Das könnte Ihnen auch gefallen
- Caffeine Effects On Cardiovascular and Neuroendocrine Responses To Acute Psychosocial Stress and Their Relationship To Level of Habitual Caffeine ConsumptionDokument17 SeitenCaffeine Effects On Cardiovascular and Neuroendocrine Responses To Acute Psychosocial Stress and Their Relationship To Level of Habitual Caffeine ConsumptionJenni MarshallNoch keine Bewertungen
- Examining The Effects of Caffeine On Students' Academic PerformancesDokument5 SeitenExamining The Effects of Caffeine On Students' Academic PerformancesPunPun Ranchana WorahanNoch keine Bewertungen
- Caffeine Dependency, Students' Views On Its Effects Towards Their Behavior in ClassDokument55 SeitenCaffeine Dependency, Students' Views On Its Effects Towards Their Behavior in ClassReluya Alyssa KarylleNoch keine Bewertungen
- Effects of Caffeine On Cognitive TaskDokument92 SeitenEffects of Caffeine On Cognitive TaskJerome Ventura BalgosNoch keine Bewertungen
- Caffeine Intake and Its Correlation To Concentration Skills of The Senior High School Students of Ina NG Buhay Catholic SchoolDokument40 SeitenCaffeine Intake and Its Correlation To Concentration Skills of The Senior High School Students of Ina NG Buhay Catholic SchoolHyun Su LeeNoch keine Bewertungen
- Caffeine Consumption, Intoxication, and Stress Among Female University Students: A Cross-Sectional StudyDokument10 SeitenCaffeine Consumption, Intoxication, and Stress Among Female University Students: A Cross-Sectional Studyakariyoshida27Noch keine Bewertungen
- Caffeine Dependence Fact SheetDokument7 SeitenCaffeine Dependence Fact Sheetapi-317394115Noch keine Bewertungen
- Chapter 1 - CaffeineDokument11 SeitenChapter 1 - Caffeinejimpertubal100% (1)
- Caffeine Literature Review-2Dokument6 SeitenCaffeine Literature Review-2api-609577576100% (1)
- Neuropsychological Effects of Caffeine Is Caffeine Addictive 2161 0487 1000295 PDFDokument12 SeitenNeuropsychological Effects of Caffeine Is Caffeine Addictive 2161 0487 1000295 PDFAli ShahNoch keine Bewertungen
- Caffeine in The Management of Patients With Headache: Reviewarticle Open AccessDokument11 SeitenCaffeine in The Management of Patients With Headache: Reviewarticle Open AccessSandroLaoNoch keine Bewertungen
- Effects of Coffee/caffeine On Brain Health and Disease: What Should I Tell My Patients?Dokument7 SeitenEffects of Coffee/caffeine On Brain Health and Disease: What Should I Tell My Patients?Mher Karizze Anne R. NarcisoNoch keine Bewertungen
- CaffeineDokument11 SeitenCaffeineDuch Guillen SoloveresNoch keine Bewertungen
- Surfactant Replacement TherapyDokument42 SeitenSurfactant Replacement TherapyPayas JoshiNoch keine Bewertungen
- GA5 Caffeine Consumption Huda AbdulazizDokument14 SeitenGA5 Caffeine Consumption Huda Abdulazizmaha abdallahNoch keine Bewertungen
- Titrimetric Analysis of Amino Acids and PeptidesDokument6 SeitenTitrimetric Analysis of Amino Acids and PeptidespaulocarpioNoch keine Bewertungen
- N503 Non-Experimental WK 5Dokument23 SeitenN503 Non-Experimental WK 5asghaznavi100% (1)
- RRL2Dokument9 SeitenRRL2Queen SiLogNoch keine Bewertungen
- Chem112 EssayDokument2 SeitenChem112 EssaykaryaNoch keine Bewertungen
