Beruflich Dokumente
Kultur Dokumente
Lancet 2006 - Astha Management
Hochgeladen von
api-3826574Originalbeschreibung:
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Lancet 2006 - Astha Management
Hochgeladen von
api-3826574Copyright:
Verfügbare Formate
Review
Pharmacological management of mild or moderate
persistent asthma
Paul M O’Byrne, Krishnan Parameswaran
Lancet 2006; 368: 794–803 Patients with mild persistent asthma rarely see their doctor with symptoms of the disease. Partly as a result of this
Firestone Institute for situation, mild asthma is generally undertreated. Findings of several large randomised clinical trials have shown
Respiratory Health, St Joseph’s benefits for this population of regular treatment with low doses of inhaled corticosteroids. Additional drugs are rarely
Healthcare and Department of
needed, and although leukotriene modifiers are effective, they are less so than inhaled corticosteroids. People with
Medicine, McMaster
University, Hamilton, Ontario, moderate persistent asthma are not well controlled on low doses of inhaled corticosteroids. A combination of this
Canada (P M O’Byrne MB, drug and long-acting inhaled β2 agonists provides improved control compared with doubling of the maintenance
K Parameswaran MD) dose of inhaled corticosteroids. The combination of budesonide and formoterol has been assessed as both maintenance
Correspondence to: and reliever treatment. This approach further reduces the risk for severe exacerbations. With these strategies, most
Dr Paul M O’Byrne, McMaster
individuals can achieve good control of their asthma. For patients who do not achieve asthma control despite taking
University Medical Center,
1200 Main Street West, drugs, measurement of the inflammatory response in the airway in induced sputum could provide further information
Hamilton, Ontario L9G 4R7, to guide treatment.
Canada
obyrnep@mcmaster.ca
Consensus guidelines for asthma treatment have, in start receiving treatment; by contrast, someone with
general, characterised patients as intermittent (very mild) fairly mild symptoms—such as persistent cough—might
asthma, and mild, moderate, and severe persistent not respond adequately to treatment and therefore not be
asthma.1,2 The most widely disseminated of these—from well controlled.
the Global Initiative for Asthma—describe patients with Asthma guidelines highlight consistently the aims and
mild persistent asthma as having symptoms more than objectives of treatment: (1) to minimise or eliminate
once a week but less than daily, nocturnal symptoms asthma symptoms; (2) to achieve the best possible lung
more than twice a month but less than once a week, and function; (3) to prevent asthma exacerbations; (4) to do
with typical lung function (forced expired volume in 1 s the above with the fewest drugs; (5) to keep short-term
[FEV1] or peak expiratory flow >80%) between asthma and long-term adverse effects to a minimum; and (6) to
episodes. Individuals with moderate persistent asthma educate the patient about the disease and goals of
have symptoms daily, nocturnal symptoms at least once a management. One other important objective should be
week, exacerbations that can affect activity and sleep, and prevention of decline in lung function and development
FEV1 or peak expiratory flow of less than 80% but more of fixed airflow obstruction, which happens in some
than 60% predicted. However, if these markers arise patients with asthma. In addition to these goals and
while on treatment, the degree of disease severity is objectives, in each of the guideline documents,
increased from mild to moderate and from moderate to researchers have described what is meant by the term
severe. Furthermore, asthma severity must be asthma control. This definition includes the above
differentiated from asthma control.3 For example, a objectives and additional aims to decrease need for rescue
patient who presents with severe asthma symptoms and treatment—such as inhaled β2 agonists—to less than
airflow obstruction might be well controlled once they daily use, to reduce variability of flow rates that is
characteristic of asthma, and to have usual activities of
Search strategy and selection criteria daily living. Achievement of this level of asthma control
should be an objective from the very first visit of the
We searched the Cochrane library (update May, 2006), MEDLINE (1965–2006), patient to the treating doctor.
