Beruflich Dokumente
Kultur Dokumente
9
Hochgeladen von
Ionela NeacsuOriginalbeschreibung:
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
9
Hochgeladen von
Ionela NeacsuCopyright:
Verfügbare Formate
Pharmacological Research 62 (2010) 9099
Contents lists available at ScienceDirect
Pharmacological Research
journal homepage: www.elsevier.com/locate/yphrs
Review
Targeting nanoparticles to cancer
M. Wang a , M. Thanou a,b,
a b
Imperial College London, Department of Chemistry, United Kingdom Kings College London Pharmaceutical Sciences Division, United Kingdom
a r t i c l e
i n f o
a b s t r a c t
Nanotechnology applications in medicine, termed as nanomedicine, have introduced a number of nanoparticles of variable chemistry and architecture for cancer imaging and treatment. Nanotechnology involves engineering multifunctional devices with dimensions at the nanoscale, similar dimensions as those of large biological vesicles or molecules in our body. These devices typically have features just tens to hundred nanometers across and they can carry one or two detection signals and/or therapeutic cargo(s). One unique class of nanoparticles is designed to do both, providing this way the theragnostic nanoparticles (therapy and diagnosis). Being inspired by physiologically existing nanomachines, nanoparticles are designed to safely reach their target and specically release their cargo at the site of the disease, this way increasing the drugs tissue bioavailability. Nanoparticles have the advantage of targeting cancer by simply being accumulated and entrapped in tumours (passive targeting). The phenomenon is called the enhanced permeation and retention effect, caused by leaky angiogenetic vessels and poor lymphatic drainage and has been used to explain why macromolecules and nanoparticles are found at higher ratios in tumours compared to normal tissues. Although accumulation in tumours is observed cell uptake and intracellular drug release have been questioned. Polyethyleneglycol (PEG) is used to protect the nanoparticles from the Reticulo-Endothelial System (RES), however, it prevents cell uptake and the required intracellular drug release. Grafting biorecognition molecules (ligands) onto the nanoparticles refers to active targeting and aims to increase specic cell uptake. Nanoparticles bearing these ligands are recognised by cell surface receptors and this leads to receptor-mediated endocytosis. Several materials are suggested for the design of nanoparticles for cancer. Polymers, linear and dendrimers, are associated with the drug in a covalent or non-covalent way and have been used with or without a targeting ligand. Stealth liposomes are suggested to carry the drug in the aqueous core, and they are usually decorated by recognition molecules, being widely studied and applied. Inorganic nanoparticles such as gold and iron oxide are usually coupled to the drug, PEG and the targeting ligand. It appears that the PEG coating and ligand decoration are common constituents in most types of nanoparticles for cancer. There are several examples of successful cancer diagnostic and therapeutic nanoparticles and many of them have rapidly moved to clinical trials. Nevertheless there is still a room for optimisation in the area of the nanoparticle kinetics such as improving their plasma circulation and tumour bioavailability and understanding the effect of targeting ligands on their efciency to treat cancer. The need to develop novel and efcient ligands has never been greater, and the use of proper conjugation chemistry is mandatory. 2010 Elsevier Ltd. All rights reserved.
Article history: Received 24 January 2010 Received in revised form 18 March 2010 Accepted 19 March 2010 Keywords: Nanoparticles Cancer Nanomedicine Nanooncology
Contents 1. 2. 3. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . FDA-approved therapeutic nanoparticles for cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.1. Cancer nanoparticles types, functionalities and modalities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Nanoparticle surface constituents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1. Nanoparticle biological stability stealth polymers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.2. Nanoparticle cancer recognition-targeting ligands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Summary and future perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91 91 92 93 93 94 97 97
4.
Corresponding author at: 150 stamford st, London, United Kingdom. E-mail address: maya.thanou@kcl.ac.uk (M. Thanou). 1043-6618/$ see front matter 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.phrs.2010.03.005
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
91
1. Introduction Nanomedicine, the application of nanotechnology to medicine, aims to overcome problems, related to diseases, at the nanoscale where most of the biological molecules exist and operate. Particularly nanotechnology application to cancer aims to bring signicant breakthroughs in diagnosis, treatment and monitoring of cancer. Nanoparticles which are molecular assemblies of functional chemistries will be able to overcome biological barriers (bio-barriers), accumulate preferentially in tumours and specically recognise single cancer cells for detection and treatment. Today, there is a strong focus on nanotechnology application to cancer. Cancer Nanotechnology is a new eld of interdisciplinary research cutting across biology, chemistry, engineering and medicine aiming to lead major advances in cancer detection diagnosis and treatment [14]. The eld has received strong support especially in US where several centres for nanotechnology for cancer have been launched and are operating since 2004. There is no better denition and overview of this eld, other than the one given in http://nano.cancer.gov/, which is termed as the NCI (National Cancer Institute, US) alliance for nanotechnology for cancer. This alliance aims to bring several teams together in a surprisingly multidisciplinary approach to explore solutions for cancer detection imaging and diagnosis [5]. In Europe a number of academic groups focus on research in this eld. However it is only until recently Europe FPVII programs have announced calls for multidisciplinary team projects in nanomedicine for cancer. In the UK the major cancer research organisation (Cancer Research, UK) appears hesitant on supporting the eld, possibly due to potential risks of non-tested nanomaterials. In a recent report Roadmaps in Nanomedicine towards 2020 from Nanomedicine European technology platform (http://www.etp-nanomedicine.eu/public) specialists foresee that oncology imaging and therapy will be the main area of application of various designers type of Nanoparticles. The targeted therapies in oncology are predicted as a 30bn D global market in 2015. The opportunity lies in the fact that for the rst time we are able to tackle cancer management needs and individualise therapies by developing personalised treatments. Ideally, a clinical lab will be using nanotechnology based assays and detect tumour markers of each patient while at the same time scientists from this lab will formulate the nanoparticles using the same biomarkers as the ones found in the patients tumour, carrying the specic genetic drug (i.e. siRNA) designed to knock down the biomarker protein related to that tumour. Cancer biomarkers include a variety of molecules such as mutant genes, RNAs, proteins, lipids, carbohydrate and small metabolite molecules. Their altered presentation or expression is related to a biological change (expressed as neoplasia) and a clinical outcome. Molecular proling studies can discover cancer biomarkers based on the relation between a molecular signature and cancer behaviour. By dening the interrelationships among these cancer biomarkers it could be possible to diagnose the patients cancer molecular prole, leading to personalised and predictive medicine [3]. A unique molecular prole can be used to predict the tumours invasive characteristics and metastatic potential. Molecular proling was rst reported by Golub et al. [6] who showed that gene expression patterns could classify tumours, providing information on the stage, grade, clinical course and response to treatment. Gene expression can demonstrate that the molecular signature of each metastatic tumour is a result of the combined tumoural, stromal, and inammatory factors of the original heterogeneous tumour [7,8]. Further, cancer molecular proling can combine cDNA microarrays with tissue microarrays for biomarker discovery and tissue immunohistochemical validation [9].
