Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Advisory Guidelines For NRIC Numbers - 310818Dokument15 SeitenAdvisory Guidelines For NRIC Numbers - 310818Clement ChanNoch keine Bewertungen
- 22975/Bdts RMR Sfast Sleeper Class (SL)Dokument2 Seiten22975/Bdts RMR Sfast Sleeper Class (SL)dilkhush6198Noch keine Bewertungen
- ANDiS CAMS Product Description 1 - 5 V 2.1Dokument41 SeitenANDiS CAMS Product Description 1 - 5 V 2.1ehtisham1Noch keine Bewertungen
- EvalDokument1 SeiteEvalRafael John Guiraldo OaniNoch keine Bewertungen
- Special Power of Attorney For NRE / NRO / FCNR (B) Accounts Standard InstructionsDokument3 SeitenSpecial Power of Attorney For NRE / NRO / FCNR (B) Accounts Standard InstructionsKoteswara Rao PasupuletiNoch keine Bewertungen
- Face Recognigion-SystemDokument30 SeitenFace Recognigion-SystemOliifan BaayyooNoch keine Bewertungen
- دامتعلال يملاعلا تاراملإا زكرم Emirates International Accreditation CenterDokument22 Seitenدامتعلال يملاعلا تاراملإا زكرم Emirates International Accreditation CenterKannan LakshmananNoch keine Bewertungen
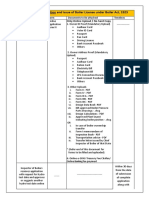
- 4 Boiler Registration and RenewalDokument7 Seiten4 Boiler Registration and RenewalGnanasekar VaishniNoch keine Bewertungen
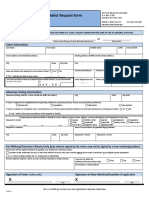
- NC Absentee Ballot Request FormDokument2 SeitenNC Absentee Ballot Request FormAnonymous X3NoCINoch keine Bewertungen
- Understanding The Benefits: SSA - GovDokument32 SeitenUnderstanding The Benefits: SSA - GovVhince GreenNoch keine Bewertungen
- FREQUENTLY ASKED QUESTIONS - Vetted by Fit India QuizDokument8 SeitenFREQUENTLY ASKED QUESTIONS - Vetted by Fit India Quizakhil tyagiNoch keine Bewertungen
- UCD International Student Handbook 2014 INSERTS 108pg A5 PREVIEW High Res ISSUUDokument109 SeitenUCD International Student Handbook 2014 INSERTS 108pg A5 PREVIEW High Res ISSUUHakita Belson Pardamean SinagaNoch keine Bewertungen
- 12786/kacheguda Exp Sleeper Class (SL)Dokument2 Seiten12786/kacheguda Exp Sleeper Class (SL)Kartik H ANoch keine Bewertungen
- DOF-RO Form 91Dokument6 SeitenDOF-RO Form 91Bobby Olavides SebastianNoch keine Bewertungen
- Personal Load in SbiDokument42 SeitenPersonal Load in SbiNitinAgnihotriNoch keine Bewertungen
- Checklist of Requirements - Job Order (Landbased) For POLO OWWADokument1 SeiteChecklist of Requirements - Job Order (Landbased) For POLO OWWAMaybelNoch keine Bewertungen
- How To Get Married in Romania - Full GuideDokument10 SeitenHow To Get Married in Romania - Full GuideAdrian PurgulyNoch keine Bewertungen
- Trips Flight DownloadETicketDokument4 SeitenTrips Flight DownloadETicketAccounts NeemansNoch keine Bewertungen
- MR Vijay Bhatt: AESPB5466PDokument4 SeitenMR Vijay Bhatt: AESPB5466Pfnopulse100% (1)
- Federal Public Service Commission: Aga Khan Road, Sector F-5/ 1, ISLAMABADDokument3 SeitenFederal Public Service Commission: Aga Khan Road, Sector F-5/ 1, ISLAMABADshahid hussainNoch keine Bewertungen
- NM Project - Project 1Dokument34 SeitenNM Project - Project 1littlemagicpkNoch keine Bewertungen
- Receipt For Driving SchoolDokument2 SeitenReceipt For Driving SchoolBhavin VyasaNoch keine Bewertungen
- By MR - Vikram JoshiDokument56 SeitenBy MR - Vikram Joshimayurimehta1Noch keine Bewertungen
- 1 8770079894 PDFDokument30 Seiten1 8770079894 PDFSatyam MaramNoch keine Bewertungen
- Https WWW - Irctc.co - in Eticketing Printticket - JSF PNR 2253304869 B 17-Dec-2018 0 PDFDokument1 SeiteHttps WWW - Irctc.co - in Eticketing Printticket - JSF PNR 2253304869 B 17-Dec-2018 0 PDFसद्दाम हुसैनNoch keine Bewertungen
- 21CFR11 Ignition Compliance 3 165359Dokument11 Seiten21CFR11 Ignition Compliance 3 165359Vicente AntonioNoch keine Bewertungen
- Saln 2012 Blank FormDokument3 SeitenSaln 2012 Blank FormGel KorlanNoch keine Bewertungen
- Application Form For Landing Rights Broadcasting LicenceDokument13 SeitenApplication Form For Landing Rights Broadcasting LicenceKCSE REVISIONNoch keine Bewertungen
- Ayor'S Message: City of Cebu Republic of The PhilippinesDokument186 SeitenAyor'S Message: City of Cebu Republic of The PhilippinestrecemarieNoch keine Bewertungen
- SOP Food DefenceDokument5 SeitenSOP Food DefenceIsna Andrianto100% (6)