OLDMEDLINE (1950–65), EMBASE (1980–April, 2006), and CINAHL (1956–April, 2006) Despite publication of these guidelines, asthma is
with the search terms “asthma”, OR “wheeze*” OR “hyperresponsiveness”. We then sometimes undertreated. Evidence to lend support to this
restricted the results with the terms “clinical trial” OR “treatment” in the electronic search, statement has existed since Turner-Warwick4 reported a
and by hand-searching for “mild” OR “moderate” asthma. We restricted our search to survey of patients managed in primary-care practice.
English language publications. We largely selected publications in the past 10 years but did Findings of telephone surveys in Europe,5 Asia,6 the
not exclude commonly referenced and highly regarded older publications. We also USA,6 and Canada7 have all shown that most people with
searched the reference lists of articles identified by this search strategy and selected those asthma are not ideally controlled. The reasons for this
we judged relevant. Decisions to include specific references were based on authors’ situation are complex, but one possible explanation is
knowledge of published work, participation in expert meetings, and many years of research unawareness by patients (including many with mild
on the subject. Thus, this work is not an exhaustive systematic review of the pharmacology persistent asthma) and their managing doctors that good
and effectiveness of all drugs that have been used to treat asthma. Rather, it is an overview asthma control can and should be achieved. In this
of current best practice strategy based on research evidence, clinical reasoning, theory, and Review, we discuss the effectiveness of current
heuristics. We did not review studies on alternative treatments for asthma. pharmacological treatments for mild and moderate
persistent asthma. Management of mild intermittent
794 www.thelancet.com Vol 368 August 26, 2006
Review
asthma and mechanisms of action of anti-asthma drugs
O’Byrne15 Pauwels16 Boushey17 Zeiger18 Garcia19
are not included.
Total patients (n) 698 7241 225 400 994
Management of mild persistent asthma FEV₁ (% predicted) 89–90% 86% 88–91% 93–95% 87–88%
Patients with mild persistent asthma form a sizable Days with symptoms per week 3 4 4 3·6 NA
proportion of people with asthma (up to 70%);8 these Nocturnal symptoms per week <1 NA NA <1 NA
individuals could be called the silent majority because β2 agonist use (inhalations per week) 7 NA NA 7 5
they rarely visit their family doctor with symptoms of the Values are either taken from or calculated (where available) from information presented in tables of baseline
disease and are seldom seen in a secondary or tertiary characteristics. NA=information not available.
health-care setting, in which most doctors with a focused
Table: Baseline characteristics of patients in clinical trials of mild persistent asthma
interest in asthma management are based. Partly for this
reason, very little attention has been paid to morbidity
associated with mild persistent asthma and in very few benefit when compared with budesonide alone. The
reports have researchers assessed patients’ responses to researchers showed that, for patients with mild persistent
treatment. Indeed, most studies that claim to have asthma, low-dose inhaled corticosteroids alone are the
studied people with mild-to-moderate asthma have not preferred treatment option. By contrast, in the same
included many (or any) individuals with mild disease, as study, another population of patients (group B), who had
indicated by the mean FEV1, which is usually around 70% moderate persistent asthma and used inhaled
predicted normal, rescue β2 agonist use of 2–3 puffs per corticosteroids at study entry, did show a striking and
day, or both.9–14 This situation makes results presented in significant difference in asthma exacerbations when
these reports of little or no value for evaluation of formoterol was added to budesonide (figure 1). The
treatment strategies for patients with mild persistent findings suggested that combination treatment is not
asthma. Fortunately, this omission has been rectified in appropriate for all patients with persistent asthma and
the past 4–5 years (table). that benefit is only seen in those not ideally controlled on
The standard of care for patients with mild persistent low doses of inhaled corticosteroids alone.
