Das könnte Ihnen auch gefallen
- ECGDokument6 SeitenECGMatthew MackeyNoch keine Bewertungen
- Pakya ECG BasicsDokument5 SeitenPakya ECG BasicsFrederick CokroNoch keine Bewertungen
- ECG Master Class-2Dokument138 SeitenECG Master Class-2Shohag ID Center100% (1)
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDokument88 SeitenAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNoch keine Bewertungen
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsVon EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNoch keine Bewertungen
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Von EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Noch keine Bewertungen
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookVon EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNoch keine Bewertungen
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasVon EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasBewertung: 3 von 5 Sternen3/5 (5)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Von EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Noch keine Bewertungen
- Heart Arrhythmias, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHeart Arrhythmias, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- May/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12Dokument3 SeitenMay/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12is_aradanas0% (1)
- Dysrhythmias ChartDokument6 SeitenDysrhythmias Chartjkrix100% (1)
- EKG Practice TestDokument16 SeitenEKG Practice TestAbdul Rohim100% (1)
- Ekg Guidelines PDFDokument7 SeitenEkg Guidelines PDFd.ramadhan100% (1)
- Inherent Rates: Cardiovascular System Alterations Module BDokument7 SeitenInherent Rates: Cardiovascular System Alterations Module Bmp_329Noch keine Bewertungen
- EKG Flash CardsDokument5 SeitenEKG Flash CardsRyann Sampino FreitasNoch keine Bewertungen
- Ecg Reading NotesDokument17 SeitenEcg Reading NotesMarian FloresNoch keine Bewertungen
- A Simplified ECG GuideDokument4 SeitenA Simplified ECG GuidekaelenNoch keine Bewertungen
- EKG Rhythms2 PDFDokument7 SeitenEKG Rhythms2 PDFAya KamajayaNoch keine Bewertungen
- Common Cardiac Related MedicationsDokument18 SeitenCommon Cardiac Related MedicationsTracy100% (2)
- ArrhythmiaDokument2 SeitenArrhythmiaChris Pritchard93% (30)
- ECG InterpretationDokument40 SeitenECG InterpretationMuhammad BadrushshalihNoch keine Bewertungen
- Ecg Cheat Sheet 35Dokument2 SeitenEcg Cheat Sheet 35jessjaylee80% (5)
- EKG Cheat SheetDokument9 SeitenEKG Cheat SheetAlert Twitter100% (5)
- Reading A EKGDokument10 SeitenReading A EKGMayer Rosenberg100% (15)
- Basic Arrhythmia RulesDokument3 SeitenBasic Arrhythmia Rulesgreenflames0997% (30)
- ACLS EKG Rhythms and InterpretationDokument10 SeitenACLS EKG Rhythms and Interpretationdonheyzz_02Noch keine Bewertungen
- EKG InterpretationDokument65 SeitenEKG Interpretationpaskariatne probo dewi100% (1)
- EKG+Mastery +ischemia PDFDokument6 SeitenEKG+Mastery +ischemia PDFCatur Ari Intan PuspitasariNoch keine Bewertungen
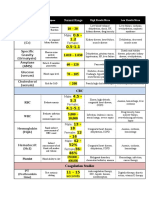
- Lab ValuesDokument3 SeitenLab Valuessurviving nursing school100% (1)
- Critical Care - Hemodynamic Monitoring TableDokument7 SeitenCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- EKG Cheat Sheet - Henry Del RosarioDokument1 SeiteEKG Cheat Sheet - Henry Del RosarioanwarNoch keine Bewertungen
- Cardiac Rhythms and DysrhythmiasDokument14 SeitenCardiac Rhythms and DysrhythmiasShawn Gaurav Jha100% (1)
- ECG ReadingDokument11 SeitenECG ReadingSuresh Shrestha100% (1)
- Basic EKG InterpretationDokument4 SeitenBasic EKG InterpretationPRaDo PATNoch keine Bewertungen
- Cardiac Dysrhythmia Chart Med-Surg NUR4Dokument3 SeitenCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2096% (97)
- 11 Steps of ECG - Ali Alnahari PDFDokument16 Seiten11 Steps of ECG - Ali Alnahari PDFBìnhNoch keine Bewertungen
- Sinus Rhythm DisturbancesDokument3 SeitenSinus Rhythm DisturbancesMarcus Philip GonzalesNoch keine Bewertungen
- Word AssociationDokument27 SeitenWord AssociationMilan Kolovrat100% (1)
- EKG Pocket GuideDokument2 SeitenEKG Pocket GuideFabian Ramirez HincapiéNoch keine Bewertungen
- Krishnan - EKG Basics Lecture NotesDokument3 SeitenKrishnan - EKG Basics Lecture NotesanishdNoch keine Bewertungen
- ECG Master Class-1Dokument132 SeitenECG Master Class-1Shohag ID Center100% (1)
- ArrhyDokument26 SeitenArrhyMouriyan AmanNoch keine Bewertungen
- Murmurs Made Easy PDFDokument3 SeitenMurmurs Made Easy PDFTanya GnNoch keine Bewertungen
- Ekg Cheat SheetDokument2 SeitenEkg Cheat Sheetdectricdf26505100% (1)
- EKG Quick Reference ChartDokument4 SeitenEKG Quick Reference ChartMildaNoch keine Bewertungen
- Cardiac DysrhythmiasDokument3 SeitenCardiac DysrhythmiasKatherine Santiago92% (62)
- ECG Made Easy by Mallareddy SripujaDokument46 SeitenECG Made Easy by Mallareddy Sripujagrreddy836100% (3)