The identication of such biomarkers is very important for individualised therapy and treatment of cancer [10,11]. For example Herceptin is a monoclonal antibody targeting amplied and over-expressed Erbb2 (HER2) is a tyrosin kinase receptor found in 2530% of breast cancers. In the process of drug approval, the FDA required diagnostic tests to detect HER2 over-expression indicating that individualised therapy for cancer is required to achieve cancer treatment without the unwanted effects. In vitro diagnostics for HER 2 now include an immunohistochemistry assay and a nucleic acid uorescence in situ hybridisation (FISH) test to guide Herceptin treatment decisions. The design of methods that can detect in vivo the expression of such markers and monitor them during treatment is a real challenge. For the rst time nanotechnology can be applied for the design of multifunctional nanoparticles that will be able to (a) detect, (b) image tumours and their metastases, (c) treat and (d) monitor treatment progression. The application and efciency of these nanoparticles in vivo will help enormously the pre- and post-operative cancer treatment. The design of such nanoparticles is not trivial as several factors have to be taken into consideration. Primarily, the chemistry of the core and the layers needs to be done with consideration of the structural integrity and stability of the particles in biological uids. Further, similar to the process of product drug development, nanoparticle development needs to consider physicochemical issues related to the properties of the nanoparticles, biopharmaceutical issues related to the properties of the biobarriers and pharmacological issues related to the site, time and duration of nanoparticles action. These nanoparticles have to be considered differently to small and large molecular drugs introducing novel parameters for their design. FDA states that ADME (Administration, Distribution, Metabolism and Excretion) studies need to be redesigned in the case of nanoparticles to take under consideration their aggregation and surface chemical characteristics [12]. Most nanoparticles are expected to accumulate in tumours due to the enhanced permeation and retention (EPR) effecta tumour characteristic that was identied by Maeda as a means to target anticancer agents to tumours [13]. Nanoparticle tumouraccumulation is deemed possible due to the highly permeable blood vessels of the tumours as a result of rapid and defected angiogenesis. In addition tumours are characterised by dysfunctional lymphatic drainage that helps the retention of nanoparticles in tumour long enough to allow local nanoparticle disintegration and release of the drug in the vicinity of tumour cells. The phenomenon has been used widely to explain the efciency of nanoparticle and macromolecular drug accumulation in tumours [14]. Our knowledge of nanoparticle biokinetics, metabolism and clearance is poor as very few nanoparticle products have been clinically tested. Doxil and Abraxane are two nanoparticles for cancer therapy that have gone through preclinical and clinical evaluation and FDA approval. Doxil is a liposomal system for doxorubicin delivery and treatment of ovarian carcinoma and Abraxane is an albumin nanoparticle taxol conjugate for the treatment of metastatic breast cancer. 2. FDA-approved therapeutic nanoparticles for cancer The rst nanoparticles used to deliver cancer chemotherapy were the liposomes. Liposomes are usually sized at the nanoscale and consist of a lipid bilayer surrounding a water core hosting the drug. The rst studies to report the efciency of liposomes as nanoparticles focused on the improvement of pharmacokinetics and biodistribution of the anthracycline drug doxorubicin. The nature of doxorubicin, unfortunately also induces cardiotoxicity and this can limit the administered dose. To avoid this, doxorubicin was encapsulated in anionic liposomes, after which studies
92
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
showed that liposomal doxorubicin improved accumulation in tumours and had increased antitumour activity while cardiotoxicity was diminished [15,16]. Liposomal doxorubicin has been shown to be safe and efcient clinically, in ovarian and breast cancer [17,18]. Doxil , the pegylated liposomal doxorubicin shows high efciency due to improved pharmacokinetics as it has been shown to escape the reticulo-endothelial system (RES)an important barrier in nanoparticle systemic circulation [1921]. Polyethyeleneglycol (PEG) is used with a number of nanoparticles as it improves colloidal stability and prevents uptake by the RES. PEG is usually added on the surface of nanoparticles to create the socalled steric stabilisation effect where the PEG molecules form a protective hydrophilic layer on the surface of nanoparticles that prevents interaction with each other (aggregation) and with blood components. As a result, grafting of PEG on the surface of nanoparticles reduces uptake by the macrophages of the mononuclear phagocyte system (MPS) and prolongs the blood circulation times [22,23]. The second nanoparticle approved for cancer therapy was an albumin Taxol conjugate. Abraxane was designed to overcome Taxol insolubility related issues, through binding of the drug to 130 nm albumin nanoparticles. Also known as nab-paclitaxel, Abraxane was designed to avoid the use of Cremophor EL solvent (polyethoxylated castor oil) that is used to solubilise Taxol [2426] and is the rst albumin nanoparticle approved for human use by FDA. Albumin is a natural carrier of endogenous hydrophobic molecules which are bound onto it through non-covalent interactions, a type of binding interaction that is critical for pharmacokinetics (protein binding). More importantly, albumin assists endothelial trancytosis of protein bound and unbound plasma constituents principally through binding to a cell surface, a 60-kDA glycoprotein receptor gp60. The receptor then binds to caveolin1 with subsequent formation of trancytotic vesicles (caveolae) [27]. In addition, albumin binds onto osteonectin, secreted protein acid rich in cystein (SPARC) which is present on breast lung and prostate cancer and that way albumin is accumulated in tumours [26,28]. Currently there are more than 50 clinical trials ongoing using nanoparticles for cancer. The majority of these nanoparticles are nab type (nanoparticle albumin bound) tested for the treatment of various cancer types (http://clinicaltrials.gov; search for nanoparticles and cancer on December 2009). The clinical trials also include a nanoliposomal irrinotecan [29], a SPIO (superparamagnetic iron oxide) to diagnose pre-operative stage of pancreatic cancer [30] a transferin targeted cyclodextrin polymer based nanoparticle for siRNA delivery CALAA-01 [31]. Importantly the clinical trials include studies of designed nanoparticles such as the lyso-thermosensitive liposomal doxorubicin (Thermodox ) as a novel activated therapy using radiofrequency ablation [32,33]. 2.1. Cancer nanoparticles types, functionalities and modalities During the last years a number of studies have been presented that show smartly designed nanoparticles for tumour targeting, imaging and therapy where reviews have attempted to describe and categorise these nanoparticles [3441]. Most of the researchers agree that nanocarriers or nanovectors are nanosized materials that can carry multiple drugs and/or imaging agents [1,34]. Particularly, they consist of a scaffold (polymer or lipids), where drugs and contrast agents are attached, a corona of polymeric material that improves biokinetics and biodistribution and a ligand that adds specicity for cancer biomarker molecular recognition and attachment to cancer cells [3436,42]. Therapeutic nanoparticles with a highly dened lipid scaffold are mainly the liposomes, discovered 40 years ago by Bangham [43,44]. Liposomes size is ranging from a minimal diameter of
30 nm to several microns [45]. Liposomes may vary in size, lipid composition, method of preparation and particularly surface chemistry. Liposomes have evolved through the years to a versatile carrier adapted each time to have a different functionality and serve a certain drug delivery purpose [46,47]. A progressing type of lipid based nanoparticle emerging in the therapeutic eld is the Solid Lipid nanoparticles (SLN). Since their rst description by Mller et al. [48,49] SLNs have attracted increasing attention as an efcient and non-toxic alternative to lipophilic colloidal drug carrier prepared either with physiological lipids or lipid molecules used as common pharmaceutical excipients. Two production techniques have been reported: the high-pressure homogenisation described by Mller and Lucks and the microemulsion-based technique by Gasco [49,50]. In contrast to the preparation method of most polymeric microsphere and nanoparticle systems, SLN production techniques do not need to employ potentially toxic organic solvents, which may also have deleterious effect on protein drugs. Furthermore, under optimised conditions they can be produced to carry lipophilic or hydrophilic drugs and seem to full the requirements for an optimum particulate carrier system. Their colloidal dimensions and their controlled release behaviour enable drug protection through administration by parenteral and non-parenteral routes thus emphasising the versatility of this nanoparticulate carrier [51,52]. Dendrimers are the main polymeric architectures that follow in the category of nanoparticles. They are a unique class of repeatedly branched polymeric macromolecules with a nearly perfect 3D geometric pattern. They can be synthesised with either divergent methods (outward from the core) or convergent methods (inward towards the core). Tomalia was the rst to synthesise the 3D PAMAM (polyamidoamine) dendrimers using divergent methods [53]. These dendrimers contain tertiary amines that allow the binding of a number of molecules. The method of convergent dendrimer synthesis has been established by Frechet [54] and a dendrimer is characterised by the generation of monomers (G) added to a main core. The size of these dendrimers varies between 1.9 nm for G1 and 4.4 nm for G4, dendrimers, being the smallest nanocarriers developed which has promoted their suggestion for a number of pharmaceutical applications [55]. They have been extensively studied in the area of therapeutics and diagnostics for cancer [56] as well as for photodynamic therapy (activation therapies) [56], boron neutron capture therapy [57] and hyperthermia therapies using gold nanoparticles [58]. Dendrimers are versatile particles regarding their size and functionality and their chemistry allows for several modications for certain imaging modalities. Gadolinium has been complexed with dendrimers and it was found that this complex enhanced conventional MR images in a dendrimer molecular weight dependent way and substantially better, compared with conventional diethylenetriaminepentaacetic acid Gd (III) chelates [59]. As drug delivery agents, dendrimers can carry drugs as complexes or as conjugates although one limitation lies in the effort of controlling the rate of drug release. The encapsulated, complexed, drugs tend to be released rapidly (before reaching the target site) and in the dendrimerdrug conjugates, it is the chemical linkage that controls the drug release. However, dendrimers offer several advantages as drug carriers targeting cancer. One major advantage is their surface functionality providing the selective coupling of imaging agents, targeting ligands and/or other components to increase tumour specicity. The abovementioned nanoparticles either based on lipids or on polymers are generally soft and exible nanoparticles. Their size ranges from 30 nm to slightly more than 100 nm. However, they can penetrate biological membranes due to their exibility and biophysical interaction with cellular membrane components.
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
93
The inorganic nanoparticles represent a different class of nanoparticles that are usually much smaller, 540 nm and they do not have the exibility observed in liposomes and polymeric nanoparticles. Inorganic nanoparticles have made their appearance in cancer therapy during the last decades in a number of applications [60]. The main type of inorganic nanoparticlesthe iron oxide nanoparticles, has been used for imaging tumours [61]. The main advantage of magnetic nanoparticles is their ability to be visualised by Magnetic Resonance (MR) imaging. Additionally, iron oxide nanoparticles can be guided to target sites (i.e. tumour) using external magnetic eld and they can be also heated to provide hypethermia for cancer therapy [62]. Yu et al. reported thermally cross-linked superparamagnetic iron oxide nanoparticles that could carry a Cy5.5 near infra-red probe (dual imaging) and doxorubicin for the imaging and treatment of cancer. The nanoparticles substantially diminished tumour size and provided the proof of concept that they can combine several modalities for maximum antitumour effect [62]. Magnetic nanoparticles have been used in the development of dual purpose probes for the in vivo transfection of siRNA [63,64]. The iron nanoparticles used in that study delivered siRNA at the same time as imaging their own accumulation in tumour sites. The iron nanoparticles used, were coated with dextran on which Cy5.5 and siRNA were chemically coupled [64]. Dextran coated iron oxide nanoparticles are already in clinical practice. Ferumoxtran-10 is a commercially available ultrasmall superparamagnetic iron oxide particle (USPIO) product [65,66]. After i.v. injection the particles collect in lymph nodes, liver, spleen, or brain tissue where they can be seen using MRI. In a lymph node with proper architecture and function (healthy) macrophages take up a substantial amount of Ferumoxtran-10. This uptake results in a marked reduction in signal intensity and turns the lymph nodes dark when seen by MRI. Inltration of lymph nodes with malignant cells replaces the macrophages and changes the architecture of the lymph nodes. In malignant lymph nodes there is no ferumoxtran-10 macrophage uptake and they can retain the high signal intensity or display heterogeneous signal intensity if micrometastases are involved. This way the grade of tumours and prognosis can be assessed as micrometastases are important for this assessment [67]. Gold nanoparticles appear as another type of inorganic metal particle used in targeting tumours. Metal nanoshells are a class of nanoparticles with tunable optical resonances. Metal nanoshells consist of a spherical dielectric core nanoparticle, in this case silica, which is surrounded by a thin metal shell, such as gold [68]. These particles possess a highly tunable plasmon resonance, a resonant phenomenon whereby light induces collective oscillations of conductive metal electrons at the nanoshell surface. When studied in vivo in mice the nanoshells were stealthed with PEG, systemically injected, and were shown to accumulate preferably at the tumour site due to the highly permeable, poorly organized vascular networks common in neo-plastic tumours. Then, NIR (Near Infra-red) laser treatment of the bulk tissue selectively heats and destroys the nanoshell-laden tumour regions within the tissue, while leaving surrounding tissue intact [69]. Nanoshells are currently evaluated in a number of clinical settings after a 5-year period of intensive preclinical development [70]. Such development of nanoshells included the combination of nanoshells with cancer antibodies. Anti-HER2 antibody was conjugated onto nanoshells providing the potential of combining antibody therapy with imaging and hyperthermia [71]. As gold nanoparticles have evolved other gold structures have also been suggested. Nanorods, with the appropriate PEG stealth layer, are being developed as an improved means of hyperthermia. After injection in xenograft bearing mice, aided by computational studies, nanorods were shown to eradicate all irradiated tumours.
