Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Lesson Notes - Bed BathDokument5 SeitenLesson Notes - Bed BathNicole Marin-ChingNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Lesson Notes - CBGDokument6 SeitenLesson Notes - CBGNicole Marin-ChingNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Lesson Notes - Insulin PenDokument6 SeitenLesson Notes - Insulin PenNicole Marin-Ching100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Lesson Notes - Body MechanicsDokument9 SeitenLesson Notes - Body MechanicsNicole Marin-ChingNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Lesson Notes - Pulse RateDokument4 SeitenLesson Notes - Pulse RateNicole Marin-ChingNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Lesson Notes - Blood Pressure ManagementDokument4 SeitenLesson Notes - Blood Pressure ManagementNicole Marin-ChingNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Powerpoint - Body MechanicsDokument69 SeitenPowerpoint - Body MechanicsNicole Marin-ChingNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Lesson Notes - Insulin VialDokument6 SeitenLesson Notes - Insulin VialNicole Marin-ChingNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Case StudyDokument5 SeitenCase StudyNicole Marin-ChingNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Lesson Notes - Pain AssessmentDokument2 SeitenLesson Notes - Pain AssessmentNicole Marin-ChingNoch keine Bewertungen
- Gemma Bautista 4 Enya Lacsina Enya Lacsina 2Dokument20 SeitenGemma Bautista 4 Enya Lacsina Enya Lacsina 2Nicole Marin-ChingNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Lesson Notes - PainDokument4 SeitenLesson Notes - PainNicole Marin-ChingNoch keine Bewertungen
- Hardbound 4 JomerDokument99 SeitenHardbound 4 JomerNicole Marin-ChingNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Pamantasan NG Lungsod NG MaynilaDokument1 SeitePamantasan NG Lungsod NG MaynilaNicole Marin-ChingNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- CodesgfDokument25 SeitenCodesgfNicole Marin-ChingNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- NursesDokument2 SeitenNursesDhingskie100% (5)
- NANDA Group ListDokument5 SeitenNANDA Group ListWahyu KristiyawanNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- NCP 2Dokument8 SeitenNCP 2Nicole Marin-ChingNoch keine Bewertungen
- Planning: Cecille O. Martinez RN, RM, Man, Edd (C)Dokument90 SeitenPlanning: Cecille O. Martinez RN, RM, Man, Edd (C)Nicole Marin-ChingNoch keine Bewertungen
- Medical AbbreviationDokument37 SeitenMedical AbbreviationJessica QueNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- CasesDokument1 SeiteCasesNicole Marin-ChingNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- NCPDokument6 SeitenNCPNicole Marin-ChingNoch keine Bewertungen
- Assessment Nursing Diagnosis Inference Planning Interventions Rationale EvaluationDokument2 SeitenAssessment Nursing Diagnosis Inference Planning Interventions Rationale EvaluationNicole Marin-ChingNoch keine Bewertungen
- Maternal and Child Health Is The Program of The Department of Health Created To Lessen The Death of Infants and Mother in The PhilippinesDokument18 SeitenMaternal and Child Health Is The Program of The Department of Health Created To Lessen The Death of Infants and Mother in The PhilippinesNicole Marin-ChingNoch keine Bewertungen
- Care of Indwelling or Foley CatheterDokument2 SeitenCare of Indwelling or Foley CatheterNicole Marin-ChingNoch keine Bewertungen
- LinaDokument5 SeitenLinaNicole Marin-ChingNoch keine Bewertungen
- Mental Health - Di Pa Final (HW)Dokument9 SeitenMental Health - Di Pa Final (HW)Nicole Marin-ChingNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Related LawsDokument5 SeitenRelated LawsNicole Marin-ChingNoch keine Bewertungen
- Nursing Republic Acts PhilippinesDokument2 SeitenNursing Republic Acts PhilippinesNicole Marin-ChingNoch keine Bewertungen
- Civil Law Case DigestDokument17 SeitenCivil Law Case DigestJanine Kae UrsulumNoch keine Bewertungen
- Dengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaDokument18 SeitenDengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaYesi Maulani NovitasariNoch keine Bewertungen