- Effects of Caffeine On Heart RateDokument10 SeitenEffects of Caffeine On Heart RateKoko Nur IzzatiNoch keine Bewertungen
- APA Lab Report FormatDokument7 SeitenAPA Lab Report FormatNymphetamine010% (1)
- Introduction To Research MethodsDokument46 SeitenIntroduction To Research MethodssiddhajoesNoch keine Bewertungen
- Kapeng Barako OriginDokument2 SeitenKapeng Barako OriginCes UniqueNoch keine Bewertungen
- Writing Lab Reports and Scientific Papers: by Warren D. Dolphin Iowa State UniversityDokument5 SeitenWriting Lab Reports and Scientific Papers: by Warren D. Dolphin Iowa State UniversityMariana Muguerza100% (1)
- Test Conceptualization: Norm-Referenced Vs Criterion-ReferencedDokument7 SeitenTest Conceptualization: Norm-Referenced Vs Criterion-ReferencedNarona MaurenNoch keine Bewertungen
- The Thurstone Temperament Schedule As An Instrument of SupervisorDokument72 SeitenThe Thurstone Temperament Schedule As An Instrument of Supervisoracordero0% (1)
- Asprin Lab ReportDokument10 SeitenAsprin Lab ReportMohamedNoch keine Bewertungen
- Effect of Breakfast Skipping On Young Females MenstruationDokument16 SeitenEffect of Breakfast Skipping On Young Females MenstruationRininta EnggartiastiNoch keine Bewertungen
- The Relationship of Body Image Disturbance On The Eating Habits Among Male and Female Students of Cebu Doctors' UniversityDokument90 SeitenThe Relationship of Body Image Disturbance On The Eating Habits Among Male and Female Students of Cebu Doctors' UniversityLesley CedroNoch keine Bewertungen
- Osmosis Practical Write UPDokument13 SeitenOsmosis Practical Write UPSanngeetaNoch keine Bewertungen
- How Caffeine Affects The Heart Rate of DaphniaDokument2 SeitenHow Caffeine Affects The Heart Rate of DaphniaMianto NamikazeNoch keine Bewertungen
- Biopsychology: Ninth EditionDokument24 SeitenBiopsychology: Ninth EditionJasleen Kaur100% (1)
- Chemistry Lab ReportDokument20 SeitenChemistry Lab Reportapi-350436359Noch keine Bewertungen
- Reflective Essay Guide.Dokument4 SeitenReflective Essay Guide.Aldana RodríguezNoch keine Bewertungen
- Imogene King: Goal Attainment TheoryDokument17 SeitenImogene King: Goal Attainment TheoryRozel EncarnacionNoch keine Bewertungen
- Purpose of ResearchDokument2 SeitenPurpose of Researchchooseruby100% (1)
- CredoDokument1 SeiteCredoCamille Abigail VivoNoch keine Bewertungen
- Caffeine StudyDokument45 SeitenCaffeine StudyKryshia MiparanumNoch keine Bewertungen
- Data Analysis, Interpretation, and Reporting: Eve 9810001M Sabrina 9810002MDokument25 SeitenData Analysis, Interpretation, and Reporting: Eve 9810001M Sabrina 9810002MPrashant DwivediNoch keine Bewertungen
- The Effect of Conformity On Estimating The Number of Sweets in A JarDokument13 SeitenThe Effect of Conformity On Estimating The Number of Sweets in A JarDominic Nico Areago100% (1)
- PDF Academic Performance QuestionnaireDokument2 SeitenPDF Academic Performance Questionnairealmayasa2002Noch keine Bewertungen
- Biochem Journal CritiqueDokument7 SeitenBiochem Journal CritiqueDiane TomogbongNoch keine Bewertungen
- Patient Education For Patient With Anorexia NervosaDokument2 SeitenPatient Education For Patient With Anorexia NervosaRidha Ramdani RahmahNoch keine Bewertungen