The nanorods were compared to nanoshells for their laser induced heat. It was found that the PEG-Nanorods solutions exhibited heat that was generated 6 times faster compared to the heat generated by nanoshells under the same conditions [72]. Overall, during the last decade nanoparticles for in vivo application targeting cancer appeared with different sizes structures and tuneable properties. However, there are 2 functional components that are required for their biological applications for cancer targeting: The stealth layer and the ligand for cancer receptors. 3. Nanoparticle surface constituents PEG layers are added onto any nanoparticle that is aimed to be administered intravenously for accumulation into tumours. Whether this is a liposome, a dendrimer or an inorganic nanoparticle such a layer (corona or halo) provides long circulation as it inhibits the accumulation of opsonins and their uptake by the macrophages. Although, currently there are no clear rules regarding the organization and the type of PEG on the surface of nanoparticles, there are some trends, derived from the extensive work on liposomes for cancer targeting. These trends indicate that the PEGs size and density on the nanoparticles are key features that will control the circulation times and accumulation in tumours. Such PEG layers can interfere with targeting ligands and inhibit them from interaction with the corresponding receptors. In the following two sections PEG and cancer targeting ligands will be discussed with emphasis on liposomes as these nanoparticles have been widely studied in vivo in tumour animal models. 3.1. Nanoparticle biological stability stealth polymers Most nanoparticles require colloidal stability in vitro (in buffers i.e. for storage) and in vivo (biological stability). A protective layer can therefore be formed by the incorporation of a hydrophilic polymer layer. The FDA-approved PEG polymer is the mostly used material. PEG is commonly adopted for the stealth function, due to their enhanced hydrophilicity and exibility [73]. PEG enhances the nanoparticles lifetime in circulation, by preventing their interaction with plasma proteins [7477]. Particularly for liposomal nanoparticle systems their protective PEG layer can be achieved through different methods. The main technique is the inclusion of PEG-lipid conjugates (Fig. 1) into the lipid lm of the liposomal formulation. Upon hydration, the liposomes are formed with PEG polymers exposed on the surfaces [78]. The other techniques are based on the formation of the liposomal platform before the addition of PEG polymers. The method of post-conjugation, includes the covalent attachment of functionalised PEG to the pre-formed nanoparticles. Post-insertion, on the other hand, is performed by incubating the pre-formed liposomes with PEG-lipid conjugates in aqueous solution [79]. The amphiphilic nature of the PEG-lipids renders them into micellar structures, and their insertion into liposomal surfaces is perceived as a method of relieving micellar strain. However, the method of preparation, the conguration and the effect of the PEG layer is dependent on the PEG chain length and their surface densities. The effect of such a layer depends on its optimisation of the organisation of the PEG chains [8083]. Although the inclusion of PEG onto liposomal surfaces improves their efciencies for transport to the tumour sites, it is important to remember that their presence may hinder their binding to and uptake by cancer cells. The incorporated PEG-lipid conjugates need to be able to render steric stability of the nanoparticles and be able to prevent surface adsorption of opsonin proteins. Higher coverage of liposomal surfaces is achieved by introducing higher densities of PEG-lipids in liposomal systems [84]. However, in the case of liposomes, there is
94
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
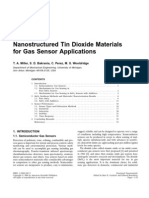
Fig. 1. Structures of PEG-lipid conjugates used in preparing stealth liposomes. Both lipids shown are formed with a PEG chain of 45 monomers, correlating to a molecular weight of approximately 2000 Da. PEG units in both lipids are capped at the distal end with a methoxy group, and conjugated to a DSPE lipid (a), or a DPPE lipid (b).
a maximum molar percentage of the PEG-lipids that can be incorporated into the lipid formulation before they become detrimental to systemic delivery. A liposomal membrane is held together by non-covalent interactions, therefore the PEG-lipid conjugates are susceptible to dissociation from the liposomes if the PEG density is sub-optimal. When presented on a liposomal surface, individual PEG chains exhibit a Flory dimension, Rf, which represents the volume that each exible PEG cloud occupies. Longer polymer chains have larger Rf, although studies have shown that the PEG density on a liposome surface is more important that the size of the polymer [85]. The Rf of a PEG2000 chain is approximately 5.6 nm, and in conjunction with grafting density, affects the resultant conformation of the PEG chains. Increasing the amount of PEG-lipids within a liposomal formulation increases the PEG density, which ultimately reduces the distance, D, between each PEG molecule on the nanoparticle surface. When D > Rf, the PEG chains will self-assemble into a random-coil like mushroom cloud. When D < Rf, the lateral pressure between the overcrowded PEG mushroom clouds will force the extension of the PEG chains into a brush conformation (Fig. 2) [86]. The brush regime results from the increased lateral pressure between the PEG chains, which forces the extension of the polymers away from the surface, into more linear conformations. What prolongs a nanoparticles retention time in circulation is its ability to avoid interaction with plasma proteins [87]. The arrangement of surface PEGs into brush congurations generates greater protein repulsion, and generally enhances a liposomes lifetime in circulation [8890]. Another phenomenon related to protein adsorption is the recognition of PEGylated liposomes by
anti-PEG antibodies [9193]. This effect has been reported to occur between 2 and 4 days after the rst administration of PEGliposomes, and leads to the event of accelerated blood clearance of further PEG-liposomes administered at repeat doses [9496]. There are yet no data on other pegylated nanoparticles induced PEGantibodies and such phenomenon should be critically investigated in the preclinical development of nanoparticles. What is left is therefore the optimisation of a delivery system with an optimal amount of PEG-lipids, where too little does not provide enough coverage to evade protein adsorption, and too much results in removal of the PEG-lipids. Inorganic nanoparticles require different methods of coating or introducing the biocompatibility and colloidal stability layers. Generally this is performed by the co-precipitation of the particles with various types of polymers or cross-linked polymers [97] a technique that can improve the particle monodispersity, an important parameter regarding their biological applications. Dextran, albumin and PEG (Mw 5000) are all types of molecules that have been studies as coating materials for providing biocompatibility to iron oxide nanoparticles [98]. PEG with a Mw of 5000 was added as a coating layer on iron oxide nanoparticles to improve biocompatibility [99]. Gold nanoparticles provide a more suitable surface for PEGgrafting. ThiolPEG or bifunctional PEG can be added on the surface to provide colloidally stable and biocompatible gold nanoparticles [100]. Sulfydrylated PEG has been added to gold nanoparticles to provide 38 nm nanoparticle that gave a bloodpool contrast agent for tumour vascular structures [101]. Recently, PEG bidentate ligands (PEG-thioctic acid and PEG-dihydrolipoic acid) were introduced onto quantum dots and gold nanoparticles to provide substantially improved stability in biological media [102]. In contrast to liposome based nanoparticles inorganic nanoparticles form much smaller structures even when coated with a biocompatibility layer. It is still unknown the effect of the PEG size and grafting density on all nanoparticle kinetics and accumulation in tumours. For liposomes some studies have indicated the important role of PEG, however there is minimum work done on the role of PEG on the kinetics of inorganic nanoparticles. Further dendrimers and biodegradable polymers Pegylation is too variable to observe trends. On biodegradable polymer nanoparticles PEG is introduced as part of the copolymer and in most cases a micelle is formed [103]. 3.2. Nanoparticle cancer recognition-targeting ligands
Fig. 2. Representation of different PEG conformations, formed through their incorporation onto surfaces at different densities. When the distance between the PEG-lipids, D, is greater than the Flory diameter of the PEG (D > Rf), the polymer will collapse into a mushroom conguration. When D < Rf, the PEG chains will be extended from the surface to form a brush-like conformation.
