Das könnte Ihnen auch gefallen
- Managing Type 2 Diabetes For DummiesVon EverandManaging Type 2 Diabetes For DummiesBewertung: 2 von 5 Sternen2/5 (1)
- Health Declaration FormDokument2 SeitenHealth Declaration Formcreativeraj_181283100% (1)
- SBIL - Health QuestionnaireDokument2 SeitenSBIL - Health QuestionnaireKrishna GBNoch keine Bewertungen
- Health Declaration FormDokument2 SeitenHealth Declaration FormYogesh PatelNoch keine Bewertungen
- Declaration of Good Health Form Ver 3.4 - tcm47-27819 PDFDokument2 SeitenDeclaration of Good Health Form Ver 3.4 - tcm47-27819 PDFAbhinav VermaNoch keine Bewertungen
- Important:: CIGNA Group InsuranceDokument2 SeitenImportant:: CIGNA Group InsuranceLoganBohannonNoch keine Bewertungen
- COI (Certificate of Insurability)Dokument2 SeitenCOI (Certificate of Insurability)bluebird PGNoch keine Bewertungen
- Cooperative Health Management Federation: Enrollment Application Form (Eaf)Dokument2 SeitenCooperative Health Management Federation: Enrollment Application Form (Eaf)Geraldine Daquipil TortalNoch keine Bewertungen
- Life Insurance: Certificate of Insurability For Major Life (Age 18 Years and Above)Dokument3 SeitenLife Insurance: Certificate of Insurability For Major Life (Age 18 Years and Above)Sahana SadanandNoch keine Bewertungen
- Group Enrollment Form PDFDokument2 SeitenGroup Enrollment Form PDFJonelle Morris-Dawkins0% (1)
- DoGH FormDokument2 SeitenDoGH FormcoolgrassNoch keine Bewertungen
- Proposal Form J Arogya T-903Dokument13 SeitenProposal Form J Arogya T-903anurag655Noch keine Bewertungen
- Health Statement FormDokument1 SeiteHealth Statement FormALT IkedaNoch keine Bewertungen
- Mri App Toba Vjul2014Dokument8 SeitenMri App Toba Vjul2014Stephen D RodriguezNoch keine Bewertungen
- Declaration of Good Health Form - With Covid QDokument2 SeitenDeclaration of Good Health Form - With Covid QRajnish YadavNoch keine Bewertungen
- Proposal Form Ashakiran PDFDokument6 SeitenProposal Form Ashakiran PDFSreejith Rajendran PillaiNoch keine Bewertungen
- Mental Health QuestionnaireDokument1 SeiteMental Health QuestionnaireNelly HNoch keine Bewertungen
- Alat GerakDokument2 SeitenAlat Gerakfelicia081585343669Noch keine Bewertungen
- Form 300Dokument8 SeitenForm 300Sachin SharmaNoch keine Bewertungen
- All Savers - EE Enrollment FormDokument4 SeitenAll Savers - EE Enrollment FormJohn PaulNoch keine Bewertungen
- Learners Record BookDokument11 SeitenLearners Record BookMarjhun Flores GuingayanNoch keine Bewertungen
- New Patient Information-2021Dokument6 SeitenNew Patient Information-2021Anime300Noch keine Bewertungen
- Personal Trainer FormsDokument8 SeitenPersonal Trainer FormsWes Geary100% (3)
- Ealth Ertificate Ealth ErtificateDokument1 SeiteEalth Ertificate Ealth ErtificateRendra FelaniNoch keine Bewertungen
- SUNLIFEDokument2 SeitenSUNLIFEGiacenNoch keine Bewertungen
- Instructions and Information For Completing The Evidence of Insurability FormDokument6 SeitenInstructions and Information For Completing The Evidence of Insurability FormnzomniacNoch keine Bewertungen
- MediRaksha Proposal FormDokument4 SeitenMediRaksha Proposal FormNarayana MugalurNoch keine Bewertungen
- Sun Life FormDokument2 SeitenSun Life FormGerald DicenNoch keine Bewertungen
- HDF Health Declaration Form (May-2016) - 2Dokument1 SeiteHDF Health Declaration Form (May-2016) - 2Tabish IslamNoch keine Bewertungen
- Star Health and Allied Insurance Company Limited: Proposal FormDokument2 SeitenStar Health and Allied Insurance Company Limited: Proposal FormBhaktha SinghNoch keine Bewertungen
- Parental Consent Form: To Whom It May ConcernDokument4 SeitenParental Consent Form: To Whom It May ConcernNorman PolilinNoch keine Bewertungen
