Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Barack Obama (Wikipedia Biography)Dokument33 SeitenBarack Obama (Wikipedia Biography)politix100% (19)
- 2015 WFB End TimesDokument4 Seiten2015 WFB End TimesArt DeLauraNoch keine Bewertungen
- Lee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Dokument181 SeitenLee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Ralph Romulus FrondozaNoch keine Bewertungen
- A Fathers SonDokument5 SeitenA Fathers SonMariah PavleasNoch keine Bewertungen
- DH 0126Dokument6 SeitenDH 0126The Delphos HeraldNoch keine Bewertungen
- USMC Flags May20Dokument4 SeitenUSMC Flags May20U.S. Naval InstituteNoch keine Bewertungen
- Human Intelligence (HUMINT)Dokument74 SeitenHuman Intelligence (HUMINT)Anonymous kbmKQLe0J100% (1)
- Hecuba's MetamorphosisDokument18 SeitenHecuba's MetamorphosisTheophilos KyriakidesNoch keine Bewertungen
- Dodi 5240 10Dokument15 SeitenDodi 5240 10Robert ValeNoch keine Bewertungen
- Gutierrez, Francisco (2006) - Internal Conflict, Terrorism and Crime in ColombiaDokument14 SeitenGutierrez, Francisco (2006) - Internal Conflict, Terrorism and Crime in ColombiaMiguel Angel ReyesNoch keine Bewertungen
- English Atomic Bomb PaperDokument11 SeitenEnglish Atomic Bomb PaperDNoch keine Bewertungen
- East India Company ShowDokument19 SeitenEast India Company ShowrazwanNoch keine Bewertungen
- From The Great Convergence' To The First Great Divergence' - Roman and Qin-Han State Formation and Its AftermathDokument12 SeitenFrom The Great Convergence' To The First Great Divergence' - Roman and Qin-Han State Formation and Its Aftermathruryk_Noch keine Bewertungen
- Yasmin Fathina (Done)Dokument2 SeitenYasmin Fathina (Done)yannaNoch keine Bewertungen
- The Symbols of United KingdomDokument2 SeitenThe Symbols of United KingdomLegend9amaNoch keine Bewertungen
- The First Daily Test: Reading The Passage Carefully and Then Decide Whether Statements Are TRUE/ FALSE or NOT GIVENDokument3 SeitenThe First Daily Test: Reading The Passage Carefully and Then Decide Whether Statements Are TRUE/ FALSE or NOT GIVENVăn phú NguyễnNoch keine Bewertungen
- AD&D - Forgotten Realms - Dreams of The Red WizardsDokument74 SeitenAD&D - Forgotten Realms - Dreams of The Red Wizardsrushajshpk100% (17)
- Spiral View of TerrorismDokument10 SeitenSpiral View of TerrorismGabriela Gutierrez ValdovinosNoch keine Bewertungen
- Brief History of Global Market Integration in 20th CenturyDokument2 SeitenBrief History of Global Market Integration in 20th Centurymae Kuan100% (3)
- Cox, R. (2010) The Point Is Not Just To Explain The World But Change It (84-93)Dokument13 SeitenCox, R. (2010) The Point Is Not Just To Explain The World But Change It (84-93)Oscar Múnera PerafánNoch keine Bewertungen
- JzqoxdlgbdDokument348 SeitenJzqoxdlgbdflorin_nite2750Noch keine Bewertungen
- Rizal ExecutionDokument4 SeitenRizal ExecutionEstrabela Alexis Mae (Alexis Mae)Noch keine Bewertungen
- Title - Domo Wiki - FANDOM Powered by WikiaDokument16 SeitenTitle - Domo Wiki - FANDOM Powered by WikiaRizky Sunarya Adam AviannurNoch keine Bewertungen
- Connect Verbs Definition.: Each Below CorrectDokument2 SeitenConnect Verbs Definition.: Each Below CorrectRita SousaNoch keine Bewertungen
- Vietnam War Memorial - FinalDokument7 SeitenVietnam War Memorial - FinalShefali DeoNoch keine Bewertungen
- Athena (Lecture Slides 8) Pallas Athena (Minerva) : IntroDokument4 SeitenAthena (Lecture Slides 8) Pallas Athena (Minerva) : IntroJeonghun LeeNoch keine Bewertungen
- BSAA Remote DesktopDokument35 SeitenBSAA Remote DesktopStefan MarshNoch keine Bewertungen
- Angel Reaction PaperDokument2 SeitenAngel Reaction PaperAngel Hiwatig IINoch keine Bewertungen
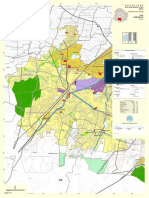
- 3.21 Map (A) - AnjanapuraDokument1 Seite3.21 Map (A) - Anjanapuramohan krishna ramegowdaNoch keine Bewertungen
- North American Aerospace Defense CommandDokument7 SeitenNorth American Aerospace Defense CommandAryan KhannaNoch keine Bewertungen