The addition of a targeting moiety onto the surface of nanoparticles (Fig. 3) aims to increase selective cellular binding and internalisation through receptor-mediated endocytosis. Without the incorporation of targeting ligands, nanoparticles rely on non-
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
95
Fig. 3. Representation of targeted and non-targeted liposomal nanoparticle systems. The targeted nanoparticles are functionalised with an outer layer of receptor-specic ligands, which can be of an antibody (full or fragment), small molecule, Antibody peptide or aptamer. The aqueous core of the liposomal nanoparticle can contain hydrophilic drugs, such as doxorubicin, or nucleic acids, such as DNA or siRNA.
specic interactions with cell membranes, which can be low when covered in a layer of PEG polymers. The targeting effect of the surface ligands is dependent not only on the nature of the ligand itself, but also on a variety of factors that require cooperative optimisation. Discussed in this section are examples of ligand-targeted nanoparticle systems with emphasis on liposomes. These examples differ from each other in many ways, including liposomal lipid content, type of ligand, method of ligand loading, degree of PEGylation and ligand density. With attention to the physical and biological effects of differently prepared nanoparticles, patterns that lead to enhanced drug delivery to cancers, through the effect of targeting ligands, can be derived. One challenge of targeting cancers and tumours is that the defective cells are often very similar in characteristics to its surrounding healthy tissue. To differentiate such cells, the ligands can be designed to have specicity for receptors that are overexpressed on cancerous cells, but are normally or minimally expressed on normal, healthy cells. These molecules should have high afnity to their cognate receptors, plus have innate abilities to induce receptor-mediated endocytosis. The targeting layer poses as the outmost exterior of the nanoparticle delivery system, where targeting ligands are generally presented on top of the stealth layer [104]. Structures such as antibodies, antibody fragments, proteins, small molecules, aptamers and peptides have all demonstrated abilities to induce nanoparticle-targeting to cancer cells. Antibodies against the HER-2 receptor, the transferrin receptor (TfR) and the prostate specic antigen receptor are both common examples of receptor targets, due to their over-expression of such receptors on cancer cells [105108]. These antibodies generally exhibit strong interactions with corresponding receptors, with dissociation constants in the nanomolar range. Antibody fragments, consisting of only the Fab binding regions, have also been studied as targeting ligands [109,110]. The advantages of such structures is that they are smaller, and do not contain the Fc region of the antibody which can induce immunogenicity and antigenicity when present on liposome surfaces [111113]. Like antibodies and antibody fragments, the use of whole proteins is also commonly considered as targeting ligands for their increased afnity for target receptors. For example, the natural ligand for TfR, transferrin, binds to its receptor with a dissociation constant of around Kd = 40 nM. On overcoming systemic barriers to arrive in tumour vicinities, targeted liposomes have greater opportunities for binding to cancer cells if the ligand has naturally high afnities for the corresponding receptor. Another protein that has shown potential for cancer targeting is the urokinase plasminogen activator, uPA, a natural ligand for the urokinase plasminogen activator receptor. Examples have used protein fragments, containing only the binding region of uPA for targeting the over-expressed receptors on colon cancers and breast cancers [114].
Peptide sequences pose as even shorter and smaller versions of antibody and protein fragments. Derived from phage display assays and X-ray crystallography studies, short peptide sequences with receptor-specicity have also been used for nanoparticle-targeting. For uPAR, peptides such as the U11 peptide were identied from examination of the binding region of uPA [115,116]. Our work has focused on promoting this peptide for targeting prostate and breast cancer cells [117]. Another prominent example of peptide ligands is the RGD peptide (Fig. 4), identied through phage display to have high afnity to 5 3 integrin receptors over-expressed on angiogenic vasculatures [118120]. Other types of shorter ligands include small molecules such as anisamide, a ligand for sigma receptors over-expressed on lung cancer cells [121,122], and folic acid (Fig. 4), specic for the folate receptors on ovarian cells [123125], are more examples of targeting moieties for nanoparticle-targeting. Ligands chosen for receptor-targeting should have the function of inducing receptor-mediated endocytosis. Depending on the type of ligandreceptor interaction, the rate of cellular internalisation would differ. This is an important factor as rates of internalisation could affect the accumulation of nanoparticle in tumour sites. Some ligand species, such as folate, have been shown to have
Fig. 4. Structures of ligands commonly used to functionalize nanoparticle surfaces, for inducing their specicity and internalisation characteristics to cancer cells. Top, cyclic RGD peptide, has been used to target v 3 integrins, which are over-expressed on tumour vasculature. Bottom, folic acid, a ligand used to target the folate receptors on ovarian cancer tissue.
96
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
fast internalisation as well as cell surface recycling rates in cancer cells [126]. On binding, ovarian cells, characterised to express 318 106 folate receptors/cell, can internalise 3 105 molecules of folic acid/h. This inherent property of the ligandreceptor conjugate could enhance accumulation of nanoparticles by faster clearance from the tumour interstitium through faster internalisation of ligand-conjugated nanoparticles. Creating greater diffusion gradients would encourage faster diffusion of nanoparticle through the tumour vasculature. The ligands also need to be conjugated onto nanoparticles in an optimal fashion, as to maintain their afnities for their corresponding receptors. For example, the measured dissociation constants for optimally conjugated HER-2 antibodies were similar to free antibodies, around 12-15 nM, depending on the surface PEG density [112,127]. The targeting layer is presented as the ultimate exterior of the nanoparticle, the surface that interacts primarily with cell membranes. Irrespective of their nature, the ligand must have the right conformation, high afnities for corresponding receptors, and be able to exhibit high rates of cellular internalisation. Furthermore, the loading and presentation of the ligand on nanoparticle surfaces must be cooperative with the stealth layer. It is important to incorporate PEG chains at densities that allow optimal coverage, which means inducing brush conformations on nanoparticle surfaces, as discussed earlier. As the brush conformation allows the extension of the PEG chains away from the nanoparticle surface, presenting targeting ligands on such a platform should allow increased interactions with corresponding receptors. The use of antibodies as targeting ligands has been widely studied due to their high afnities to cognate receptors. A prominent example has been the use of HER-2 antibodies, which target the HER-2 receptor that are over-expressed on cancer cells [128130]. Incorporation of anti-HER2 antibodies onto the surfaces of PEGylated liposomes has indeed shown greater efciency for drug delivery compared to non-targeted PEG-liposomes [131]. Treatment of tumour models with doxorubicin-encapsulated liposomes enabled complete depletion in subcutaneous tumours, when the antibodies are conjugated onto a liposomal platform of optimal PEG2000 density (6 mol%). In this case, and in most examples of targeted nanoparticles, increased therapeutic effect of targeted nanoparticles is a result of increased tumour cell uptake, and not tumour-accumulation (within tumour interstitium). Both targeted and non-targeted nanoparticles arrive at the tumour vicinity via the EPR effect, after which the mechanism of tumour cell internalisation is enhanced by the presence of surface ligands. Although the presentation of ligands on a PEG-brush surface enhances their binding to receptors, their improved exposure can decrease the nanoparticle lifetimes in circulation. Using an RGDtargeted stealth system, nanoparticles carrying doxorubicin were found to accumulate faster and in higher concentrations in the liver and the spleen [132]. Faster clearance from circulation generally corresponds to a higher and faster accumulation into the liver and the spleen (RES). In this example, the total amount of PEG2000 content was included at optimal brush densities, at 6.5 mol%. The ligands are incorporated as RGD-PEG-lipid conjugates, which indicates their extension from the nanoparticle surface as a consequence of the brush-like state. Presentation of the ligand in a PEG-brush fashion reveals the targeting molecules increasingly to plasma proteins, hence their faster clearance from circulation could be a result of Fc-mediated RES uptake into liver and spleenassociated macrophages [133,134]. When ligands are loaded onto liposomes of ambient PEG2000 density (57 mol%), what is generally observed is a faster clearance from circulation, accompanied by a higher accumulation and internalisation into cancer cells [131,135137]. Most nanoparticle examples that describe successful receptortargeting, use targeting ligands that are loaded onto nanoparticle