asthma in the past was to recommend regular use of Another large study, in which patients with mild
inhaled short-acting β2 agonists.20 However, monotherapy persistent asthma were given inhaled corticosteroids, is
with these drugs results in deterioration of overall asthma the START trial.16 These investigators looked at whether
control21 and in an increased risk for death,22 and this early intervention with inhaled corticosteroids (again,
treatment approach is no longer recommended in budesonide) prevented progression of asthma in adults
national or international guidelines. Subsequently, and children aged 5–11 years with newly diagnosed, mild,
researchers are investigating the benefits of inhaled persistent asthma (table). The outcome was measured by
corticosteroids, which are the pre-eminent anti- time to first very severe exacerbation, which needed a
inflammatory treatment for asthma,23 in patients’ with visit to the emergency room or admission, and by decline
mild persistent disease. Findings of these studies have in post-bronchodilator FEV1. Patients were treated with
lead to some controversy. low-dose budesonide or placebo for 3 years. During the
In the OPTIMA trial,15 the researchers’ objective was to first year, almost 34% of individuals in the placebo arm
assess whether the benefits of adding a long-acting needed additional treatment with inhaled corticosteroids
inhaled β2 agonist (formoterol) to inhaled corticosteroids and 4% had a severe asthma exacerbation. This proportion
(budesonide), particularly for reduction of mild and was reduced in the budesonide arm to 20% needing
severe asthma exacerbations, which had been reported in
people with moderate persistent asthma,24–26 also were 1·0
apparent in patients with mild persistent asthma. In
(number per patient per year)
OPTIMA, two groups of patients were selected: the first 0·8
Rate of exacerbations
(group A) consisted of almost 700 individuals with mild
persistent asthma who had never used inhaled 0·6
corticosteroids (table). In this group, budesonide alone
0·4
(200 μg/day) was compared with the same dose of
budesonide plus formoterol or placebo for 1 year of
0·2
treatment. The primary outcome was rate of severe
asthma exacerbations; this rate was 0·77 per patient per 0·0
year in the placebo-treated group, falling to 0·29 per
9
a
00 0
00
00 0
9
00
18
00 00
18
Pl
or
0
or
B2
B2
8
or
or
B4
B2
+F
+F
patient per year with low-dose budesonide alone (figure 1).
+F
+F
00
B4
B2
B2
B8
All other study outcomes, including days with asthma
symptoms and nights with nocturnal symptoms, were Optima A Optima B FACET
improved by budesonide treatment. The combination of Figure 1: Rate of severe asthma exacerbations in OPTIMA and FACET studies
budesonide and formoterol did not provide any additional Pla=placebo. B200=budesonide 200 μg/day. For9=formoterol 9 μg/day.
www.thelancet.com Vol 368 August 26, 2006 795
Review
additional inhaled corticosteroids and 2% with a severe the proportion needing a course of prednisone throughout
exacerbation. By year 3 of the study, 50% of patients the year was very low and much lower than previously
allocated placebo who had not used inhaled corticosteroids described in similar populations,11 making finding a
at the start of the study were being treated with this drug treatment effect for regular budesonide in a study of this
and 6% of the population had a severe asthma size almost impossible.
exacerbation. In the budesonide arm, 30% were given
additional inhaled corticosteroids and 3% had a severe Is regular use of inhaled corticosteroids in mild
asthma exacerbation. Changes in both pre-bronchodilator persistent asthma worthwhile?
