Das könnte Ihnen auch gefallen
- Vijay Law Series List of Publications - 2014: SN Subject/Title Publisher Year IsbnDokument3 SeitenVijay Law Series List of Publications - 2014: SN Subject/Title Publisher Year IsbnSabya Sachee Rai0% (2)
- Avatar Legends The Roleplaying Game 1 12Dokument12 SeitenAvatar Legends The Roleplaying Game 1 12azeaze0% (1)
- Seventh Day Adventist Quiz by KnowingTheTimeDokument4 SeitenSeventh Day Adventist Quiz by KnowingTheTimeMiiiTheart100% (3)
- Zoe LeonardDokument9 SeitenZoe LeonardSandro Alves SilveiraNoch keine Bewertungen
- Mark Scheme (Results) Summer 2019: Pearson Edexcel International GCSE in English Language (4EB1) Paper 01RDokument19 SeitenMark Scheme (Results) Summer 2019: Pearson Edexcel International GCSE in English Language (4EB1) Paper 01RNairit100% (1)
- Fin Trauma Podcast Ver2Dokument3 SeitenFin Trauma Podcast Ver2fulanotaNoch keine Bewertungen
- Tirado-Bsn 4D - JR Summary and ReflectionDokument3 SeitenTirado-Bsn 4D - JR Summary and ReflectionJeniper Marie Cute29Noch keine Bewertungen
- Damage Control ResuscitationDokument15 SeitenDamage Control ResuscitationLizzy BennetNoch keine Bewertungen
- Damage Control SurgeryDokument68 SeitenDamage Control SurgeryMAMA LALANoch keine Bewertungen
- Initial Assessment and ResuscitationDokument9 SeitenInitial Assessment and ResuscitationSri MahadhanaNoch keine Bewertungen
- Embolization Hepatic TraumaDokument10 SeitenEmbolization Hepatic TraumaФедір ПавукNoch keine Bewertungen
- Mechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxDokument7 SeitenMechanical Ventilator Discontinuation Process: Lingye Chen,, Daniel Gilstrap,, Christopher E. CoxGhost11mNoch keine Bewertungen
- Terapi CairanDokument5 SeitenTerapi CairanZikry SitaniaNoch keine Bewertungen
- Ying Li 2016Dokument8 SeitenYing Li 2016Bogdan TrandafirNoch keine Bewertungen
- AnastesiDokument22 SeitenAnastesidhitadwynNoch keine Bewertungen
- Damage Control Surgery and ICU (Feb-14-08)Dokument10 SeitenDamage Control Surgery and ICU (Feb-14-08)Agung Sari WijayantiNoch keine Bewertungen
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDokument6 SeitenTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142Noch keine Bewertungen
- Guidelines For Perioperative Care in Cardiac SurgeryDokument5 SeitenGuidelines For Perioperative Care in Cardiac SurgeryTomi EscribanoNoch keine Bewertungen
- Avoiding Revascularization With Lifestyle Changes: The Multicenter Lifestyle Demonstration ProjectDokument5 SeitenAvoiding Revascularization With Lifestyle Changes: The Multicenter Lifestyle Demonstration ProjectNag Mallesh RaoNoch keine Bewertungen
- Safety PPMDokument11 SeitenSafety PPMMonica TrifitrianaNoch keine Bewertungen
- Abdominal TraumaDokument34 SeitenAbdominal TraumaStephany RodriguezNoch keine Bewertungen
- Abdominal TraumaDokument34 SeitenAbdominal Traumalaurz95Noch keine Bewertungen
- Anesthesia Considerations During Cytoreductive SurDokument9 SeitenAnesthesia Considerations During Cytoreductive Surdrardigustian2986Noch keine Bewertungen
- Physiotherapy in The ICUDokument10 SeitenPhysiotherapy in The ICUakheel ahammedNoch keine Bewertungen
- SOSD Phases of Fluid ResuscitationDokument8 SeitenSOSD Phases of Fluid ResuscitationAvinash KumbharNoch keine Bewertungen
- ACG Ulcer Bleeding Guideline SummaryDokument6 SeitenACG Ulcer Bleeding Guideline SummaryElison J PanggaloNoch keine Bewertungen
- Splenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st CenturyDokument4 SeitenSplenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st Centurykevin stefanoNoch keine Bewertungen
- Perioperative Period of Reconstructive and Burn Surgery in Intensive Care MedicineDokument9 SeitenPerioperative Period of Reconstructive and Burn Surgery in Intensive Care MedicineRiza Angela BarazanNoch keine Bewertungen
- Shock Hipo 2 FixDokument11 SeitenShock Hipo 2 FixAdeliaNoch keine Bewertungen
- Trauma Assessment Initial Trauma AssessmentDokument6 SeitenTrauma Assessment Initial Trauma Assessmentrika100% (1)
- Blunt Abdominal Injuries: Adam J Brooks and Brian J RowlandsDokument12 SeitenBlunt Abdominal Injuries: Adam J Brooks and Brian J RowlandsRajan KarmakarNoch keine Bewertungen
- BST - General ConsiderationsDokument9 SeitenBST - General ConsiderationsDita Mutiara IrawanNoch keine Bewertungen
- JofIMAB2013vol19b2p282 285 PDFDokument4 SeitenJofIMAB2013vol19b2p282 285 PDFAlung Padang SiraitNoch keine Bewertungen
- Traum ManagementDokument7 SeitenTraum Managementchinthaka18389021Noch keine Bewertungen
- Intensive Care Unit Management of The Trauma PatientDokument8 SeitenIntensive Care Unit Management of The Trauma Patientantonio dengNoch keine Bewertungen
- Abdominal TraumaDokument30 SeitenAbdominal TraumaOscar HernandezNoch keine Bewertungen
- Impact of Postoperative Morbidity On Long-Term Survival After OesophagectomyDokument10 SeitenImpact of Postoperative Morbidity On Long-Term Survival After OesophagectomyPutri PadmosuwarnoNoch keine Bewertungen
- Prehospital Stroke Care: New Prospects For Treatment and Clinical ResearchDokument8 SeitenPrehospital Stroke Care: New Prospects For Treatment and Clinical ResearchmiriamneuroNoch keine Bewertungen
- Strategies For Improving Visualization During Endoscopic Skull Base SurgeryDokument10 SeitenStrategies For Improving Visualization During Endoscopic Skull Base SurgeryTi FaNoch keine Bewertungen
- Pre and Post Operative Care: To: DR - Biniyam. By: Biniam.MDokument56 SeitenPre and Post Operative Care: To: DR - Biniyam. By: Biniam.MBini JaminNoch keine Bewertungen
- Richards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023Dokument13 SeitenRichards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023jorge fabregatNoch keine Bewertungen
- Bmri2016 3741426Dokument7 SeitenBmri2016 3741426MandaNoch keine Bewertungen
- Tatalaksana Hyponatremia Pada Diuresis Post ObstruktifDokument4 SeitenTatalaksana Hyponatremia Pada Diuresis Post ObstruktifGilberto ChafrinaNoch keine Bewertungen
- A Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Dokument25 SeitenA Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Navjot Brar71% (14)
- Santoso2005Dokument11 SeitenSantoso2005ayubahriNoch keine Bewertungen
- Politrauma - Rolul AtiDokument18 SeitenPolitrauma - Rolul AtiChirita ElenaNoch keine Bewertungen
- Blood Transfusion 2Dokument7 SeitenBlood Transfusion 2omarragabselimNoch keine Bewertungen
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDokument38 Seiten2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- DCV PDFDokument25 SeitenDCV PDFLeyDi CamposanoNoch keine Bewertungen
- Surgical Decompression: Chronic Subdural HematomaDokument3 SeitenSurgical Decompression: Chronic Subdural Hematomaeirene simbolonNoch keine Bewertungen
- %pediatric TracheostomyDokument25 Seiten%pediatric TracheostomyFabian Camelo OtorrinoNoch keine Bewertungen
- 1,4 Dan 5Dokument3 Seiten1,4 Dan 5Gilberto ChafrinaNoch keine Bewertungen
- Perioperative Care For CABG PatientsDokument32 SeitenPerioperative Care For CABG PatientsAya EyadNoch keine Bewertungen
