Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- SOCIETY Culture With Family PlanningDokument1 SeiteSOCIETY Culture With Family PlanningyabaeveNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- DEPED UNICEF Disaster Risk Reduction Resource ManualDokument94 SeitenDEPED UNICEF Disaster Risk Reduction Resource ManualNicolai AquinoNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Disaster Readiness and Risk Reduction HandoutsDokument4 SeitenDisaster Readiness and Risk Reduction HandoutsyabaeveNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The Four Priorities For ActionDokument2 SeitenThe Four Priorities For ActionyabaeveNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Your Scenarios Here Are Examples of The Three Types of Fluid Volume DeficitDokument2 SeitenYour Scenarios Here Are Examples of The Three Types of Fluid Volume DeficityabaeveNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- HttpsDokument4 SeitenHttpsyabaeveNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
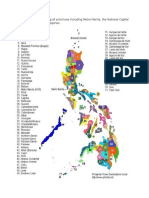
- Philippine Map Indicating All Provinces Including Metro Manila, The National Capital Region (NCR) of The PhilippinesDokument1 SeitePhilippine Map Indicating All Provinces Including Metro Manila, The National Capital Region (NCR) of The PhilippinesyabaeveNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Heat Capacity FormulaDokument6 SeitenHeat Capacity FormulayabaeveNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- How To Remove System Volume Info in Usb DriveDokument1 SeiteHow To Remove System Volume Info in Usb DriveyabaeveNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Anatomy SyllabusDokument7 SeitenAnatomy SyllabusyabaeveNoch keine Bewertungen
- Club Election ScriptDokument2 SeitenClub Election ScriptyabaeveNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Answer SheetsDokument1 SeiteAnswer SheetsyabaeveNoch keine Bewertungen
- E213 Bleeding Control Shock ManagementDokument1 SeiteE213 Bleeding Control Shock ManagementyabaeveNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Weather and Climate ChangeDokument6 SeitenWeather and Climate ChangeyabaeveNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Guide On Childhood Immunization 2014Dokument1 SeiteGuide On Childhood Immunization 2014yabaeveNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- IDRN 1300 Spear v5 20120110Dokument6 SeitenIDRN 1300 Spear v5 20120110yabaeveNoch keine Bewertungen
- DocDokument8 SeitenDocyabaeveNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- General ScienceDokument147 SeitenGeneral ScienceyabaeveNoch keine Bewertungen
- Computer Safety Do and No ListDokument18 SeitenComputer Safety Do and No ListyabaeveNoch keine Bewertungen
- I2Dokument9 SeitenI2yabaeveNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Community First Aid and Emergency Extrication Training Course SyllabusDokument1 SeiteCommunity First Aid and Emergency Extrication Training Course SyllabusyabaeveNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Biology Finals 1bDokument1 SeiteBiology Finals 1byabaeveNoch keine Bewertungen
- Earthquake and Fire DrillDokument51 SeitenEarthquake and Fire Drillyabaeve100% (1)
- Lesson 1Dokument5 SeitenLesson 1yabaeveNoch keine Bewertungen
- Environmental Science SyllabusDokument4 SeitenEnvironmental Science Syllabusyabaeve100% (5)
- Geological SyllabusDokument3 SeitenGeological SyllabusyabaeveNoch keine Bewertungen
- China Is A Socialist Country. The Government Owns and Controls Almost All Natural ResourcesDokument6 SeitenChina Is A Socialist Country. The Government Owns and Controls Almost All Natural ResourcesyabaeveNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Food Production and DistributionDokument9 SeitenFood Production and DistributionyabaeveNoch keine Bewertungen
- BayabanDear SirDokument1 SeiteBayabanDear SirEduard Espeso Chiong-Gandul Jr.Noch keine Bewertungen
- Geological Science Final Examination: 1. Stages of Thunder Storm 10-12 (Plate Boundaries)Dokument1 SeiteGeological Science Final Examination: 1. Stages of Thunder Storm 10-12 (Plate Boundaries)yabaeveNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)