Das könnte Ihnen auch gefallen
- Complications During Labor and DeliveryDokument27 SeitenComplications During Labor and DeliveryMA. JYRELL BONITONoch keine Bewertungen
- USMLE Step 2 CK 6 Months Study Plan For 240Dokument1 SeiteUSMLE Step 2 CK 6 Months Study Plan For 240DhritisdiaryNoch keine Bewertungen
- Helminth ChartsDokument4 SeitenHelminth ChartsDrbee10Noch keine Bewertungen
- Amboss Hemolytic AnemiaDokument16 SeitenAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Gyne ReflectionDokument18 SeitenGyne ReflectionKC Dela RosaNoch keine Bewertungen
- Risk Factors - Step 2 PDFDokument5 SeitenRisk Factors - Step 2 PDFAmberNoch keine Bewertungen
- Aquifer Case - Summary - FamilyMedicine21 - 12-YDokument10 SeitenAquifer Case - Summary - FamilyMedicine21 - 12-YHyunsoo EllisNoch keine Bewertungen
- Medicowesome - AnatomyDokument19 SeitenMedicowesome - AnatomySubhashNoch keine Bewertungen
- Chapter 1 Compatible ModeDokument93 SeitenChapter 1 Compatible ModeJyha KhariNoch keine Bewertungen
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDokument3 SeitenHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Medstar ObGyn 2nd EditionDokument570 SeitenMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- Cervix Cancer Power Point With SlidesDokument41 SeitenCervix Cancer Power Point With SlidesAmín JiménezNoch keine Bewertungen
- FHSIS Form TCL Pre NatalDokument11 SeitenFHSIS Form TCL Pre NatalEden Vblagasy100% (5)
- Vasa PraeviaDokument3 SeitenVasa PraeviaAngelica CabututanNoch keine Bewertungen
- EndometriosisDokument1 SeiteEndometriosisZiyad100% (1)
- Anomalies of the placenta and cord: risks and diagnosisDokument52 SeitenAnomalies of the placenta and cord: risks and diagnosisDaniel Andre S. Somoray100% (1)
- Ninja On Fleek - Fern Charts MT2 SLAY Most UpdatedDokument56 SeitenNinja On Fleek - Fern Charts MT2 SLAY Most UpdatedyenniNoch keine Bewertungen
- Genetic LecturesDokument35 SeitenGenetic Lecturesميمونه عبدالرحيم مصطفىNoch keine Bewertungen
- Bilateral Peritonsillar Abscess Case ReportDokument2 SeitenBilateral Peritonsillar Abscess Case ReportshashaNoch keine Bewertungen
- Obstetics Simplified El-MowafiDokument515 SeitenObstetics Simplified El-Mowafiapi-370504650% (2)
- A Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Sudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015Dokument23 SeitenSudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015DrChauhanNoch keine Bewertungen
- Urinary IncontinenceDokument1 SeiteUrinary IncontinenceZiyad100% (1)
- Urinary IncontinenceDokument1 SeiteUrinary IncontinenceZiyad100% (1)
- Antepartum HemorrhageDokument3 SeitenAntepartum Hemorrhagenur1146Noch keine Bewertungen
- Differential Diagnosis of The Adnexal Mass 2020Dokument38 SeitenDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNoch keine Bewertungen
- Chapter 20 - Conditions Occurring During PregnancyDokument5 SeitenChapter 20 - Conditions Occurring During PregnancyEunice CortésNoch keine Bewertungen
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDokument117 SeitenDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylNoch keine Bewertungen
- Treatment Algorithm for Severe Morning SicknessDokument2 SeitenTreatment Algorithm for Severe Morning Sicknessrayyanzubaidi100% (1)
- BIOL 215 - CWRU Final Exam Learning GoalsDokument32 SeitenBIOL 215 - CWRU Final Exam Learning GoalsKesharaSSNoch keine Bewertungen
- Divine Intervention Episode 12 Bacteria Cases ADokument18 SeitenDivine Intervention Episode 12 Bacteria Cases ASwisskelly1Noch keine Bewertungen
- Shoulder dystocia management and PPH treatmentDokument9 SeitenShoulder dystocia management and PPH treatmentJeffrey HingNoch keine Bewertungen
- Fluid & Electrolite Management in Surgical WardsDokument97 SeitenFluid & Electrolite Management in Surgical WardsBishwanath PrasadNoch keine Bewertungen
- USMLE Step 1 Review in BiochemistryDokument18 SeitenUSMLE Step 1 Review in BiochemistryDevindra 2k17Noch keine Bewertungen
