Das könnte Ihnen auch gefallen
- Community Health PromotionDokument25 SeitenCommunity Health PromotionShekhar GaddamNoch keine Bewertungen
- Quora ProblemDokument1 SeiteQuora ProblemShekhar GaddamNoch keine Bewertungen
- Human Resources Section4-Textbook On Public Health and Community MedicineDokument24 SeitenHuman Resources Section4-Textbook On Public Health and Community MedicineShekhar GaddamNoch keine Bewertungen
- Social Determinants Health Urban Populations Me Tho Do LocalDokument12 SeitenSocial Determinants Health Urban Populations Me Tho Do LocalShekhar GaddamNoch keine Bewertungen
- Adaptation of Health WHODokument52 SeitenAdaptation of Health WHOShekhar GaddamNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDokument12 SeitenDate Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceSiddhant A. KhankalNoch keine Bewertungen
- Mikron CrazyDrill Crosspilot BrochureDokument8 SeitenMikron CrazyDrill Crosspilot BrochureClaudiu IndreNoch keine Bewertungen
- Feasibility Study Example 35Dokument132 SeitenFeasibility Study Example 35Cyrene JamesNoch keine Bewertungen
- Evaluation Report - Shanthi SewanaDokument2 SeitenEvaluation Report - Shanthi SewanaAnuranga SahampathNoch keine Bewertungen
- Numerical Test 5 SolutionsDokument16 SeitenNumerical Test 5 Solutionslawrence ojuaNoch keine Bewertungen
- Topic Two Financial Mathematics/Time Value of MoneyDokument43 SeitenTopic Two Financial Mathematics/Time Value of Moneysir bookkeeperNoch keine Bewertungen
- Chp.7 Cash and ReceivablesDokument104 SeitenChp.7 Cash and ReceivablesNurindah W RNoch keine Bewertungen
- Factors Affecting iPhone Sales Decline in IndiaDokument7 SeitenFactors Affecting iPhone Sales Decline in IndiaKuhuNoch keine Bewertungen
- ACYCST1 - Hybrid - Syllabus - T32223 - MT ClassDokument8 SeitenACYCST1 - Hybrid - Syllabus - T32223 - MT ClassHannah Jane ToribioNoch keine Bewertungen
- Myntra Project: History, Values, Mission, Philosophy and CSR Initiatives of the Leading Indian Fashion Ecommerce CompanyDokument41 SeitenMyntra Project: History, Values, Mission, Philosophy and CSR Initiatives of the Leading Indian Fashion Ecommerce Companysunilkumbar100% (1)
- Gildemeister - Nef-Plus 710 / 2.000 MM Distance Between CentersDokument9 SeitenGildemeister - Nef-Plus 710 / 2.000 MM Distance Between CentersMarko DekanićNoch keine Bewertungen
- Non Salary Budget Proforma NSB Proforma For Schools Education Department 2014 2015Dokument4 SeitenNon Salary Budget Proforma NSB Proforma For Schools Education Department 2014 2015Humraz AliNoch keine Bewertungen
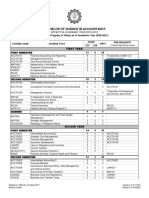
- Cit U Bsa ProspectusDokument4 SeitenCit U Bsa ProspectusRheneir MoraNoch keine Bewertungen
- Crafting Guide AlbionDokument79 SeitenCrafting Guide Albionjoaquin reyesNoch keine Bewertungen
- Toaz - Info Summer Internship Report On Digital Marketing PRDokument30 SeitenToaz - Info Summer Internship Report On Digital Marketing PRAli AhmadNoch keine Bewertungen
- #5745654-Healthcare Administrators - EditedDokument9 Seiten#5745654-Healthcare Administrators - EditedAlphonce KipronoNoch keine Bewertungen
- PDS - BridgingF-i v1.5 080720 ENGDokument2 SeitenPDS - BridgingF-i v1.5 080720 ENGFairuz MohdNoch keine Bewertungen
- MEP Guidebook 2Dokument2 SeitenMEP Guidebook 2Christopher LimNoch keine Bewertungen
- Week 14 Ellen Moore CaseDokument9 SeitenWeek 14 Ellen Moore Casegr4ng3Noch keine Bewertungen
- Assignment 1Dokument7 SeitenAssignment 1Haftamu TekleNoch keine Bewertungen
- 11 - Notice of Appointment Various Positions POM MICP Cebu Leg SubicDokument3 Seiten11 - Notice of Appointment Various Positions POM MICP Cebu Leg Subicmitch galaxNoch keine Bewertungen
- #2 Evolution of QualityDokument5 Seiten#2 Evolution of QualityCarolyn vestidasNoch keine Bewertungen
- Credit Card StatementDokument1 SeiteCredit Card Statementcharlene carter100% (2)
- InvoiceDokument1 SeiteInvoiceOfik TaufikNoch keine Bewertungen
- GHS Hazard Comm Labeling & SDS - 1Dokument61 SeitenGHS Hazard Comm Labeling & SDS - 1Rosiawan Sasambo100% (1)
- 110606-9 KA26 GT26 Technology Update Vietnam - HandoutDokument68 Seiten110606-9 KA26 GT26 Technology Update Vietnam - Handouttrungnq_ktd97Noch keine Bewertungen
- (PFM) WK 3 CapitalismDokument16 Seiten(PFM) WK 3 CapitalismAngel BNoch keine Bewertungen
- Overheard Accounting MathDokument18 SeitenOverheard Accounting Mathfaraaz360Noch keine Bewertungen
- NSPO Editable1Dokument6 SeitenNSPO Editable1Sarlyn AquinoNoch keine Bewertungen
- World Policy Journal: Bangladesh: A Labor ParadoxDokument11 SeitenWorld Policy Journal: Bangladesh: A Labor ParadoxPranto BaraiNoch keine Bewertungen