry White-Corno en FaDokument1 SeiteLoves Theme. Barry White-Corno en FaJorge Antonio Barajas GuerreroNoch keine Bewertungen
- New Millenium FibresDokument34 SeitenNew Millenium FibresMonit Sharma VashisthNoch keine Bewertungen
- Fan-Made Climactic End Game Phase for EverrainDokument5 SeitenFan-Made Climactic End Game Phase for Everrainrichard leonardoNoch keine Bewertungen
- Scouts Camp Activity 2023Dokument4 SeitenScouts Camp Activity 2023Mhel PerezNoch keine Bewertungen
- USNEWS Ranking 2022Dokument16 SeitenUSNEWS Ranking 2022Amaka AbatuluNoch keine Bewertungen
- L&T Panel Accessories Price List 01JUL2017Dokument44 SeitenL&T Panel Accessories Price List 01JUL2017TarunPatraNoch keine Bewertungen
- Common Patterns of Cortisol Imbalance: Patient HandoutDokument2 SeitenCommon Patterns of Cortisol Imbalance: Patient HandoutCorey EasleyNoch keine Bewertungen
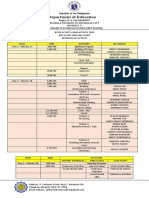
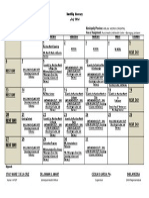
- Monthly ItineraryDokument1 SeiteMonthly ItineraryErwindelaCruzNoch keine Bewertungen
- Case StudyDokument4 SeitenCase StudyBabilash KBNoch keine Bewertungen
- Massey Ferguson 6495 TRACTOR Service Parts Catalogue Manual (Part Number 1637444)Dokument19 SeitenMassey Ferguson 6495 TRACTOR Service Parts Catalogue Manual (Part Number 1637444)bvk2980022Noch keine Bewertungen
- Real estate data appendix with mortgage detailsDokument11 SeitenReal estate data appendix with mortgage detailsPutri Indah PermatasariNoch keine Bewertungen
- Epic Games Inc V Apple Inc Candce-20-05640 0812.0-2Dokument185 SeitenEpic Games Inc V Apple Inc Candce-20-05640 0812.0-2Chance MillerNoch keine Bewertungen
- 2020-11-24 Business Violations SpreadsheetDokument7 Seiten2020-11-24 Business Violations SpreadsheetNewsChannel 9100% (1)
- NP + TV (E12) (Key Lien)Dokument41 SeitenNP + TV (E12) (Key Lien)Linh HoàngNoch keine Bewertungen