and post-bronchodilator FEV1, although significant, were The most widely used primary outcome variables in
small at the end of 3 years of treatment. Thus, early asthma drug trials—improvements in FEV1 or morning
intervention with low doses of inhaled corticosteroids did peak expiratory flow—are not the best choice in studies of
prevent progression of asthma, but the effects were— patients with mild persistent asthma, because these
particularly in the case of lung function—incomplete. measurements will generally be normal or close to normal
The Childhood Asthma Management Plan (CAMP) in this population. Since this group of patients are
study is a large prospective trial.27 The researchers aimed asymptomatic some of the time, use of symptom scores,
to assess whether treatment with either inhaled control questionnaires, or quality-of-life methods—which
corticosteroids or nedocromil prevented decline in lung are better choices for primary outcome—needs large
function in children with asthma. 1041 children aged sample sizes to be adequately powered because of the
5–12 years with mild-to-moderate asthma were randomly small size of change likely to be seen. Therefore, the
allocated either 200 μg of budesonide, 8 mg of nedocromil, benefits reported in large trials of low-dose daily inhaled
or placebo twice daily for 4–6 years. The primary outcome corticosteroids can seem not worth the effort needed to
was change in FEV1 predicted after administration of a achieve them. However, patients with mild persistent
bronchodilator; this measure was not improved by either asthma have, by definition, persistent symptoms every
active treatment. However, no decline happened in FEV1 week, with nocturnal symptoms occasionally, and rates of
over the 4 years of study in children allocated placebo. severe asthma exacerbations, if untreated, that are higher
Despite the lack of effect on post-bronchodilator FEV1, than expected before the above studies were undertaken.
compared with those allocated nedocromil, children who A trial of low doses of inhaled corticosteroids in patients
received budesonide had a significantly smaller decline with mild persistent asthma should last for at least
in ratio of FEV1 to forced vital capacity and improved 3 months to obtain most therapeutic benefit18 and could
airway responsiveness to methacholine, fewer provide the size of benefit that will ensure that individuals
admissions, fewer urgent visits to a caregiver, greater will continue to use the drug. If this benefit is not
reduction in need for rescue treatment for symptoms, achieved, the patient is unlikely to continue to use inhaled
fewer courses of prednisone, and fewer days on which corticosteroids on a regular basis, and will revert to
additional asthma drugs were needed. intermittent use. However, if a therapeutic trial is not
In the IMPACT study, researchers assessed intermittent attempted, clinical effectiveness will never be known. All
short-course inhaled corticosteroids, guided by a patients with mild persistent asthma deserve the
symptom-based action plan, alone or in addition to daily opportunity to decide whether the benefit from use of
treatment with either budesonide or an anti-leukotriene, inhaled corticosteroids, usually only once daily, is worth
zafirlukast, in 225 adult patients with mild persistent the effort.
asthma for 1 year.17 This population was almost identical A trial of inhaled corticosteroids is frequently
in baseline characteristics to those of OPTIMA and recommended for children with intermittent wheezing
START (table), albeit with a much longer duration of to help in establishing a diagnosis of asthma when
asthma than in these studies. Findings of IMPACT opinion is uncertain. Most episodes of wheezing in
indicated that patients with mild persistent asthma could infants and young children could be due to viral
be treated with intermittent courses of inhaled or oral bronchitis. Findings of a study have shown that twice-
corticosteroids, together with an action plan. This daily administration of inhaled corticosteroids for 2 years,
conclusion was reached despite the fact that regular use compared with placebo, controlled symptoms but had an
of inhaled budesonide was significantly better than effect only during the treatment period, with no carryover
intermittent use in improving pre-bronchodilator FEV1, effect after the drug was stopped (during the third study
asthma control scores, number of symptom-free days, year).28 Intermittent treatment with inhaled corticosteroids
airway hyper-responsiveness, and markers of airway during episodes of wheezing was also not effective at
inflammation (sputum eosinophils and exhaled nitric preventing future episodes of wheezing.29
oxide). Outcomes that were not better were asthma Another issue that needs to be considered when
quality-of-life scores, measurements of morning peak making a decision to start treatment with inhaled
expiratory flow, and post-bronchodilator FEV1. Importantly, corticosteroids in mild asthma is the potential for side-
the proportion of patients with severe asthma effects. These drugs are not metabolised in the lungs and