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Dokument2 SeitenMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviNoch keine Bewertungen
- Hidgh 1Dokument1 SeiteHidgh 1Khawaja IrfanNoch keine Bewertungen
- Bundle 2012053110483376037Dokument7 SeitenBundle 2012053110483376037ryanwoNoch keine Bewertungen
- Proposal Form New India Floater Mediclaim Policy-1Dokument7 SeitenProposal Form New India Floater Mediclaim Policy-1Hemraj SonarNoch keine Bewertungen
- 2015 Ski Venture Booking FormDokument2 Seiten2015 Ski Venture Booking FormdustersNoch keine Bewertungen
- Global Health Employee Application Form Moratorium)Dokument3 SeitenGlobal Health Employee Application Form Moratorium)Amonbek OtambekovNoch keine Bewertungen
- Family HealthDokument2 SeitenFamily HealthsammythomsonNoch keine Bewertungen
- Reg 2-Primary Care Claim Form-31 Oct 2008Dokument2 SeitenReg 2-Primary Care Claim Form-31 Oct 2008Pradeep KhubchandaniNoch keine Bewertungen
- MedicalVerification PDFDokument3 SeitenMedicalVerification PDFOptical RecoveryNoch keine Bewertungen
- Application Form 2015Dokument8 SeitenApplication Form 2015Ladislau F. CsorbaNoch keine Bewertungen
- Member Addition FormDokument3 SeitenMember Addition FormharshitakoutaNoch keine Bewertungen
- Crewsure Claim Form (XLCatlin) 1.3Dokument2 SeitenCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- AUH HealthPerfect ApplicationForm en HRDokument4 SeitenAUH HealthPerfect ApplicationForm en HRVignesh Kumar HariharNoch keine Bewertungen
- Medical CertificateDokument2 SeitenMedical Certificatelaxman28975% (4)
- Family FLoater FormDokument6 SeitenFamily FLoater FormSantosh KodereNoch keine Bewertungen
- AppForm - GroupMedIns - Member - 2016-06 (June14)Dokument3 SeitenAppForm - GroupMedIns - Member - 2016-06 (June14)Ruchie EtolleNoch keine Bewertungen
- Patient Information: Person Responsible For Account (If Other Than Patient)Dokument5 SeitenPatient Information: Person Responsible For Account (If Other Than Patient)abelcooleyNoch keine Bewertungen
- Medical History FormDokument5 SeitenMedical History FormgaloperiscolNoch keine Bewertungen
- Instructions To Guardian:: Guardian'S Report - Minor Current Reporting Period From - ToDokument5 SeitenInstructions To Guardian:: Guardian'S Report - Minor Current Reporting Period From - ToLaurena ThompsonNoch keine Bewertungen
- PHD Life Ver 8Dokument2 SeitenPHD Life Ver 8Anand Kumar VimalanathanNoch keine Bewertungen
- Department of State Academic Exchanges Participant Medical History and Examination FormDokument8 SeitenDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNoch keine Bewertungen
- OVHC Claim Form 102017 PDFDokument3 SeitenOVHC Claim Form 102017 PDFtarmudiNoch keine Bewertungen
- Chiropractic Intake FormDokument4 SeitenChiropractic Intake FormtmontagNoch keine Bewertungen
- Kolkata Claim Form - MD-IndiaDokument4 SeitenKolkata Claim Form - MD-Indiadipankar0majumderNoch keine Bewertungen
- PARQDokument2 SeitenPARQBro KingNoch keine Bewertungen
- Covid-19 Questionnaire (To Be Completed by The Applicant) : Borang Soal Selidik Covid-19 (Diisi Oleh Pemohon)Dokument3 SeitenCovid-19 Questionnaire (To Be Completed by The Applicant) : Borang Soal Selidik Covid-19 (Diisi Oleh Pemohon)Mashitah Md NorNoch keine Bewertungen
- COVID RTW Form (CAN)Dokument3 SeitenCOVID RTW Form (CAN)A. MuyepaNoch keine Bewertungen
- The New India Assurance Company Limited: Head Office: 87, M G Road, Fort, Mumbai-400001 Mediclaim Insurance Proposal FormDokument6 SeitenThe New India Assurance Company Limited: Head Office: 87, M G Road, Fort, Mumbai-400001 Mediclaim Insurance Proposal FormChirantan BuchNoch keine Bewertungen
- Claim Form en Nov 08Dokument4 SeitenClaim Form en Nov 08Juju FernsNoch keine Bewertungen
- MockboardexamDokument13 SeitenMockboardexamJayke TanNoch keine Bewertungen