surfaces via a PEG spacer. The rationale for such an action lies in the extension of the ligand from the nanoparticle platform, enhancing its exibility and interaction with receptors. Our own work has examined the effects of presenting a ligand without a PEG spacer [117]. Through the synthesis of a peptidelipid conjugate, we were able to functionalise the surfaces of liposomes with peptide ligands specic for the urokinase plasminogen activator receptor. These targeted systems were able to induce enhanced cell-binding and gene delivery compared to non-targeted nanoparticles. However, these ligands are exposed at reduced proximities to nanoparticle surfaces, an event that becomes problematic when long PEG chains are included. Addition of PEG2000 molecules at optimal densities for in vivo delivery is essential, but results in the sterically shielding of the short peptide-lipids, hence preventing their interaction with cellular receptors. Similar studies, using a RGD-type peptide for targeting 5 3 integrins, also describe this nding. This report showed that short peptide-targeted nanoparticles exhibited lower cell-binding abilities when higher mol% of PEG2000 was included into the formulation [106,138]. As a sufcient PEG coating is essential for avoiding recognition by the RES, ligands should be extended away from nanoparticle surfaces, to avoid shielding by the polymer chains. The chain length of the PEG spacer between the ligand and the nanoparticle surface also requires consideration. When the chain length of the PEG spacer is longer than the other PEG chains involved in the PEG-brush, the conjugated ligand can become buried within the brush layer [139]. The extra units of a longer PEG spacer are subject to mushroom-like folding, which results again in limited exposure of the ligand. Implications of this effect have been described with a folate-targeted liposome. Conjugation of the folate through a PEG3400 spacer, when the rest of the stealth content is comprised of PEG2000 , the effect of the ligand is not apparent. The folate-targeted nanoparticles were unable to increase tumouraccumulation, plus they did not exhibit short circulation lifetimes, a consequence commonly accompanying an effectively exposed ligand [134]. The ligand-conjugated PEG spacer therefore needs to be at the same length as the stealth constituent on the surface of the nanoparticle. Concentration of surface ligands is another parameter that affects the ligands targeting effect [140]. Higher ligand densities are envisioned as a method of increasing the probability of nanoparticle interactions with cell receptors (multivalency). However, the presence of increased non-PEG-like material on nanoparticle surfaces can be more detrimental than advantageous to delivery. A study using aptamers as a targeting ligand for prostate cancer-specic antigens (PSMA) demonstrated that higher densities of surface ligands resulted in greater accumulation of nanoparticles into the liver and the spleen [141]. In that study Gu et al. used poly (d,l-lactide-coglycolyde) [PLGA] and PEG triblock copolymer based nanoparticles. The nanoparticles were composed by PLGA-b-PEG and PLGA-b-PEG-b-Apt (aptamer for PSMA) [141]. Localization of such nanoparticles in tumours was also at lower concentrations compared to nanoparticles functionalized with lower densities of aptamers. This suggests that higher coverage of the PEGylated nanoparticles surfaces with targeting ligands further shields the effect of the PEG layer, hence resulting in greater recognition by tumour and spleen-associated macrophages. Later studies using a HER-2 targeting system enhanced this argument, where heavy-ligand loading led to higher clearance rates from circulation [142]. High surface coverage of ligands therefore renders the PEG layer obsolete, an occurrence that needs to be avoided in order to reduce interactions with plasma proteins. Although the physical implications of ligand loading were not studied, the biological effects of antibody-targeted nanoparti-
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099
97
cles demonstrate the importance of optimising ligand densities for maximising their targeting abilities [143]. Examples of targeted nanoparticle drug delivery systems have shown faster and higher concentration accumulation in tumours, compared to non-targeted systems [133,144]. Generally it is believed that the introduction of targeting ligands does not enhance nanoparticle accumulation into tumours, but shows higher efcacy by enhancing internalisation into tumour cells. However, in some cases of antibody and folate-targeted nanoparticles accumulation into tumours was faster than compared to non-targeted nanoparticles [133,144146]. This occurrence is envisioned as a consequence of recognition of the nanoparticles by tumourassociated macrophages (TAM) [134,147150]. In response to this hypothesis, folate receptors have been identied to be overexpressed on TAMS. This effect of TAM-recognition is pronounced when the folate ligands are loaded onto PEG-brushes, a conformation that highlights the exposure of the ligands. 4. Summary and future perspectives Here, we present an overview of the clinically used and tested nanoparticles for imaging and treatment of cancer. Currently, both clinical and preclinical studies show a variety of the type of nanoparticles developed for cancer. There are more types of nanoparticles currently at an early design step that may progress in the future to preclinical development for cancer imaging and therapy. From all these nanoparticles, we would like to highlight the potential value of theragnostic nanoparticles. These nanoparticles are designed to do both imaging (diagnosis) and therapy (i.e. chemotherapy or genetic therapy). A particular version of these nanoparticles is the activation-theranostic nanoparticles. In this case nanoparticles are monitored for their kinetics in tumours. When imaging (i.e. MRI) shows maximum nanoparticle accumulation in tumours a physical source is applied to change the status of the nanoparticles and burst-release the drug. Such source can be the NIR laser, induced heat or the ultrasound induced heat or light for photosensitive components. The changes induced on the nanoparticles can be nanoparticle decomposition, or melting releasing rapidly and locally the active (i.e. chemotherapy). The combination of hyperthermia and locally delivered anticancer agents can lead to very specic tumour only cell killing in a short period of time. This way surgery and/or chronic chemotherapy treatments can be avoided. We have also highlighted important factors that affect the performance of PEG-coated nanoparticles, the PEG size and its grafting density, based on the liposome nanoparticle example. The coupling of PEG and ligands on the nanoparticles, needs to be designed and studied for optimum circulation times, binding and tumour cell uptake. It is an important fact that targeting ligands lead to macrophage recognition and faster clearance compared to the non-targeted nanoparticles. In the future nanoparticles design should introduce cleavable masking of the ligands till reaching the tumour cells. A thorough study of the effect of PEG size and density on nanoparticle kinetics, is needed. As well as more studies are required on the clearance mechanism, the metabolism and excretion of nanoparticles and their components. Nanoparticles for cancer imaging and therapy have evolved rapidly during the last decade and it is expected that more and more will become clinical practise. Their controlled size and multifunctionality are the main reasons for their increasing applications as anticancer agents. References
[1] Ferrari M. Cancer nanotechnology: opportunities and challenges. Nat Rev Cancer 2005;5:16171.
[2] Srinivas PR, Barker P, Srivastava S. Nanotechnology in early detection of cancer. Lab Investig 2002;82:65762. [3] Nie S, Xing Y, Kim GJ, Simons JW. Nanotechnology applications in cancer. Annu Rev Biomed Eng 2007;9:25788. [4] Wang MD, Shin DM, Simons JW, Nie S. Nanotechnology for targeted cancer therapy. Expert Rev Anticancer Ther 2007;7:8337. [5] Cancer nanotechnology: small, but heading for the big time. Nat Rev Drug Discov 2007;6:1745. [6] Golub TR, Slonim DK, Tamayo P, et al. Molecular classication of cancer: class discovery and class prediction by gene expression monitoring. Science 1999;286:5317. [7] Scherf U, Ross DT, Waltham M, et al. A gene expression database for the molecular pharmacology of cancer. Nat Genet 2000;24:23644. [8] Ross DT, Scherf U, Eisen MB, et al. Systematic variation in gene expression patterns in human cancer cell lines. Nat Genet 2000;24:22735. [9] Rubin MA. Use of laser capture microdissection, cDNA microarrays, and tissue microarrays in advancing our understanding of prostate cancer. J Pathol 2001;195:806. [10] Evans WE, Relling MV. Moving towards individualized medicine with pharmacogenomics. Nature 2004;429:4648. [11] Petros WP, Evans WE. Pharmacogenomics in cancer therapy: is host genome variability important? Trends Pharmacol Sci 2004;25:45764. [12] Zolnik BS, Sadrieh N. Regulatory perspective on the importance of ADME assessment of nanoscale material containing drugs. Adv Drug Deliv Rev 2009;61:4227. [13] Matsumura Y, Maeda H. A new concept for macromolecular therapeutics in cancer chemotherapy: mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res 1986;46:638792. [14] Thanou M, Duncan R. Polymer-protein and polymer-drug conjugates in cancer therapy. Curr Opin Investig Drugs 2003;4:7019. [15] Treat J, Greenspan A, Forst D, et al. Antitumor activity of liposomeencapsulated doxorubicin in advanced breast cancer: phase II study. J Natl Cancer Inst 1990;82:170610. [16] Forssen EA, Tokes ZA. Improved therapeutic benets of doxorubicin by entrapment in anionic liposomes. Cancer Res 1983;43:54650. [17] Straubinger RM, Lopez NG, Debs RJ, Hong K, Papahadjopoulos D. Liposomebased therapy of human ovarian cancer: parameters determining potency of negatively charged and antibody-targeted liposomes. Cancer Res 1988;48:523745. [18] Robert NJ, Vogel CL, Henderson IC, et al. The role of the liposomal anthracyclines and other systemic therapies in the management of advanced breast cancer. Semin Oncol 2004;31:10646. [19] Gabizon A, Martin F. Polyethylene glycol-coated (pegylated) liposomal doxorubicin. Rationale for use in solid tumours. Drugs 1997;54(Suppl. 4):1521. [20] Gabizon A, Shmeeda H, Barenholz Y. Pharmacokinetics of pegylated liposomal Doxorubicin: review of animal and human studies. Clin Pharmacokinet 2003;42:41936. [21] Allen TM, Martin FJ. Advantages of liposomal delivery systems for anthracyclines. Semin Oncol 2004;31:515. [22] Papahadjopoulos D, Allen TM, Gabizon A, et al. Sterically stabilized liposomes: improvements in pharmacokinetics and antitumor therapeutic efcacy. Proc Natl Acad Sci USA 1991;88:114604. [23] Woodle MC, Lasic DD. Sterically stabilized liposomes. Biochim Biophys Acta 1992;1113:17199. [24] Damascelli B, Cantu G, Mattavelli F, et al. Intraarterial chemotherapy with polyoxyethylated castor oil free paclitaxel, incorporated in albumin nanoparticles (ABI-007): phase II study of patients with squamous cell carcinoma of the head and neck and anal canal: preliminary evidence of clinical activity. Cancer 2001;92:2592602. [25] Desai N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxel concentrations, and endothelial cell transport of cremophor-free, albumin-bound paclitaxel, ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res 2006;12:131724. [26] Miele E, Spinelli GP, Tomao F, Tomao S. Albumin-bound formulation of paclitaxel (Abraxane ABI-007) in the treatment of breast cancer. Int J Nanomed 2009;4:99105. [27] Vogel SM, Minshall RD, Pilipovic M, Tiruppathi C, Malik AB. Albumin uptake and transcytosis in endothelial cells in vivo induced by albumin-binding protein. Am J Physiol Lung Cell Mol Physiol 2001;281:L151222. [28] Hawkins MJ, Soon-Shiong P, Desai N. Protein nanoparticles as drug carriers in clinical medicine. Adv Drug Deliv Rev 2008;60:87685. [29] Drummond DC, Noble CO, Guo Z, Hong K, Park JW, Kirpotin DB. Development of a highly active nanoliposomal irinotecan using a novel intraliposomal stabilization strategy. Cancer Res 2006;66:32717. [30] Flexman JA, Yung A, Yapp DT, Ng SS, Kozlowski P. Assessment of vessel size by MRI in an orthotopic model of human pancreatic cancer. Conf Proc IEEE Eng Med Biol Soc 2008;2008:8514. [31] Davis ME. The rst targeted delivery of siRNA in humans via a self-assembling, cyclodextrin polymer-based nanoparticle: from concept to clinic. Mol Pharm 2009;6:65968. [32] Poon RT, Borys N. Lyso-thermosensitive liposomal doxorubic: a novel approach to enhance efcacy of thermal ablation of liver cancer. Expert Opin Pharmacother 2009;10:33343. [33] Kong G, Anyarambhatla G, Petros WP, et al. Efcacy of liposomes and hyperthermia in a human tumor xenograft model: importance of triggered drug release. Cancer Res 2000;60:69507.