exacerbations did not differ between groups. However, every molecule of corticosteroid that is administered is
796 www.thelancet.com Vol 368 August 26, 2006
Review
absorbed into the systemic circulation. All studies in from 200 μg/day to 800 μg/day) improved all outcomes,
patients with mild persistent asthma have used low doses but addition of long-acting β2 agonist to the highest dose
of inhaled corticosteroids (maximum dose 400 μg/day). of inhaled corticosteroid was the most effective strategy,
A wealth of data is available showing the safety of these particularly for reduction of severe asthma exacerbations
low doses, even when used long term, in adults.30 (figure 1). Researchers on several subsequent studies could
However, in both the START trial16 and the CAMP study,27 not show any benefit of a two-fold rise in dose of inhaled
a significant reduction in growth velocity of children of corticosteroid for most outcomes assessed, including
1·0–1·5 cm was reported over 3–5 years of treatment reduction of the rate of asthma exacerbations15 or
with budesonide (200–400 μg/day). This finding is prevention of exacerbations.36–38 By contrast, addition of a
unlikely to have any effect on the final height of these long-acting β2 agonist to the inhaled corticosteroid did
children, because one study—in which children treated improve most outcomes,26 including lessening of asthma
with inhaled budesonide were followed up to final exacerbations.15,25,39 Use of a combination of inhaled
height—did not show any detrimental effect, even with corticosteroid and long-acting β2 agonist for patients with
an average dose of 500 μg/day.31 Also, the low doses of moderate persistent asthma has also been shown to
budesonide used in the CAMP study over 3 years did not improve all indicators of asthma control, when compared
have any measurable effect on hypothalamic-pituitary- with a corticosteroid alone,15,40,41
adrenal axis function.32 In the GOAL study,41 researchers investigated how
frequently ideal asthma control can be achieved in three
Other treatment options for mild persistent groups of patients, who mostly had moderate-to-severe
asthma asthma (only 10% of participants had mild persistent
Leukotriene receptor antagonists, which have both disease). The three groups consisted of people not using
bronchodilator and anti-inflammatory properties,33,34 have inhaled corticosteroids at study entry (steroid-naive), and
been assessed and compared with inhaled corticosteroids those taking low-dose or moderate-dose inhaled
in adults18 and children19 with mild persistent asthma. In corticosteroids at study entry, but who were not well
both studies, a leukotriene receptor antagonist, controlled. The study population was randomly allocated
montelukast, was compared with a low-dose inhaled either increasing doses of inhaled corticosteroid alone (to
corticosteroid (fluticasone, 200 μg/day). In these studies, a maximum of 1000 μg/day of fluticasone) or similar
both drugs improved most asthma-control measures, but doses together with the long-acting β2 agonist salmeterol
fluticasone was significantly better for most outcomes. for 1 year. Phase I of the study was dose escalation,
This outcome was especially true in patients who had whereby the dose was stepped up until total asthma
eosinophilic bronchitis. Responses to treatment differed control was achieved or until the maximum dose
within and between individuals.35 Although, on average, (fluticasone 1000 μg or fluticasone 1000 μg and salmeterol
inhaled corticosteroids improve almost all asthma 100 μg daily dose) was reached. Phase II was after total
outcomes, more so than leukotriene receptor antagonists, control was achieved or after 12 weeks on the maximum
some patients might show a greater response to leukotriene dose of drug. Findings suggested that total asthma
receptor antagonists. Currently, accurate identification of control—which was identified by the patient having no
these responders—based on their clinical, physiological, symptoms, normal lung function, and no limitation of
or pharmacogenomic characteristics—is not possible. activities—could be achieved in some patients but in less
Thus, although leukotriene receptor antagonists are than 50% of the overall population and less than 30% of
regarded as a treatment option for patients with mild those already taking moderate doses of inhaled
persistent asthma, they are not as effective as low doses of corticosteroids at randomisation, even with the highest
inhaled corticosteroids. doses of combination treatment. However, well controlled
asthma—defined by the presence of mild occasional
Management of moderate persistent asthma symptoms—was achieved in up to 78% of patients not
Patients with moderate persistent asthma are described as receiving inhaled corticosteroids before study entry and
those whose disease is not well controlled on low doses of in 62% of those already on moderate doses of these drugs
inhaled corticosteroids (≤500 μg of beclometasone or (figure 2). The combination of inhaled corticosteroid and
equivalent dose for other corticosteroids in adults, and long-acting β2 agonist was significantly better than
≤250 μg in children). Asthma-treatment guidelines inhaled corticosteroid alone.