- 296 Neck of Femur Fracture Peri-Operative ManagementDokument8 Seiten296 Neck of Femur Fracture Peri-Operative ManagementNilam dwinilamsariNoch keine Bewertungen
- Myasthenia Gravis Multiple Sclerosis Case FileDokument3 SeitenMyasthenia Gravis Multiple Sclerosis Case Filehttps://medical-phd.blogspot.comNoch keine Bewertungen
- Septic Shock TreatmentDokument22 SeitenSeptic Shock TreatmentAdreiTheTripleA100% (1)
- Anzcor Guideline 11 10 1 Als Traumatic Arrest 27apr16Dokument11 SeitenAnzcor Guideline 11 10 1 Als Traumatic Arrest 27apr16Mario Colville SolarNoch keine Bewertungen
- Pre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MDokument55 SeitenPre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MBini JaminNoch keine Bewertungen
- PIIS0007091221004359Dokument7 SeitenPIIS0007091221004359luisfernandoamaya89Noch keine Bewertungen
- Anesthessia During OesophagectomyDokument8 SeitenAnesthessia During OesophagectomyAngy KarakostaNoch keine Bewertungen
- Damage Control Resuscitation: The New Face of Damage ControlDokument15 SeitenDamage Control Resuscitation: The New Face of Damage ControlAndreia MattiuciNoch keine Bewertungen
- Matthew T Harting Surgical Management of CongenitalDokument14 SeitenMatthew T Harting Surgical Management of CongenitalLuis Enrique Sánchez-SierraNoch keine Bewertungen
- Observed and Medinine Care For Patients Operated On in The Abdominal CavityDokument11 SeitenObserved and Medinine Care For Patients Operated On in The Abdominal CavityAlex HirschNoch keine Bewertungen
- Essentials in Lung TransplantationVon EverandEssentials in Lung TransplantationAllan R. GlanvilleNoch keine Bewertungen
- Medico-Legal Issues in AnaesthesiaDokument2 SeitenMedico-Legal Issues in AnaesthesiaSuresh KumarNoch keine Bewertungen
- Controversial Issues in NeuroanaesthesiaDokument12 SeitenControversial Issues in NeuroanaesthesiaSuresh KumarNoch keine Bewertungen
- Ventilator Associated Pneumonia (Vap)Dokument11 SeitenVentilator Associated Pneumonia (Vap)Suresh KumarNoch keine Bewertungen
- Local Anaesthetic AgentsDokument21 SeitenLocal Anaesthetic AgentsSuresh KumarNoch keine Bewertungen
- Day Care AnesthesiaDokument4 SeitenDay Care AnesthesiaSuresh KumarNoch keine Bewertungen
- Alleviating Cancer PainDokument9 SeitenAlleviating Cancer PainSuresh KumarNoch keine Bewertungen
- Labour Analgesia - Recent ConceptsDokument18 SeitenLabour Analgesia - Recent ConceptsSuresh KumarNoch keine Bewertungen
- Anaesthesia in The Gastrointestinal Endoscopy SuiteDokument3 SeitenAnaesthesia in The Gastrointestinal Endoscopy SuiteSuresh KumarNoch keine Bewertungen
- Anaesthesia For Bleeding TonsilDokument6 SeitenAnaesthesia For Bleeding TonsilSave MedicalEducation Save HealthCareNoch keine Bewertungen
- Anaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Dokument16 SeitenAnaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Suresh KumarNoch keine Bewertungen
- Anaesthesia Breathing SystemsDokument15 SeitenAnaesthesia Breathing SystemsSuresh KumarNoch keine Bewertungen
- Neuromuscular PhysiologyDokument6 SeitenNeuromuscular PhysiologySuresh KumarNoch keine Bewertungen
- Anaesthetic Management of Ihd Patients For Non Cardiac SurgeryDokument18 SeitenAnaesthetic Management of Ihd Patients For Non Cardiac SurgerySuresh KumarNoch keine Bewertungen
- Uptake and Distribution of Inhalational AnestheticsDokument12 SeitenUptake and Distribution of Inhalational AnestheticsSuresh KumarNoch keine Bewertungen