- Determinan Kejadian Demam Berdarah Dengue (DBD) Di Kecamatan Medan Tembung Dian Maya Sari, Sori Muda Sarumpaet, Dan HiswaniDokument17 SeitenDeterminan Kejadian Demam Berdarah Dengue (DBD) Di Kecamatan Medan Tembung Dian Maya Sari, Sori Muda Sarumpaet, Dan HiswaniRyadhianNoch keine Bewertungen
- 3 Nursing Care Plans For Dengue Hemorrhagic FeverDokument8 Seiten3 Nursing Care Plans For Dengue Hemorrhagic FeverCarren Wingwash100% (3)
- Communicablediseaseqa 140829080936 Phpapp02Dokument20 SeitenCommunicablediseaseqa 140829080936 Phpapp02Keiarah Kath Estrada CallaoNoch keine Bewertungen
- Dengue: Ades Aegypti Mosquito, Which Feed During The DayDokument6 SeitenDengue: Ades Aegypti Mosquito, Which Feed During The DayPulkit BansalNoch keine Bewertungen
- Pnle CHN PDFDokument11 SeitenPnle CHN PDFapremsNoch keine Bewertungen
- DIGESTDokument12 SeitenDIGESTTrisha Paola TanganNoch keine Bewertungen
- DengueDokument44 SeitenDengueAl JihadNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CHN Ratio Test 2022Dokument12 SeitenCHN Ratio Test 2022Arvinjohn GacutanNoch keine Bewertungen
- Emerging Epidemics-Dengue and ChikungunyaDokument32 SeitenEmerging Epidemics-Dengue and ChikungunyabobbymayaaNoch keine Bewertungen
- Nurse Hooman-QuestionsDokument39 SeitenNurse Hooman-QuestionsSophia Gella FredilesNoch keine Bewertungen
- LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Dokument8 SeitenLPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085le sage0% (1)
- A Major ResearchProposal Group2 BSN3D v1.0 20210117Dokument13 SeitenA Major ResearchProposal Group2 BSN3D v1.0 20210117Iosif CadeNoch keine Bewertungen
- Dengue FeverDokument15 SeitenDengue Feversylvia100% (1)
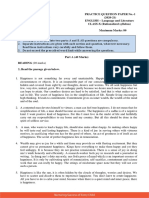
- Practice Question Paper No.-1 (2020-21) ENGLISH - Language and Literature CLASS-X (Rationalized Syllabus) Time Allowed: 3 Hrs. Maximum Marks: 80Dokument20 SeitenPractice Question Paper No.-1 (2020-21) ENGLISH - Language and Literature CLASS-X (Rationalized Syllabus) Time Allowed: 3 Hrs. Maximum Marks: 80Srish TripathyNoch keine Bewertungen
- Breteau IndexDokument18 SeitenBreteau IndexJa ClementeNoch keine Bewertungen
- Dengue Control ProgramDokument2 SeitenDengue Control ProgramJeanne Mari CostalesNoch keine Bewertungen
- Case Presentation 1Dokument37 SeitenCase Presentation 1Safoora RafeeqNoch keine Bewertungen
- Competency Appraisal 2: PediaDokument85 SeitenCompetency Appraisal 2: PediaAnna Mateo De LeonNoch keine Bewertungen
- A Literature Review On DengueDokument5 SeitenA Literature Review On DengueFrancico XavierNoch keine Bewertungen
- Laporan Kerusakan Sample Laboratorium 2023Dokument349 SeitenLaporan Kerusakan Sample Laboratorium 2023adiNoch keine Bewertungen
- Health9 - q1 - Mod4 - Effects of Environmental Issues - v3Dokument21 SeitenHealth9 - q1 - Mod4 - Effects of Environmental Issues - v3Mark Jonest Balmocena FermanNoch keine Bewertungen
- Diagnosis of Dengue: Dr.M.sravana Durga, 1 Year Junior Resident MD PaediatricsDokument24 SeitenDiagnosis of Dengue: Dr.M.sravana Durga, 1 Year Junior Resident MD PaediatricsAneesh MyneniNoch keine Bewertungen
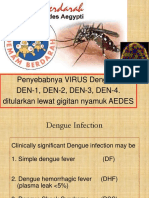
- Penyebabnya VIRUS Dengue: DEN-1, DEN-2, DEN-3, DEN-4. Ditularkan Lewat Gigitan Nyamuk AEDESDokument41 SeitenPenyebabnya VIRUS Dengue: DEN-1, DEN-2, DEN-3, DEN-4. Ditularkan Lewat Gigitan Nyamuk AEDESarischarompisNoch keine Bewertungen
- ELC590 Infomative Speech (Sample) PDFDokument7 SeitenELC590 Infomative Speech (Sample) PDFAinaHadirahNoch keine Bewertungen
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDokument4 SeitenDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodSiddhartha GuptaNoch keine Bewertungen
- Analisis Spasial Tingkat Risiko Wilayah Terhadap DBD (Studi Kasus: Kecamatan Manggala, Panakukkang, Dan Mariso Kota Makassar)Dokument10 SeitenAnalisis Spasial Tingkat Risiko Wilayah Terhadap DBD (Studi Kasus: Kecamatan Manggala, Panakukkang, Dan Mariso Kota Makassar)Afif DhiaulhaqNoch keine Bewertungen
- Emilio Aguinaldo College-Cavite: Communicable Diseases Among InfantsDokument34 SeitenEmilio Aguinaldo College-Cavite: Communicable Diseases Among Infantsarlian malihanNoch keine Bewertungen
- Module 7 - DOH ProgramDokument32 SeitenModule 7 - DOH Programmirai desuNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)