- Problem Statement CaffeineDokument2 SeitenProblem Statement Caffeinearissa razaliNoch keine Bewertungen
- The Problem and Its BackgroundDokument37 SeitenThe Problem and Its BackgroundJustin ApolonioNoch keine Bewertungen
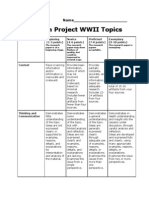
- Research Project RubricDokument2 SeitenResearch Project Rubricapi-252976458Noch keine Bewertungen
- Final - Daphnia Heart Rate ReportDokument15 SeitenFinal - Daphnia Heart Rate ReportWill PerkinsNoch keine Bewertungen
- 8224-Cover Letter-32202-1-4-20230320Dokument3 Seiten8224-Cover Letter-32202-1-4-20230320Muhammad HusinNoch keine Bewertungen
- Activity 6 Laboratory ProcedureDokument7 SeitenActivity 6 Laboratory ProcedureAinie JuripaeNoch keine Bewertungen
- Behavioral Addiction Versus Substance Addiction: Correspondence of Psychiatric and Psychological ViewsDokument5 SeitenBehavioral Addiction Versus Substance Addiction: Correspondence of Psychiatric and Psychological ViewsBiljana GagachovskaNoch keine Bewertungen
- Occupational Stress: A Comparative Study Among Doctors of Hospitals of HaryanaDokument12 SeitenOccupational Stress: A Comparative Study Among Doctors of Hospitals of Haryanashanu kumarNoch keine Bewertungen
- (Schematic Diagram) : Predisposing Factors Precipitating FactorsDokument5 Seiten(Schematic Diagram) : Predisposing Factors Precipitating FactorsGraiLe Joy Palbusa Ngina-BadayNoch keine Bewertungen
- Assignment ANOVADokument21 SeitenAssignment ANOVAsuhaimi sobrieNoch keine Bewertungen
- Bio Paper FinalDokument8 SeitenBio Paper FinalNiem PhamNoch keine Bewertungen
- Dying To Be Thin ReviewDokument5 SeitenDying To Be Thin Reviewapi-242071284Noch keine Bewertungen
- Experimental ResearchDokument1 SeiteExperimental ResearchCharmen Diaz RamosNoch keine Bewertungen
- Anxiety in Major Depression: Relationship To Suicide AttemptsDokument5 SeitenAnxiety in Major Depression: Relationship To Suicide AttemptsRen DNoch keine Bewertungen
- Effect of Caffeine On Cognitive Functions 1Dokument4 SeitenEffect of Caffeine On Cognitive Functions 1polapNoch keine Bewertungen
- Sample of Coffee and There Caffeine ContentDokument21 SeitenSample of Coffee and There Caffeine Contentadhyayan2107Noch keine Bewertungen
- Caffeine Research PaperDokument7 SeitenCaffeine Research Paperfznn7hzd100% (1)
- Decimal Unit PlanDokument17 SeitenDecimal Unit Planapi-288753185Noch keine Bewertungen
- Anti Romantic - Full PDFDokument4 SeitenAnti Romantic - Full PDFSergio Diaz Phyll'zNoch keine Bewertungen
- Cozy InteriorityDokument22 SeitenCozy InteriorityErica de OliveiraNoch keine Bewertungen
- Amity International School Vasundhara, Sector-6: Holiday Homework (2011-2012) Class IxDokument8 SeitenAmity International School Vasundhara, Sector-6: Holiday Homework (2011-2012) Class IxfacebookmaneeshNoch keine Bewertungen
- Flip Module 3D Page PDFDokument110 SeitenFlip Module 3D Page PDFPixyorizaNoch keine Bewertungen
- Academic Emotions in Students' Self-Regulated Learning and AchievementDokument15 SeitenAcademic Emotions in Students' Self-Regulated Learning and AchievementAldo RamirezNoch keine Bewertungen
