Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Patient Encounter FormDokument2 SeitenPatient Encounter FormSpectator Medic0% (1)
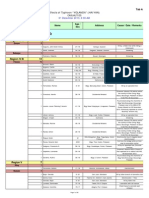
- List of Casualties Due To Typhoon YolandaDokument31 SeitenList of Casualties Due To Typhoon YolandaSunStar Philippine NewsNoch keine Bewertungen
- Current Concepts On Meniscal Repairs, SrimongkolpitakDokument12 SeitenCurrent Concepts On Meniscal Repairs, SrimongkolpitakAlhoi lesley davidsonNoch keine Bewertungen
- Done-EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocol-1Dokument18 SeitenDone-EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocol-1Mary Gloriscislle M. JoreNoch keine Bewertungen
- Penanganan Trauma Muskuloskeletal Dan ImobilisasiDokument54 SeitenPenanganan Trauma Muskuloskeletal Dan Imobilisasiamir hamzahNoch keine Bewertungen
- Reten Modern Dressing 2023 PKDMTDokument51 SeitenReten Modern Dressing 2023 PKDMTMasros TukiranNoch keine Bewertungen
- Head Trauma - Dr. Affan Priyambodo, SPBS (K)Dokument32 SeitenHead Trauma - Dr. Affan Priyambodo, SPBS (K)Verty SalleNoch keine Bewertungen
- Classification of Fractures - BasicDokument19 SeitenClassification of Fractures - BasicAdeel HashmiNoch keine Bewertungen
- CHAPTER 48 - Skin Integrity & Wound CareDokument3 SeitenCHAPTER 48 - Skin Integrity & Wound CareANoch keine Bewertungen
- Pe SubjectDokument3 SeitenPe SubjectAkira EnriquezNoch keine Bewertungen
- Sprains and StrainsDokument7 SeitenSprains and StrainsNitin RaizadaNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaibnusinaNoch keine Bewertungen
- Sports Injury StatisticsDokument2 SeitenSports Injury StatisticsJeffrey EscauriagaNoch keine Bewertungen
- Advanced Management of TBI - Dr. Farhad, SPBSDokument40 SeitenAdvanced Management of TBI - Dr. Farhad, SPBSHanifan NugrahaNoch keine Bewertungen
- Qru3063 A211 Group: 3 Project Title: Rilia Thinking Template For PBL Activities Relevant Information Learning Issues Inquiry ActivitiesDokument2 SeitenQru3063 A211 Group: 3 Project Title: Rilia Thinking Template For PBL Activities Relevant Information Learning Issues Inquiry ActivitiesIzzati AzmiNoch keine Bewertungen
- S.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Dokument47 SeitenS.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Chrysi TsiouriNoch keine Bewertungen
- SMF Orthopaedi Dan Traumatologi RSU DR Saiful Anwar Malang: Thomas Erwin C J HuwaeDokument58 SeitenSMF Orthopaedi Dan Traumatologi RSU DR Saiful Anwar Malang: Thomas Erwin C J Huwaeyulia manaweanNoch keine Bewertungen
- Basic Fracture ManagementDokument107 SeitenBasic Fracture ManagementPrabath ChinthakaNoch keine Bewertungen
- Robert Chasowa Was Assaulted - AutopsyDokument2 SeitenRobert Chasowa Was Assaulted - AutopsyMalawi2014Noch keine Bewertungen
- Blunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature ReviewDokument13 SeitenBlunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature Revieworalposter PIPKRA2023Noch keine Bewertungen
- Laporan Emergency 2 FebDokument8 SeitenLaporan Emergency 2 FebbisturisevenNoch keine Bewertungen
- Acute Mild Traumatic Brain Injury (Concussion) in Adults - UpToDateDokument22 SeitenAcute Mild Traumatic Brain Injury (Concussion) in Adults - UpToDateZulvina FaozanudinNoch keine Bewertungen
- Pathophysiology of Head TraumaDokument2 SeitenPathophysiology of Head TraumaGrace Jane Dionaldo100% (1)
- ORT038 Advice After Breaking Your ClavicleDokument3 SeitenORT038 Advice After Breaking Your ClavicleFelix FrancisNoch keine Bewertungen
- Proximal Humerus FracturesDokument4 SeitenProximal Humerus FracturesParidhi MittalNoch keine Bewertungen
- Cdi-2 Quiz 1 MidDokument5 SeitenCdi-2 Quiz 1 Midangelo macalongNoch keine Bewertungen
- Common Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCDokument67 SeitenCommon Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCPrince EdwardNoch keine Bewertungen
- Fix Me I'm Broken (On First Aid)Dokument21 SeitenFix Me I'm Broken (On First Aid)Romar LagunaNoch keine Bewertungen
- First Aid For Sprain and StrainsDokument9 SeitenFirst Aid For Sprain and StrainsKristine May Pangandian MagnoNoch keine Bewertungen
- Lingering InjuriesDokument12 SeitenLingering Injuriessunrei musicNoch keine Bewertungen