- Defensive Driving TrainingDokument19 SeitenDefensive Driving TrainingSheri DiĺlNoch keine Bewertungen
- Dinner Theater Business PlanDokument21 SeitenDinner Theater Business PlanBhumika KariaNoch keine Bewertungen
- Comparison of The Gasification Performance in The Downdraftfixed-Bedgasifier Fed by Different Feedstocks Rice Husk, Sawdust, and Their MixtureDokument8 SeitenComparison of The Gasification Performance in The Downdraftfixed-Bedgasifier Fed by Different Feedstocks Rice Husk, Sawdust, and Their MixturechaniefNoch keine Bewertungen
- Latest Eassy Writing Topics For PracticeDokument18 SeitenLatest Eassy Writing Topics For PracticeAnjani Kumar RaiNoch keine Bewertungen
- Research On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaDokument5 SeitenResearch On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaSiddharth ChaudharyNoch keine Bewertungen
- SC Circular Re BP 22 Docket FeeDokument2 SeitenSC Circular Re BP 22 Docket FeeBenjamin HaysNoch keine Bewertungen
- Thermal Hybrids R5Dokument9 SeitenThermal Hybrids R5amir.kalantariNoch keine Bewertungen
- 450-11 Schmalensee RebuttalDokument11 Seiten450-11 Schmalensee RebuttalFlorian MuellerNoch keine Bewertungen
- AP Physics Name: AP Thermal PracticeDokument2 SeitenAP Physics Name: AP Thermal PracticeMuddamsetty ArunkalyanNoch keine Bewertungen
- Leadership and Decision Making PDFDokument34 SeitenLeadership and Decision Making PDFNhi PhamNoch keine Bewertungen
- HP-exampleDokument30 SeitenHP-exampleAnonymous 105zV1Noch keine Bewertungen
- About FW TaylorDokument9 SeitenAbout FW TaylorGayaz SkNoch keine Bewertungen
- BACS2042 Research Methods: Chapter 1 Introduction andDokument36 SeitenBACS2042 Research Methods: Chapter 1 Introduction andblood unityNoch keine Bewertungen
- Cortex - M1: Technical Reference ManualDokument174 SeitenCortex - M1: Technical Reference ManualSzilárd MájerNoch keine Bewertungen
- BSBMGT516 Facilitate Continuous Improvement: Summative Assessment 1Dokument4 SeitenBSBMGT516 Facilitate Continuous Improvement: Summative Assessment 1Mmc MixNoch keine Bewertungen
- Technical Report: Determination of The Resistance To DelaminationDokument4 SeitenTechnical Report: Determination of The Resistance To DelaminationStefan NaricNoch keine Bewertungen
- TrustworthinessDokument24 SeitenTrustworthinessJamsheed Raza100% (1)
- Manual de Parts ES16D6Dokument36 SeitenManual de Parts ES16D6Eduardo CortezNoch keine Bewertungen
- ACCOUNTS Foundation Paper1Dokument336 SeitenACCOUNTS Foundation Paper1mukni613324100% (1)
- BS351: Financial Reporting: Learning ObjectivesDokument3 SeitenBS351: Financial Reporting: Learning ObjectivesMajeed Ullah KhanNoch keine Bewertungen
- Rule 63Dokument43 SeitenRule 63Lady Paul SyNoch keine Bewertungen
- Response LTR 13 330 VielmettiDokument2 SeitenResponse LTR 13 330 VielmettiAnn Arbor Government DocumentsNoch keine Bewertungen
- Course Outline ReviewerDokument12 SeitenCourse Outline Reviewerjmd.besanaNoch keine Bewertungen
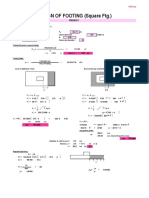
- Design of Footing (Square FTG.) : M Say, L 3.75Dokument2 SeitenDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNoch keine Bewertungen
- Report - Summary - Group 3 - MKT201Dokument4 SeitenReport - Summary - Group 3 - MKT201Long Nguyễn HảiNoch keine Bewertungen
- Object Based and Unified StorageDokument12 SeitenObject Based and Unified Storageashu narayanNoch keine Bewertungen
- Electric Baseboard StelproDokument4 SeitenElectric Baseboard StelprojrodNoch keine Bewertungen
- Case Study 05 PDFDokument5 SeitenCase Study 05 PDFSaltNPepa SaltNPepaNoch keine Bewertungen
- State of The Art Synthesis Literature ReviewDokument7 SeitenState of The Art Synthesis Literature Reviewfvdddmxt100% (2)