- Daryl Mahon - Evidence Based Counselling & Psychotherapy For The 21st Century Practitioner-Emerald Publishing (2023)Dokument197 SeitenDaryl Mahon - Evidence Based Counselling & Psychotherapy For The 21st Century Practitioner-Emerald Publishing (2023)Mariano ScandarNoch keine Bewertungen
- Homework 1Dokument10 SeitenHomework 1Nam Anh KiraiNoch keine Bewertungen
- Popular Sovereignty Is EnoughDokument4 SeitenPopular Sovereignty Is EnoughdominatedebateNoch keine Bewertungen
- 20 ASL Circular-1 PDFDokument3 Seiten20 ASL Circular-1 PDFAlagu MurugesanNoch keine Bewertungen
- Age Term Date Student Instrument Teacher: E E G GDokument1 SeiteAge Term Date Student Instrument Teacher: E E G GAustin SalsburyNoch keine Bewertungen
- Check List For Module 2 Krishna SevakDokument1 SeiteCheck List For Module 2 Krishna SevakHitesh sunshineNoch keine Bewertungen
- Little Fears - Cry HavocDokument9 SeitenLittle Fears - Cry HavocDaniel PaganoNoch keine Bewertungen
- Ayer - Knowledge Right To Be SureDokument3 SeitenAyer - Knowledge Right To Be SurescrbdggggNoch keine Bewertungen
- THESIS-CHAPTER-1-3-revised 1Dokument36 SeitenTHESIS-CHAPTER-1-3-revised 1Michael AndalNoch keine Bewertungen
- The True Rosicrucian & Holy Grail Traditions - Online CoursesDokument8 SeitenThe True Rosicrucian & Holy Grail Traditions - Online CoursesPanther PantherNoch keine Bewertungen
- Assignment QuestionsDokument5 SeitenAssignment Questionsvijay1vijay2147Noch keine Bewertungen
- Counseling Theories Final PaperDokument11 SeitenCounseling Theories Final Paperapi-334628919Noch keine Bewertungen
- Research Methodology - Unit 2 - Week 1 - Group Discussion On ResearchDokument3 SeitenResearch Methodology - Unit 2 - Week 1 - Group Discussion On ResearchE.GANGADURAI AP-I - ECENoch keine Bewertungen
- Final Action Research For PrintingDokument21 SeitenFinal Action Research For PrintingJeurdecel Laborada Castro - MartizanoNoch keine Bewertungen
- Summative Test in Research Vii - First Quarter1Dokument2 SeitenSummative Test in Research Vii - First Quarter1Rodarbal Zerimar Hteb100% (5)
- UbD Animal FarmDokument3 SeitenUbD Animal FarmAlisha Nangia100% (1)
- Structured Learning Experiences - GamesDokument7 SeitenStructured Learning Experiences - GamesSemajmarx007100% (1)
- The Business Advanced Sample Pages Students BookDokument8 SeitenThe Business Advanced Sample Pages Students BookВиктория СуховаяNoch keine Bewertungen
- Building A High Performance CultureDokument14 SeitenBuilding A High Performance Culturenavinvijay2Noch keine Bewertungen
- Aura Soma Bottle MeaningsDokument27 SeitenAura Soma Bottle MeaningsLiz Wang80% (5)
- Click Here For Download: (PDF) How The Brain Learns David A. Sousa - Download PDF Book FreeDokument2 SeitenClick Here For Download: (PDF) How The Brain Learns David A. Sousa - Download PDF Book FreeSalis FadliNoch keine Bewertungen
- Republic of The Philippines Department of Education Region XII Kenram, Isulan, Sultan KudaratDokument2 SeitenRepublic of The Philippines Department of Education Region XII Kenram, Isulan, Sultan KudaratRayan CastroNoch keine Bewertungen
- Handout - Functions of ManagementDokument3 SeitenHandout - Functions of ManagementStephanie DecidaNoch keine Bewertungen
- Ohms Law Lesson-PlanDokument3 SeitenOhms Law Lesson-PlanNoor Ayesha SultanaNoch keine Bewertungen