- Councelling and History TakingDokument5 SeitenCouncelling and History TakingbashingarNoch keine Bewertungen
- Student Objectives - ACOGDokument164 SeitenStudent Objectives - ACOGmango91286100% (1)
- Clinical Key Master - Content - List - 14 Jun 2019Dokument49 SeitenClinical Key Master - Content - List - 14 Jun 2019Axevim GNoch keine Bewertungen
- Biliary DisoderDokument50 SeitenBiliary DisoderZanida ZainonNoch keine Bewertungen
- HistCellBioUSMLEDokument25 SeitenHistCellBioUSMLERushi ShahNoch keine Bewertungen
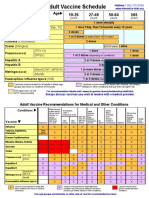
- Adult Vaccine Schedule Eng PDFDokument2 SeitenAdult Vaccine Schedule Eng PDFAbdur RehmanNoch keine Bewertungen
- Respiratory Physio UsmleDokument61 SeitenRespiratory Physio UsmleDr.G.Bhanu Prakash100% (2)
- HHHHDokument36 SeitenHHHHdger11Noch keine Bewertungen
- Biliary Disorders and Pancreatic Conditions ExplainedDokument59 SeitenBiliary Disorders and Pancreatic Conditions ExplainedErick Sioco InsertoNoch keine Bewertungen
- Divine Intervention Episode 13 Step 1 Metabolism Review A: Some MS4Dokument11 SeitenDivine Intervention Episode 13 Step 1 Metabolism Review A: Some MS4Swisskelly1Noch keine Bewertungen
- Checklistfor 45 Yr OldsDokument1 SeiteChecklistfor 45 Yr OldsyohaneskoNoch keine Bewertungen
- Disease of The Biliary TractDokument7 SeitenDisease of The Biliary TractMae DoctoleroNoch keine Bewertungen
- Heme Testing Aid/APLS: Some PGY-1Dokument4 SeitenHeme Testing Aid/APLS: Some PGY-1Swisskelly1Noch keine Bewertungen
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDokument14 SeitenEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaNoch keine Bewertungen
- Assessment and Management of Patients With Biliary DisorderDokument50 SeitenAssessment and Management of Patients With Biliary DisorderZanida ZainonNoch keine Bewertungen
- Gyne History Taking PDFDokument6 SeitenGyne History Taking PDFGokul AdarshNoch keine Bewertungen
- Divine Intervention Episode 5 Cardio A Physiology1Dokument18 SeitenDivine Intervention Episode 5 Cardio A Physiology1Swisskelly1Noch keine Bewertungen
- Pediatrics Modern Day AnalysisDokument144 SeitenPediatrics Modern Day AnalysisDaniyal AzmatNoch keine Bewertungen
- Renal OsteodystrophyDokument4 SeitenRenal OsteodystrophyLuigiNoch keine Bewertungen
- Kaplan Books + Videos Essential USMLE ReviewDokument3 SeitenKaplan Books + Videos Essential USMLE ReviewAditya Pavankumar Ganti100% (1)
- The RX Study Planner - 2021 EditionDokument33 SeitenThe RX Study Planner - 2021 EditionYASSERNoch keine Bewertungen
- Adaptive Leadership The Case of Jacinda New ZealandDokument4 SeitenAdaptive Leadership The Case of Jacinda New ZealandJahnvi AndhariaNoch keine Bewertungen
- Biliary Tree LectureDokument58 SeitenBiliary Tree Lecturesgod34Noch keine Bewertungen
- Lower Gastrointestinal TractDokument45 SeitenLower Gastrointestinal Tractsofia_245Noch keine Bewertungen
- Case Stenosis Aorta + RegurgitationDokument58 SeitenCase Stenosis Aorta + RegurgitationRuth Faustine Jontah RayoNoch keine Bewertungen
- Orgo Cheat Sheets Leah4sci Collection 2018 5192018 PDFDokument32 SeitenOrgo Cheat Sheets Leah4sci Collection 2018 5192018 PDFGian BañaresNoch keine Bewertungen
- Radiology: Dr. Abdulaziz Alsaad Neuroradiology Fellow King Fahad Medical CityDokument22 SeitenRadiology: Dr. Abdulaziz Alsaad Neuroradiology Fellow King Fahad Medical CityAjmal EnsanahNoch keine Bewertungen
- Goljan Respiratory NotesDokument21 SeitenGoljan Respiratory Notesmedic2424100% (1)
- Obs & GynDokument121 SeitenObs & GynSaya K. AkremNoch keine Bewertungen
- Neuroblastoma: A Cancer of the Sympathetic Nervous SystemDokument153 SeitenNeuroblastoma: A Cancer of the Sympathetic Nervous SystemWael ElsawyNoch keine Bewertungen
- Toxicology USMLE NotesDokument15 SeitenToxicology USMLE NotesDuncan JacksonNoch keine Bewertungen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- 14 - Toronto Notes 2011 - GynecologyDokument52 Seiten14 - Toronto Notes 2011 - GynecologyZiyad100% (4)
- Fluid Management in PediatricsDokument3 SeitenFluid Management in PediatricsZiyadNoch keine Bewertungen