98
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099 [70] Lal S, Clare SE, Halas NJ. Nanoshell-enabled photothermal cancer therapy: impending clinical impact. Acc Chem Res 2008;41:184251. [71] Loo C, Lin A, Hirsch L, et al. Nanoshell-enabled photonics-based imaging and therapy of cancer. Technol Cancer Res Treat 2004;3:3340. [72] von Maltzahn G, Park JH, Agrawal A, et al. Computationally guided photothermal tumor therapy using long-circulating gold nanorod antennas. Cancer Res 2009;69:3892900. [73] Bergstrom K, Osterberg E, Holmberg K, et al. Effects of branching and molecular weight of surface-bound poly(ethylene oxide) on protein rejection. J Biomater Sci Polym Ed 1994;6:12332. [74] Allen C, Dos Santos N, Gallagher R, et al. Controlling the physical behavior and biological performance of liposome formulations through use of surface grafted poly(ethylene glycol). Biosci Rep 2002;22:22550. [75] Woodle MC. Sterically stabilized liposome therapeutics. Adv Drug Deliv Rev 1995;16:24965. [76] Andresen TL, Jensen SS, Jorgensen K. Advanced strategies in liposomal cancer therapy: problems and prospects of active and tumor specic drug release. Prog Lipid Res 2005;44:6897. [77] Immordino ML, Dosio F, Cattel L. Stealth liposomes: review of the basic science, rationale, and clinical applications, existing and potential. Int J Nanomed 2006;1:297315. [78] Kostarelos K, Miller AD. Synthetic, self-assembly ABCD nanoparticles; a structural paradigm for viable synthetic non-viral vectors. Chem Soc Rev 2005;34:97094. [79] Hoarau D, Delmas P, David S, Roux E, Leroux JC. Novel long-circulating lipid nanocapsules. Pharm Res 2004;21:17839. [80] Torchilin VP, Omelyanenko VG, Papisov MI, et al. Poly(ethylene glycol) on the liposome surface: on the mechanism of polymer-coated liposome longevity. Biochim Biophys Acta 1994;1195:1120. [81] Vonarbourg A, Passirani C, Saulnier P, Benoit JP. Parameters inuencing the stealthiness of colloidal drug delivery systems. Biomaterials 2006;27:435673. [82] Woodle MC. Controlling liposome blood clearance by surface-grafted polymers. Adv Drug Deliv Rev 1998;32:13952. [83] Simoes S, Slepushkin V, Gaspar R, Pedroso de Lima MC. Duzgunes N. Successful transfection of lymphocytes by ternary lipoplexes. Biosci Rep 1999;19: 6019. [84] Kenworthy AK, Hristova K, Needham D, McIntosh TJ. Range and magnitude of the steric pressure between bilayers containing phospholipids with covalently attached poly(ethylene glycol). Biophys J 1995;68:192136. [85] Dos Santos N, Allen C, Doppen AM, et al. Inuence of poly(ethylene glycol) grafting density and polymer length on liposomes: relating plasma circulation lifetimes to protein binding. Biochim Biophys Acta 2007;1768:136777. [86] Degennes PG. Polymers at an interfacea simplied view. Adv Colloid Interface 1987;27:189209. [87] Yan X, Scherphof GL, Kamps JA. Liposome opsonization. J Liposome Res 2005;15:10939. [88] Szleifer I. Polymers proteins: interactions at interfaces. Curr Opin Solid St M 1997;2:33744. [89] Jeon SI, Lee JH, Andrade JD, Degennes PG. Protein surface interactions in the presence of polyethylene oxide.1, Simplied theory. J Colloid Interface Sci 1991;142:14958. [90] Gbadamosi JK, Hunter AC, Moghimi SM. PEGylation of microspheres generates a heterogeneous population of particles with differential surface characteristics and biological performance. Febs Lett 2002;532:33844. [91] Wang XY, Ishida T, Kiwada H. Anti-PEG IgM elicited by injection of liposomes is involved in the enhanced blood clearance of a subsequent dose of PEGylated liposomes. J Control Rel 2007;119:23644. [92] Tagami T, Nakamura K, Shimizu T, Ishida T, Kiwada H. Effect of siRNA in PEG-coated siRNA-lipoplex on anti-PEG IgM production. J Contr Rel 2009;137:23440. [93] Ishida T, Kashima S, Kiwada H. The contribution of phagocytic activity of liver macrophages to the accelerated blood clearance (ABC) phenomenon of PEGylated liposomes in rats. J Control Rel 2008;126:1625. [94] Ishida T, Kiwada H. Accelerated blood clearance (ABC) phenomenon upon repeated injection of PEGylated liposomes. Int J Pharm 2008;354:5662. [95] Ishida T, Atobe K, Wang XY, Kiwada H. Accelerated blood clearance of PEGylated liposomes upon repeated injections: effect of doxorubicinencapsulation and high-dose rst injection. J Control Rel 2006;115:2518. [96] Judge A, McClintock K, Phelps JR, Maclachlan I. Hypersensitivity and loss of disease site targeting caused by antibody responses to PEGylated liposomes. Mol Ther 2006;13:32837. [97] Gupta AK, Gupta M. Synthesis and surface engineering of iron oxide nanoparticles for biomedical applications. Biomaterials 2005;26:39954021. [98] Berry CC, Wells S, Charles S, Curtis AS. Dextran and albumin derivatised iron oxide nanoparticles: inuence on broblasts in vitro. Biomaterials 2003;24:45517. [99] Gupta AK, Curtis AS. Surface modied superparamagnetic nanoparticles for drug delivery: interaction studies with human broblasts in culture. J Mater Sci Mater Med 2004;15:4936. [100] Shenoy D, Fu W, Li J, et al. Surface functionalization of gold nanoparticles using hetero-bifunctional poly(ethylene glycol) spacer for intracellular tracking and delivery. Int J Nanomed 2006;1:517. [101] Cai QY, Kim SH, Choi KS, et al. Colloidal gold nanoparticles as a bloodpool contrast agent for X-ray computed tomography in mice. Investig Radiol 2007;42:797806.
[34] Peer D, Karp JM, Hong S, Farokhzad OC, Margalit R, Langer R. Nanocarriers as an emerging platform for cancer therapy. Nat Nanotechnol 2007;2:75160. [35] Davis ME, Chen ZG, Shin DM. Nanoparticle therapeutics: an emerging treatment modality for cancer. Nat Rev Drug Discov 2008;7:77182. [36] Cho K, Wang X, Nie S, Chen ZG, Shin DM. Therapeutic nanoparticles for drug delivery in cancer. Clin Cancer Res 2008;14:13106. [37] Lammers T, Hennink WE, Storm G. Tumour-targeted nanomedicines: principles and practice. Br J Cancer 2008;99:3927. [38] Bharali DJ, Khalil M, Gurbuz M, Simone TM, Mousa SA. Nanoparticles and cancer therapy: a concise review with emphasis on dendrimers. Int J Nanomed 2009;4:17. [39] Tanaka T, Decuzzi P, Cristofanilli M, et al. Nanotechnology for breast cancer therapy. Biomed Microdevices 2009;11:4963. [40] Farokhzad OC, Langer R. Impact of nanotechnology on drug delivery. ACS Nano 2009;3:1620. [41] Youan BB. Impact of nanoscience and nanotechnology on controlled drug delivery. Nanomedicine 2008;3:4016. [42] Byrne JD, Betancourt T, Brannon-Peppas L. Active targeting schemes for nanoparticle systems in cancer therapeutics. Adv Drug Deliv Rev 2008;60:161526. [43] Cohen BE, Bangham AD. Diffusion of small nonelectrolytes across liposome membranes. Nature 1972;236, 173-&. [44] Johnson SM, Bangham AD. Potassium permeability of single compartment liposomes with and without valinomycin. Biochim Biophys Acta 1969;193, 82-&. [45] Lasic D, editor. Medical application of liposomes. Amsterdam: Elsevier; 1998. [46] Torchilin VP. Recent advances with liposomes as pharmaceutical carriers. Nat Rev Drug Discov 2005;4:14560. [47] Allen TM, Cullis PR. Drug delivery systems: entering the mainstream. Science 2004;303:181822. [48] Muller RH, Mehnert W, Lucks JS, et al. Solid lipid nanoparticles (Sln)an alternative colloidal carrier system for controlled drug-delivery. Eur J Pharm Biopharm 1995;41:629. [49] Cavalli R, Caputo O, Carlotti ME, Trotta M, Scarnecchia C, Gasco MR. Sterilization and freeze-drying of drug-free and drug-loaded solid lipid nanoparticles. Int J Pharm 1997;148:4754. [50] Almelda AJ, Souto E. Solid lipid nanoparticles