- This Study Resource Was Shared Via: Sinus BradycardiaDokument3 SeitenThis Study Resource Was Shared Via: Sinus BradycardiaPascal St Peter NwaorguNoch keine Bewertungen
- ArythmiaDokument345 SeitenArythmiaMuhammad ArifinNoch keine Bewertungen
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDokument4 SeitenLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNoch keine Bewertungen
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDokument102 SeitenElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNoch keine Bewertungen
- Cardiac DrugsDokument5 SeitenCardiac Drugseric100% (17)
- PANCE - Cardio Review 2020Dokument50 SeitenPANCE - Cardio Review 2020Siam100% (1)
- 100 Essential Drugs1Dokument8 Seiten100 Essential Drugs1Matt McGlothlin85% (13)
- Sally Aburumman Bushra SaleemDokument75 SeitenSally Aburumman Bushra SaleemAbdulrahman AlsayyedNoch keine Bewertungen
- English GuideDokument85 SeitenEnglish GuideanandkishoreNoch keine Bewertungen
- 1 - Patient Evaluation, Diagnosis and Treatment PlanningDokument5 Seiten1 - Patient Evaluation, Diagnosis and Treatment PlanningMohammed100% (1)
- Adverse Drug ReactionDokument15 SeitenAdverse Drug ReactionPuji Arifianti RamadhanyNoch keine Bewertungen
- Lacunar Infarct - Radiology Reference Article - RadiopaediaDokument8 SeitenLacunar Infarct - Radiology Reference Article - RadiopaediaRismanto TorsioNoch keine Bewertungen
- Animals Should Not Be Used As A Laboratory ToolsDokument6 SeitenAnimals Should Not Be Used As A Laboratory ToolsLuisa Castillo100% (1)
- 4 Ophthalmologists Cullman, AL: We Found NearDokument2 Seiten4 Ophthalmologists Cullman, AL: We Found NearSantosh Sharma VaranasiNoch keine Bewertungen
- Is It Okay To Drink Alcohol On Steroids - Google SearchDokument1 SeiteIs It Okay To Drink Alcohol On Steroids - Google SearchEsin SyurmeliNoch keine Bewertungen
- West African Journal of Medicine: Volume 40, Number 1 January 2023Dokument12 SeitenWest African Journal of Medicine: Volume 40, Number 1 January 2023ThankGod OgbonnaNoch keine Bewertungen
- CHN Finals ExamDokument10 SeitenCHN Finals ExamJhayneNoch keine Bewertungen
- Bates Physical Exam Video NotesDokument3 SeitenBates Physical Exam Video Notesdulcedeleche12359Noch keine Bewertungen
- Nutrition Month 2011: Isulong Ang Breastfeeding - Tama, Sapat at Eksklusibo! (Tsek) ProgramDokument22 SeitenNutrition Month 2011: Isulong Ang Breastfeeding - Tama, Sapat at Eksklusibo! (Tsek) Programセル ZhelNoch keine Bewertungen
- Medical Intensive Care UnitDokument120 SeitenMedical Intensive Care Unithaaronminalang100% (6)
- VTR 214 PDFDokument2 SeitenVTR 214 PDFKimberly AndrzejewskiNoch keine Bewertungen
- Ginjal Polikistik PDFDokument15 SeitenGinjal Polikistik PDFAgunkRestuMaulanaNoch keine Bewertungen
- Health and Family Welfare (C) Department: PreambleDokument14 SeitenHealth and Family Welfare (C) Department: PreambleAjish BenjaminNoch keine Bewertungen
- Fixation of Mandibular Fractures With 2.0 MM MiniplatesDokument7 SeitenFixation of Mandibular Fractures With 2.0 MM MiniplatesRajan KarmakarNoch keine Bewertungen
- 07 - NDP Diving Emergency Assistance Plan SampleDokument2 Seiten07 - NDP Diving Emergency Assistance Plan Sample12scribd123Noch keine Bewertungen
- Efficacy of Toltrazuril As A Metaphylactic and Therapeutic Treatment of Coccidiosis in First-Year Grazing CalvesDokument8 SeitenEfficacy of Toltrazuril As A Metaphylactic and Therapeutic Treatment of Coccidiosis in First-Year Grazing Calvesthanh ba matNoch keine Bewertungen
- Continue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFDokument21 SeitenContinue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFhengki jokteryNoch keine Bewertungen
- 傷寒論 Shang Han LunDokument3 Seiten傷寒論 Shang Han LunDave Mainenti97% (30)
- IMA Monthly Report Form JulyDokument4 SeitenIMA Monthly Report Form JulyInternetStudioNoch keine Bewertungen
- Critical Care Nurse Skills ChecklistDokument4 SeitenCritical Care Nurse Skills ChecklistMichael Silva0% (1)
- Allen Part Pedia CaseDokument3 SeitenAllen Part Pedia CasePaul Michael Baguhin0% (1)
- Case Study 5 (Respiratory) - COPDDokument6 SeitenCase Study 5 (Respiratory) - COPDSamantha AquinoNoch keine Bewertungen
- CotrimoxazoleDokument3 SeitenCotrimoxazolecsy123Noch keine Bewertungen
- NT To Look Better Than EVER This Summer? Why THIS Diet Plan Could Be The Answer (And You Can Still Eat Chocolate!)Dokument4 SeitenNT To Look Better Than EVER This Summer? Why THIS Diet Plan Could Be The Answer (And You Can Still Eat Chocolate!)dreeNoch keine Bewertungen
- Case Study Formate MSNDokument2 SeitenCase Study Formate MSNLijoNoch keine Bewertungen
- Priyanka Sen Final Practice School Internship ReportDokument35 SeitenPriyanka Sen Final Practice School Internship ReportThakur Aditya PratapNoch keine Bewertungen
- Massage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassageDokument1 SeiteMassage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassagenaveenNoch keine Bewertungen