Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CASA 212 - 200 (NS) : NO Description P.N QTY ConditionDokument6 SeitenCASA 212 - 200 (NS) : NO Description P.N QTY ConditionsssavNoch keine Bewertungen
- Area & Perimeter - CRACK SSC PDFDokument10 SeitenArea & Perimeter - CRACK SSC PDFSai Swaroop AttadaNoch keine Bewertungen
- Australian Car Mechanic - June 2016Dokument76 SeitenAustralian Car Mechanic - June 2016Mohammad Faraz AkhterNoch keine Bewertungen
- Prime Time 3 Workbook GrammarDokument2 SeitenPrime Time 3 Workbook GrammarSourCreamNoch keine Bewertungen
- New Holland TM165 Shuttle Command (Mechanical Transmission) PDFDokument44 SeitenNew Holland TM165 Shuttle Command (Mechanical Transmission) PDFElena DNoch keine Bewertungen
- PRANIR ProfileDokument14 SeitenPRANIR ProfileManish VadanereNoch keine Bewertungen
- 2018 Za (Q + Ma) Ac1025Dokument95 Seiten2018 Za (Q + Ma) Ac1025전민건Noch keine Bewertungen
- imageRUNNER+ADVANCE+C5051-5045-5035-5030 Parts CatalogDokument268 SeitenimageRUNNER+ADVANCE+C5051-5045-5035-5030 Parts CatalogDragos Burlacu100% (1)
- Lets Talk About Food Fun Activities Games Oneonone Activities Pronuncia - 1995Dokument1 SeiteLets Talk About Food Fun Activities Games Oneonone Activities Pronuncia - 1995IAmDanaNoch keine Bewertungen
- The Mechanism of Notifying and Record Keeping Three Forms Are Used For Notifying and Record KeepingDokument6 SeitenThe Mechanism of Notifying and Record Keeping Three Forms Are Used For Notifying and Record KeepingRoger FernandezNoch keine Bewertungen
- Consultant Agreement PDFDokument6 SeitenConsultant Agreement PDFRathore&Co Chartered AccountantNoch keine Bewertungen
- Universal Beams PDFDokument2 SeitenUniversal Beams PDFArjun S SanakanNoch keine Bewertungen
- Translation and Distribution Agreement PDFDokument7 SeitenTranslation and Distribution Agreement PDFClaudio Valerio Gaetani80% (5)
- Standards For Pipes and FittingsDokument11 SeitenStandards For Pipes and FittingsMohammed sabatinNoch keine Bewertungen
- PIL HANDOUT in TextDokument173 SeitenPIL HANDOUT in Textbhargavi mishraNoch keine Bewertungen
- I. Characteristics of WastewaterDokument59 SeitenI. Characteristics of WastewaterEljay VinsonNoch keine Bewertungen
- MBFI Quiz KeyDokument7 SeitenMBFI Quiz Keypunitha_pNoch keine Bewertungen
- Hippa and ISO MappingDokument13 SeitenHippa and ISO Mappingnidelel214Noch keine Bewertungen
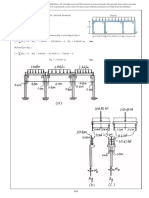
- Problemas Del Capitulo 7Dokument26 SeitenProblemas Del Capitulo 7dic vilNoch keine Bewertungen
- SYKES - Telework Work Area AgreementDokument2 SeitenSYKES - Telework Work Area AgreementFritz PrejeanNoch keine Bewertungen
- NYPE93Dokument0 SeitenNYPE93gvsprajuNoch keine Bewertungen
- SMB Marketing PlaybookDokument18 SeitenSMB Marketing PlaybookpramodharithNoch keine Bewertungen
- Plea Agreement of ThomasbergDokument10 SeitenPlea Agreement of ThomasbergSal CoastNoch keine Bewertungen
- GET IELTS BAND 9 SpeakingDokument54 SeitenGET IELTS BAND 9 Speakingm.alizadehsaraNoch keine Bewertungen
- LSM - Neutral Axis Depth CalculationDokument2 SeitenLSM - Neutral Axis Depth CalculationHimal KafleNoch keine Bewertungen
- E Sevai RegistrationDokument18 SeitenE Sevai RegistrationSatheesh PNoch keine Bewertungen
- Retdem CathDokument17 SeitenRetdem CathShane Aileen AngelesNoch keine Bewertungen
- Mohamed Nagy Elsayed: Supply Chain ManagerDokument6 SeitenMohamed Nagy Elsayed: Supply Chain Managerfasiha thathiNoch keine Bewertungen
- Program 7Dokument6 SeitenProgram 7Khushi GuptaNoch keine Bewertungen
- By Daphne Greaves Illustrated by Michela GalassiDokument15 SeitenBy Daphne Greaves Illustrated by Michela GalassiLucian DilgociNoch keine Bewertungen