as a drug delivery system for peptides and proteins. Adv Drug Deliv Rev 2007;59:47890. [51] Wissing SA, Kayser O, Muller RH. Solid lipid nanoparticles for parenteral drug delivery. Adv Drug Deliv Rev 2004;56:125772. [52] Wong HL, Bendayan R, Rauth AM, Li YQ, Wu XY. Chemotherapy with anticancer drugs encapsulated in solid lipid nanoparticles. Adv Drug Deliv Rev 2007;59:491504. [53] Tomalia DA, Uppuluri S, Swanson DR, et al. Dendritic macromolecules: a fourth major class of polymer architecturenew properties driven by architecture. Mater Res Soc Symp P 1999;543:28998. [54] Hawker CJ, Frechet JMJ. Preparation of polymers with controlled molecular architecturea new convergent approach to dendritic macromolecules. J Am Chem Soc 1990;112:763847. [55] Svenson S, Tomalia DA. Commentarydendrimers in biomedical applications - reections on the eld. Adv Drug Deliv Rev 2005;57:210629. [56] Wolinsky JB, Grinstaff MW. Therapeutic and diagnostic applications of dendrimers for cancer treatment. Adv Drug Deliv Rev 2008;60:103755. [57] Barth RF, Coderre JA, Vicente MGH, Blue TE. Boron neutron capture therapy of cancer: current status and future prospects. Clin Cancer Res 2005;11:39874002. [58] Shi XG, Wang SH, Meshinchi S, et al. Dendrimer-entrapped gold nanoparticles as a platform for cancer-cell targeting and Imaging. Small 2007;3:1245 52. [59] Wiener EC, Brechbiel MW, Brothers H, et al. Dendrimer-based metal chelates: a new class of magnetic resonance imaging contrast agents. Magn Reson Med 1994;31:18. [60] Gunasekera UA, Pankhurst QA, Douek M. Imaging applications of nanotechnology in cancer. Target Oncol 2009;4:16981. [61] Peng XH, Qian X, Mao H, et al. Targeted magnetic iron oxide nanoparticles for tumor imaging and therapy. Int J Nanomed 2008;3:31121. [62] Yu MK, Jeong YY, Park J, et al. Drug-loaded superparamagnetic iron oxide nanoparticles for combined cancer imaging and therapy in vivo. Angew Chem Int Ed Engl 2008;47:53625. [63] Moore A, Medarova Z. Imaging of siRNA delivery and silencing. Methods Mol Biol 2009;487:93110. [64] Medarova Z, Pham W, Farrar C, Petkova V, Moore A. In vivo imaging of siRNA delivery and silencing in tumors. Nat Med 2007;13:3727. [65] Harisinghani MG, Saksena MA, Hahn PF, et al. Ferumoxtran-10-enhanced MR lymphangiography: does contrast-enhanced imaging alone sufce for accurate lymph node characterization? AJR Am J Roentgenol 2006;186:1448. [66] Sharma R, Saini S, Ros PR, et al. Safety prole of ultrasmall superparamagnetic iron oxide ferumoxtran-10: phase II clinical trial data. J Magn Reson Imag 1999;9:2914. [67] Islam T, Harisinghani MG. Overview of nanoparticle use in cancer imaging. Cancer Biomark 2009;5:617. [68] Averitt RD, Westcott SL, Halas NJ. Linear optical properties of gold nanoshells. J Opt Soc Am B 1999;16:182432. [69] Hirsch LR, Stafford RJ, Bankson JA, et al. Nanoshell-mediated near-infrared thermal therapy of tumors under magnetic resonance guidance. Proc Natl Acad Sci USA 2003;100:1354954.
M. Wang, M. Thanou / Pharmacological Research 62 (2010) 9099 [102] Mei BC, Susumu K, Medintz IL, Mattoussi H. Polyethylene glycol-based bidentate ligands to enhance quantum dot and gold nanoparticle stability in biological media. Nat Protoc 2009;4:41223. [103] Otsuka H, Nagasaki Y, Kataoka K. PEGylated nanoparticles for biological and pharmaceutical applications. Adv Drug Deliv Rev 2003;55:40319. [104] Wang AZ, Gu F, Zhang L, et al. Biofunctionalized targeted nanoparticles for therapeutic applications. Expert Opin Biol Ther 2008;8:106370. [105] Wagner E, Curiel D, Cotten M. Delivery of drugs, proteins and genes into cells using transferrin as a ligand for receptor-mediated endocytosis. Adv Drug Deliv Rev 1994;14:11335. [106] Garg A, Tisdale AW, Haidari E, Kokkoli E. Targeting colon cancer cells using PEGylated liposomes modied with a bronectin-mimetic peptide. Int J Pharm 2009;366:20110. [107] Ishida O, Maruyama K, Tanahashi H, et al. Liposomes bearing polyethyleneglycol-coupled transferrin with intracellular targeting property to the solid tumors in vivo. Pharm Res 2001;18:10428. [108] Zhang Y, Zhang YF, Bryant J, Charles A, Boado RJ, Pardridge WM. Intravenous RNA interference gene therapy targeting the human epidermal growth factor receptor prolongs survival in intracranial brain cancer. Clin Cancer Res 2004;10:366777. [109] Tang Y, Scollard D, Chen P, Wang J, Holloway C, Reilly RM. Imaging of HER2/neu expression in BT-474 human breast cancer xenografts in athymic mice using [(99m)Tc]-HYNIC-trastuzumab (Herceptin) Fab fragments. Nucl Med Commun 2005;26:42732. [110] Laginha KM, Moase EH, Yu N, Huang A, Allen TM. Bioavailability and therapeutic efcacy of HER2 scFv-targeted liposomal doxorubicin in a murine model of HER2-overexpressing breast cancer. J Drug Target 2008;16:60510. [111] Maruyama K, Takahashi N, Tagawa T, Nagaike K, Iwatsuru M. Immunoliposomes bearing polyethyleneglycol-coupled Fab fragment show prolonged circulation time and high extravasation into targeted solid tumors in vivo. FEBS Lett 1997;413:17780. [112] Kirpotin D, Park JW, Hong K, et al. Sterically stabilized anti-HER2 immunoliposomes: design and targeting to human breast cancer cells in vitro. Biochemistry 1997;36:6675. [113] Yang L, Mao H, Wang YA, et al. Single chain epidermal growth factor receptor antibody conjugated nanoparticles for in vivo tumor targeting and imaging. Small 2009;5:23543. [114] Yang L, Peng XH, Wang YA, et al. Receptor-targeted nanoparticles for in vivo imaging of breast cancer. Clin Cancer Res 2009;15:472232. [115] Stoppelli MP, Corti A, Sofentini A, Cassani G, Blasi F, Assoian RK. Differentiation-enhanced binding of the amino-terminal fragment of human urokinase plasminogen activator to a specic receptor on U937 monocytes. Proc Natl Acad Sci USA 1985;82:493943. [116] Huai Q, Mazar AP, Kuo A, et al. Structure of human urokinase plasminogen activator in complex with its receptor. Science 2006;311:6569. [117] Wang M, Lowik DW, Miller AD, Thanou M. Targeting the urokinase plasminogen activator receptor with synthetic self-assembly nanoparticles. Bioconjug Chem 2009;20:3240. [118] Ruoslahti E. RGD and other recognition sequences for integrins. Annu Rev Cell Dev Biol 1996;12:697715. [119] Pasqualini R, Koivunen E, Ruoslahti E. Alpha v integrins as receptors for tumor targeting by circulating ligands. Nat Biotechnol 1997;15:5426. [120] Schiffelers RM, Koning GA, ten Hagen TL, et al. Anti-tumor efcacy of tumor vasculature-targeted liposomal doxorubicin. J Control Rel 2003;91:11522. [121] Banerjee R, Tyagi P, Li S, Huang L. Anisamide-targeted stealth liposomes: a potent carrier for targeting doxorubicin to human prostate cancer cells. Int J Cancer 2004;112:693700. [122] Li SD, Chono S, Huang L. Efcient oncogene silencing and metastasis inhibition via systemic delivery of siRNA. Mol Ther 2008;16:9426. [123] Weitman SD, Lark RH, Coney LR, et al. Distribution of the folate receptor GP38 in normal and malignant cell lines and tissues. Cancer Res 1992;52:3396401. [124] Goren D, Horowitz AT, Tzemach D, Tarshish M, Zalipsky S, Gabizon A. Nuclear delivery of doxorubicin via folate-targeted liposomes with bypass of multidrug-resistance efux pump. Clin Cancer Res 2000;6:194957. [125] Pan X, Lee RJ. Tumour-selective drug delivery via folate receptor-targeted liposomes. Expert Opin Drug Deliv 2004;1:717. [126] Paulos CM, Reddy JA, Leamon CP, Turk MJ, Low PS. Ligand binding and kinetics of folate receptor recycling in vivo: impact on receptor-mediated drug delivery. Mol Pharmacol 2004;66:140614.