- Cyanotic Congenital Heart DiseaseDokument1 SeiteCyanotic Congenital Heart DiseaseZiyadNoch keine Bewertungen
- Prenatal Assessment of FetusDokument1 SeitePrenatal Assessment of FetusZiyadNoch keine Bewertungen
- "Most Common's" in Pediatric CardiologyDokument1 Seite"Most Common's" in Pediatric CardiologyZiyadNoch keine Bewertungen
- Acyanotic Congenital Heart DiseaseDokument2 SeitenAcyanotic Congenital Heart DiseaseZiyad100% (1)
- Typical CSF Findings in Pediatric MeningitisDokument1 SeiteTypical CSF Findings in Pediatric MeningitisZiyadNoch keine Bewertungen
- Instruments & IndicationsDokument11 SeitenInstruments & IndicationsZiyad100% (2)
- Thyroid DiseaseDokument1 SeiteThyroid DiseaseZiyadNoch keine Bewertungen
- Obstetric BleedingDokument1 SeiteObstetric BleedingZiyadNoch keine Bewertungen
- Resume Obs 21-27 Februari 21Dokument6 SeitenResume Obs 21-27 Februari 21imamsantos1191Noch keine Bewertungen
- SecretDokument1 SeiteSecretAyisha LoureliNoch keine Bewertungen
- Pre EclampsiaDokument1 SeitePre EclampsiaRajith AnandNoch keine Bewertungen
- IUGR Case PresentationDokument21 SeitenIUGR Case PresentationAlice ChirilaNoch keine Bewertungen
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsDokument5 SeitenAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiNoch keine Bewertungen
- Intraoperative Surgical Complication During Cesarean SectionDokument14 SeitenIntraoperative Surgical Complication During Cesarean Sectioncarbolico100% (1)
- Lat XiDokument3 SeitenLat XiEsa NadhirNoch keine Bewertungen
- Germiston +27833736090 Dr. Jabulile/cheap Abortion Pills 4 Sale in Germiston/johannesburg ClinicDokument1 SeiteGermiston +27833736090 Dr. Jabulile/cheap Abortion Pills 4 Sale in Germiston/johannesburg Clinicsseruwagi miyodiNoch keine Bewertungen
- Hellp Syndrome ArticleDokument8 SeitenHellp Syndrome ArticleDIANNE FAYE LARAGANNoch keine Bewertungen
- Postterm Pregnancy Risks & Management OptionsDokument5 SeitenPostterm Pregnancy Risks & Management OptionsOmar MohammedNoch keine Bewertungen
- 10 Bahasa Indonesia Kasus Kehamilan MelahirkanDokument164 Seiten10 Bahasa Indonesia Kasus Kehamilan Melahirkancuuphy meryliantNoch keine Bewertungen
- Maternal and Fetal Outcomes in Term Premature Rupture of MembraneDokument6 SeitenMaternal and Fetal Outcomes in Term Premature Rupture of MembraneMuhammad Fikri RidhaNoch keine Bewertungen
- Jurnal Ilmu Kedokteran Dan Kesehatan, Volume 7, Nomor 1, Januari 2020 393Dokument8 SeitenJurnal Ilmu Kedokteran Dan Kesehatan, Volume 7, Nomor 1, Januari 2020 393Nurhalimah HarahapNoch keine Bewertungen
- 1 Persiapan Penanganan Bayi Baru LahirDokument54 Seiten1 Persiapan Penanganan Bayi Baru LahirRosa NinmusuNoch keine Bewertungen
- Lecture-11 Breech PresentationDokument27 SeitenLecture-11 Breech PresentationMadhu Sudhan PandeyaNoch keine Bewertungen
- Abnormalitiesofcordplacenta 140706120521 Phpapp01 PDFDokument65 SeitenAbnormalitiesofcordplacenta 140706120521 Phpapp01 PDFNise Mon KuriakoseNoch keine Bewertungen
- CHORIOAMNIONITISDokument32 SeitenCHORIOAMNIONITISnurul azareeNoch keine Bewertungen
- Pre Eclampsia: Preeclampsia Is A Pregnancy Complication Characterized by High Blood Pressure and Signs of Damage ToDokument3 SeitenPre Eclampsia: Preeclampsia Is A Pregnancy Complication Characterized by High Blood Pressure and Signs of Damage ToSahaaneiy IlmeeNoch keine Bewertungen
- How To Measure Cervical Length: Karl Oliver Kagan and Jiri SonekDokument14 SeitenHow To Measure Cervical Length: Karl Oliver Kagan and Jiri SoneknidoNoch keine Bewertungen
- Understanding Antepartum Haemorrhage (APHDokument18 SeitenUnderstanding Antepartum Haemorrhage (APHSanaNoch keine Bewertungen
- Topic - Version Subject - ObgDokument23 SeitenTopic - Version Subject - ObgMandeep KaurNoch keine Bewertungen
- AbortionsDokument99 SeitenAbortionsAGERI PUSHPALATHANoch keine Bewertungen
- Icd 10 Revisi 2010Dokument45 SeitenIcd 10 Revisi 2010Lena ArdhiyantiNoch keine Bewertungen