Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Lung Cancer - Symptoms and Causes - Mayo ClinicDokument9 SeitenLung Cancer - Symptoms and Causes - Mayo ClinicTakuranashe DebweNoch keine Bewertungen
- The Real Paul Thibault: Nothing But The Truth..Dokument20 SeitenThe Real Paul Thibault: Nothing But The Truth..LancasterFirstNoch keine Bewertungen
- Kaplan Grade OverviewDokument5 SeitenKaplan Grade Overviewapi-310875630Noch keine Bewertungen
- Pediatric Malignant Bone TumoursDokument28 SeitenPediatric Malignant Bone TumourscorneliusNoch keine Bewertungen
- A Harmonious Smile: Biological CostsDokument12 SeitenA Harmonious Smile: Biological Costsjsjs kaknsbsNoch keine Bewertungen
- Speaking Level Placement Test Business English PDFDokument2 SeitenSpeaking Level Placement Test Business English PDFLee HarrisonNoch keine Bewertungen
- A Deep Learning Approach To Antibiotic DiscoveryDokument29 SeitenA Deep Learning Approach To Antibiotic DiscoveryDeepika ChhabraNoch keine Bewertungen
- Rosemont Hill Health CenterDokument14 SeitenRosemont Hill Health CenterMona SahooNoch keine Bewertungen
- Nursing Interventions for Ineffective Airway ClearanceDokument3 SeitenNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- IFCC Visiting LectureDokument3 SeitenIFCC Visiting LectureMaruhum NurNoch keine Bewertungen
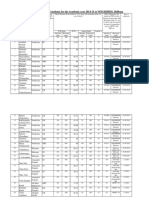
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Dokument10 SeitenAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNoch keine Bewertungen
- 4bi1 - Jan22 2b QPDokument28 Seiten4bi1 - Jan22 2b QPXIN PEINoch keine Bewertungen
- Detailed Advertisement of Various GR B & C 2023 - 0 PDFDokument47 SeitenDetailed Advertisement of Various GR B & C 2023 - 0 PDFMukul KostaNoch keine Bewertungen
- Dapagliflozin Uses, Dosage, Side Effects, WarningsDokument8 SeitenDapagliflozin Uses, Dosage, Side Effects, WarningspatgarettNoch keine Bewertungen
- Strupp ArticleDokument10 SeitenStrupp ArticleDental SpaNoch keine Bewertungen
- Guidelines For Good Distribution Practices For Drugs, Cosmetics, Medical Devices and Household Chemical SubstancesDokument4 SeitenGuidelines For Good Distribution Practices For Drugs, Cosmetics, Medical Devices and Household Chemical SubstancessboaduappiahNoch keine Bewertungen
- BG Gluc2Dokument3 SeitenBG Gluc2Nghi NguyenNoch keine Bewertungen
- Social Welfare Administrartion McqsDokument2 SeitenSocial Welfare Administrartion McqsAbd ur Rehman Vlogs & VideosNoch keine Bewertungen
- Chirangi vs. StateDokument3 SeitenChirangi vs. StateFaithNoch keine Bewertungen
- Everything You Need to Know About Prenatal CareDokument5 SeitenEverything You Need to Know About Prenatal Carelaura fernandiaNoch keine Bewertungen
- MG English Consumer BookletDokument41 SeitenMG English Consumer BookletAnh HoaiNoch keine Bewertungen
- Hypertension Drugs Cheat Sheet: by ViaDokument3 SeitenHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNoch keine Bewertungen
- Dat IatDokument4 SeitenDat Iatscribd birdNoch keine Bewertungen
- L-Sit ProgressionsDokument2 SeitenL-Sit ProgressionsMattNoch keine Bewertungen
- 32 Vol4 EpaperDokument32 Seiten32 Vol4 EpaperThesouthasian TimesNoch keine Bewertungen
- HACCP Plan Distribution Cold ChainDokument23 SeitenHACCP Plan Distribution Cold ChainHACCPEuropa86% (7)
- Experential and Relationship Oriented Approaches 1Dokument12 SeitenExperential and Relationship Oriented Approaches 1Mary Ann CabalejoNoch keine Bewertungen
- Immersion Death: Dr. Rayyan Al-AliDokument42 SeitenImmersion Death: Dr. Rayyan Al-AliRayyan AlaliNoch keine Bewertungen
- Understanding the Brain Through Microscopic AnalysisDokument4 SeitenUnderstanding the Brain Through Microscopic AnalysisNoah VoelkerNoch keine Bewertungen
- BSHF-101 E.MDokument8 SeitenBSHF-101 E.MRajni KumariNoch keine Bewertungen