99
[127] Kirpotin DB, Park JW, Hong K, et al. Targeting of liposomes to solid tumors: the case of sterically stabilized anti-HER2 immunoliposomes. J Liposome Res 1997;7:391417. [128] Mendelsohn J, Baselga J. The EGF receptor family as targets for cancer therapy. Oncogene 2000;19:655065. [129] Holmes WE, Sliwkowski MX, Akita RW, et al. Identication of heregulin. A specic activator of P185ERBB2. Science 1992;256:120510. [130] Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. New Engl J Med 2001;344:78392. [131] Park JW, Hong K, Kirpotin DB, et al. Anti-HER2 immunoliposomes: enhanced efcacy attributable to targeted delivery. Clin Cancer Res 2002;8:117281. [132] Xiong XB, Huang Y, Lu WL, et al. Enhanced intracellular delivery and improved antitumor efcacy of doxorubicin by sterically stabilized liposomes modied with a synthetic RGD mimetic. J Control Rel 2005;107:26275. [133] Elbayoumi TA, Torchilin VP. Enhanced accumulation of long-circulating liposomes modied with the nucleosome-specic monoclonal antibody 2C5 in various tumours in mice: gamma-imaging studies. Eur J Nucl Med Mol Imag 2006;33:1196205. [134] Gabizon A, Horowitz AT, Goren D, Tzemach D, Shmeeda H, Zalipsky S. In vivo fate of folate-targeted polyethylene-glycol liposomes in tumor-bearing mice. Clin Cancer Res 2003;9:65519. [135] Zalipsky S, Puntambekar B, Boulikas P, Engbers CM, Woodle MC. Peptide attachment to extremities of liposomal surface grafted PEG chains: preparation of the long-circulating form of laminin pentapeptide, YIGSR. Bioconjug Chem 1995;6:7058. [136] Fens MH, Hill KJ, Issa J, et al. Liposomal encapsulation enhances the antitumour efcacy of the vascular disrupting agent ZD6126 in murine B16.F10 melanoma. Br J Cancer 2008;99:125664. [137] Allen TM, Hansen C, Martin F, Redemann C, Yauyoung A. Liposomes containing synthetic lipid derivatives of poly(ethylene glycol) show prolonged circulation half-lives in vivo. Biochim Biophys Acta 1991;1066:2936. [138] Demirgoz D, Garg A, Kokkoli E. PR b-targeted PEGylated liposomes for prostate cancer therapy. Langmuir 2008;24:1351824. [139] Sawant RR, Sawant RM, Kale AA, Torchilin VP. The architecture of ligand attachment to nanocarriers controls their specic interaction with target cells. J Drug Target 2008;16:596600. [140] Gantert M, Lewrick F, Adrian JE, et al. Receptor-specic targeting with liposomes in vitro based on sterol-PEG(1300) anchors. Pharm Res 2009;26:52938. [141] Gu F, Zhang L, Teply BA, et al. Precise engineering of targeted nanoparticles by using self-assembled biointegrated block copolymers. Proc Natl Acad Sci USA 2008;105:258691. [142] Shmeeda H, Tzemach D, Mak L, Gabizon A. Her2-targeted pegylated liposomal doxorubicin: retention of target-specic binding and cytotoxicity after in vivo passage. J Control Rel 2009;136:15560. [143] Kirpotin DB, Drummond DC, Shao Y, et al. Antibody targeting of longcirculating lipidic nanoparticles does not increase tumor localization but does increase internalization in animal models. Cancer Res 2006;66: 673240. [144] Kamaly N, Kalber T, Thanou M, Bell JD, Miller AD. Folate receptor targeted bimodal liposomes for tumor magnetic resonance imaging. Bioconjug Chem 2009;20:64855. [145] Elbayoumi TA, Pabba S, Roby A, Torchilin VP. Antinucleosome antibodymodied liposomes and lipid-core micelles for tumor-targeted delivery of therapeutic and diagnostic agents. J Liposome Res 2007;17:114. [146] Song S, Liu D, Peng J, et al. Novel peptide ligand directs liposomes toward EGFR high-expressing cancer cells in vitro and in vivo. FASEB J 2009;23:1396404. [147] Turk MJ, Waters DJ, Low PS. Folate-conjugated liposomes preferentially target macrophages associated with ovarian carcinoma. Cancer Lett 2004;213:16572. [148] Alizadeh D, Zhang L, Hwang J, Schluep T, Badie B. Tumor-associated macrophages are predominant carriers of cyclodextrin-based nanoparticles into gliomas. Nanomedicine 2009;6:38290. [149] Stevens PJ, Sekido M, Lee RJ. A folate receptor-targeted lipid nanoparticle formulation for a lipophilic paclitaxel prodrug. Pharm Res 2004;21:21537. [150] Leimgruber A, Berger C, Cortez-Retamozo V, et al. Behavior of endogenous tumor-associated macrophages assessed in vivo using a functionalized nanoparticle. Neoplasia 2009;11:45968.
Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Mad To Be Normal Conversations With RD Laing 1853433950Dokument408 SeitenMad To Be Normal Conversations With RD Laing 1853433950ronwerter6100% (1)
- DRUG STUDY-1st BatchDokument27 SeitenDRUG STUDY-1st BatchCanny CańasNoch keine Bewertungen
- The Myth of The Absent Black Father - ThinkProgress PDFDokument4 SeitenThe Myth of The Absent Black Father - ThinkProgress PDFBishara WilsonNoch keine Bewertungen
- Dast20 PDFDokument3 SeitenDast20 PDFMarchnuelNoch keine Bewertungen
- Microbiome and CancerDokument63 SeitenMicrobiome and CancerK C Goutham ReddyNoch keine Bewertungen
- Atlas of Full Breast Ultrasonography - 1st PDFDokument392 SeitenAtlas of Full Breast Ultrasonography - 1st PDFIosub Lica-Claudiu100% (3)
- Cardiocare 2000 Operation ManualDokument61 SeitenCardiocare 2000 Operation ManualDokter MoezNoch keine Bewertungen
- Carbon Nanotubes - Properties, Synthesis, Purification and Medical ApplicationsDokument13 SeitenCarbon Nanotubes - Properties, Synthesis, Purification and Medical ApplicationsIonela NeacsuNoch keine Bewertungen
- BiosensorDokument310 SeitenBiosensorduch_204691Noch keine Bewertungen
- Solar Thermoelectric Generators Fabricated On A Silicon-On-Insulator SubstrateDokument13 SeitenSolar Thermoelectric Generators Fabricated On A Silicon-On-Insulator SubstrateIonela NeacsuNoch keine Bewertungen
- Supplementary Material: Preparation of The Ninps/Ito ElectrodeDokument2 SeitenSupplementary Material: Preparation of The Ninps/Ito ElectrodeIonela NeacsuNoch keine Bewertungen
- The Swedish Higher Education SystemDokument2 SeitenThe Swedish Higher Education SystemIonela NeacsuNoch keine Bewertungen
- Using Area Hierarchy For Multi-Resolution Storage and Search in Large Wireless Sensor NetworksDokument27 SeitenUsing Area Hierarchy For Multi-Resolution Storage and Search in Large Wireless Sensor NetworksIonela NeacsuNoch keine Bewertungen
- Iwanicki IR CS 045 2008Dokument8 SeitenIwanicki IR CS 045 2008Ionela NeacsuNoch keine Bewertungen
- AMCh 1Dokument29 SeitenAMCh 1Anonymous h87K4sTNoch keine Bewertungen
- Gas Sensors Preprints - PDDokument24 SeitenGas Sensors Preprints - PDIonela NeacsuNoch keine Bewertungen
- NCPDokument11 SeitenNCPJohnhineNoch keine Bewertungen
- Diaper Decoder Poster v2Dokument1 SeiteDiaper Decoder Poster v2abhiNoch keine Bewertungen
- Example 1: Application LetterDokument2 SeitenExample 1: Application LetterYulinar MashuriNoch keine Bewertungen
- Issue-9-GRE Sample Issue Pool Essay Topic 83Dokument1 SeiteIssue-9-GRE Sample Issue Pool Essay Topic 83Janavi KhochareNoch keine Bewertungen
- Shell Gadus S3 Wirerope T: Performance, Features & Benefits Main ApplicationsDokument2 SeitenShell Gadus S3 Wirerope T: Performance, Features & Benefits Main ApplicationssfkcrcnNoch keine Bewertungen
- ACLS Advanced Cardiac Life Support, Iridia MedicalDokument54 SeitenACLS Advanced Cardiac Life Support, Iridia MedicalYu Lin ZhangNoch keine Bewertungen
- Introduction To Human BodyDokument57 SeitenIntroduction To Human Bodyjunitria13Noch keine Bewertungen
- Method StatementDokument20 SeitenMethod StatementCharles IkenyeNoch keine Bewertungen
- Dakar DeclarationDokument2 SeitenDakar DeclarationEberechiNoch keine Bewertungen
- Workup For ProteinuriaDokument17 SeitenWorkup For ProteinuriaSantiago ChávezNoch keine Bewertungen
- Soal Tes 1 Sem 6 S1 Reg 2021Dokument3 SeitenSoal Tes 1 Sem 6 S1 Reg 2021arka jrNoch keine Bewertungen
- Philippine Nursing Organizations Org Name DescriptionDokument8 SeitenPhilippine Nursing Organizations Org Name DescriptionShehada Marcos BondadNoch keine Bewertungen
- The 28-Day Crossfit Program For BeginnersDokument2 SeitenThe 28-Day Crossfit Program For BeginnersAditya Pratap SinghNoch keine Bewertungen
- Husky Air Compressor Operator ManualDokument60 SeitenHusky Air Compressor Operator ManualJ DavisNoch keine Bewertungen
- The Factories Act, 1948Dokument14 SeitenThe Factories Act, 1948Nirmalkumar NatarajanNoch keine Bewertungen
- The Tongue - Facts, Function & Diseases - Live SciencerDokument12 SeitenThe Tongue - Facts, Function & Diseases - Live SciencerImtiax LaghariNoch keine Bewertungen
- ISSLDokument58 SeitenISSLsufiNoch keine Bewertungen
- Avoiding The Line of Fire: "For Safety's Sake - Do Something"Dokument1 SeiteAvoiding The Line of Fire: "For Safety's Sake - Do Something"Sergio SáezNoch keine Bewertungen
- Case Study PresentationDokument19 SeitenCase Study PresentationShariq Siddiqui100% (1)
- 3-2. Assessing Production DocumentsDokument48 Seiten3-2. Assessing Production DocumentsSandeep sharmaNoch keine Bewertungen
- Proposed Research BudgetDokument3 SeitenProposed Research BudgetAndreMostertNoch keine Bewertungen
- Evaluate Med TechDokument35 SeitenEvaluate Med TechWilly Pérez-Barreto MaturanaNoch keine Bewertungen
- Swedish Group - ProgrammeDokument3 SeitenSwedish Group - Programmemarudo01Noch keine Bewertungen