- Low Flow AnaesthesiaDokument16 SeitenLow Flow AnaesthesiaSuresh Kumar100% (1)
- Pulmonary Function Test in Pre Anaesthetic EvaluationDokument10 SeitenPulmonary Function Test in Pre Anaesthetic EvaluationSuresh KumarNoch keine Bewertungen
- Liver Function Tests and Their InterpretationDokument9 SeitenLiver Function Tests and Their InterpretationSuresh KumarNoch keine Bewertungen
- 11 Chemistry NcertSolutions Chapter 2 ExercisesDokument54 Seiten11 Chemistry NcertSolutions Chapter 2 ExercisesGeeteshGuptaNoch keine Bewertungen
- Pugh MatrixDokument18 SeitenPugh MatrixSulaiman Khan0% (1)
- A Neural Network Based System For Intrusion Detection and Classification of AttacksDokument6 SeitenA Neural Network Based System For Intrusion Detection and Classification of AttacksbharadwajrohanNoch keine Bewertungen
- Magtajas vs. PryceDokument3 SeitenMagtajas vs. PryceRoyce PedemonteNoch keine Bewertungen
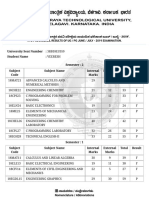
- VTU Result PDFDokument2 SeitenVTU Result PDFVaibhavNoch keine Bewertungen
- Adult Consensual SpankingDokument21 SeitenAdult Consensual Spankingswl156% (9)
- Apr 00Dokument32 SeitenApr 00nanda2006bNoch keine Bewertungen
- CH 13 ArqDokument6 SeitenCH 13 Arqneha.senthilaNoch keine Bewertungen
- Functions of Communication Oral Communication PDFDokument12 SeitenFunctions of Communication Oral Communication PDFKrystle Francess Barrios0% (1)
- Journal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengDokument10 SeitenJournal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengAnass CHERRAFINoch keine Bewertungen
- Reading8 PilkingtonDokument8 SeitenReading8 Pilkingtonab_amyNoch keine Bewertungen
- Nurse Implemented Goal Directed Strategy To.97972Dokument7 SeitenNurse Implemented Goal Directed Strategy To.97972haslinaNoch keine Bewertungen
- Philippine Psychometricians Licensure Exam RevieweDokument1 SeitePhilippine Psychometricians Licensure Exam RevieweKristelle Mae C. Azucenas0% (1)
- Why The Sea Is SaltDokument3 SeitenWhy The Sea Is SaltVictor CiobanNoch keine Bewertungen
- Story of Their Lives: Lived Experiences of Parents of Children With Special Needs Amidst The PandemicDokument15 SeitenStory of Their Lives: Lived Experiences of Parents of Children With Special Needs Amidst The PandemicPsychology and Education: A Multidisciplinary JournalNoch keine Bewertungen
- Hinog vs. MellicorDokument11 SeitenHinog vs. MellicorGreta VilarNoch keine Bewertungen
- Young Learners Starters Sample Papers 2018 Vol1Dokument15 SeitenYoung Learners Starters Sample Papers 2018 Vol1Natalia García GarcíaNoch keine Bewertungen
- Student Handbook MCCDokument32 SeitenStudent Handbook MCCeyusuf74Noch keine Bewertungen
- Productflyer - 978 1 4020 5716 8Dokument1 SeiteProductflyer - 978 1 4020 5716 8jmendozaqNoch keine Bewertungen
- Hoaxes Involving Military IncidentsDokument5 SeitenHoaxes Involving Military IncidentsjtcarlNoch keine Bewertungen
- My Pitch p2Dokument16 SeitenMy Pitch p2api-477556951Noch keine Bewertungen
- CH 2 & CH 3 John R. Schermerhorn - Management-Wiley (2020)Dokument9 SeitenCH 2 & CH 3 John R. Schermerhorn - Management-Wiley (2020)Muhammad Fariz IbrahimNoch keine Bewertungen
- Makalsh CMDDokument22 SeitenMakalsh CMDMaudy Rahmi HasniawatiNoch keine Bewertungen
- BRP 40k Second Edition 2col PDFDokument54 SeitenBRP 40k Second Edition 2col PDFColin BrettNoch keine Bewertungen
- School of ApologeticsDokument104 SeitenSchool of ApologeticsSAMSONNoch keine Bewertungen