recommend a combination of inhaled corticosteroid and a We should note that evidence for the enhanced benefit
long-acting inhaled β2 agonist in these people.1,2 This of combined inhaled corticosteroids and long-acting β2
recommendation stems from findings of the FACET agonists in patients with moderate persistent asthma
study,25 which compared a low dose of inhaled corticosteroid exists mainly in adults. Findings of a systematic review of
rising to a four-fold increase, with and without a long- eight randomised controlled trials of long-acting β2
acting β2 agonist, in patients with moderate-to-severe agonists to treat symptoms in children using inhaled
persistent asthma. The investigators showed that a four- corticosteroids showed no apparent protection from
fold boost in dose of inhaled corticosteroid (budesonide, asthma exacerbation in those on a β2 agonist compared
www.thelancet.com Vol 368 August 26, 2006 797
Review
Fluticasone phase II Fluticasone and salmeterol phase II non-significant) numbers of asthma-related deaths were
Fluticasone phase I Fluticasone and salmeterol phase I recorded with regular use of salmeterol. The population
80 in the US surveillance study had, in general, very poorly
controlled asthma, yet less than 50% of these patients
Proportion of patients
60 reported being treated with inhaled corticosteroids. The
African-American population had even less well controlled
40
asthma, with lower lung function and even fewer patients
prescribed inhaled corticosteroids. Although long-acting
20
β2 agonists are effective for symptom relief in asthma,
they have not been reported to have clinically important
0
Steroid–naive Low–dose Moderate–dose anti-inflammatory effects. Therefore, their use as
inhaled inhaled monotherapy in patients with poorly controlled asthma is
corticosteroid corticosteroid
not recommended in any treatment guidelines, and it
Figure 2: Proportion of patients achieving good asthma control after 1 year seems to be associated with an increased risk of severe
of treatment with fluticasone either alone or in combination with asthma outcomes and disease-related deaths. Although
salmeterol in the GOAL study
Modified from reference 41 with permission of the American Thoracic Society.
no long-term surveillance study has been undertaken of a
combination of corticosteroid and long-acting β2 agonist
with children using a comparison treatment (mainly in one inhaler, this treatment strategy, as described above,
placebo).42 reduces severe asthma exacerbations and improves
Despite evidence for effectiveness when used in asthma control in all studies in which it has been assessed
combination with inhaled corticosteroids in adults with in adults, with no concerns raised about the safety of these
moderate asthma, considerable concern has been voiced combinations.
about the safety of long-acting β2 agonists. This situation Another treatment approach described for management
arose after publication of a surveillance study, which was of moderate asthma is use of an inhaler containing a
mandated after the long-acting β2 agonist salmeterol was combination of the corticosteroid budesonide and the
approved for use in the USA.43 Researchers identified an long-acting β2 agonist formoterol, for both maintenance
increased risk of respiratory-related mortality or life- and rescue therapy.14,40,45 This approach is possible because
threatening events with salmeterol compared with placebo formoterol is an inhaled β2 agonist, which has a rapid
in a population of patients with asthma, and these onset and a long duration of action46 and acts as a
differences were significant for the African-American bronchodilator as the dose increases.47 The drug can,
subset of study participants. The findings accorded with therefore, be effectively used as relief treatment for
those of another post-marketing surveillance study asthma.48 The idea of using formoterol in combination
undertaken in the UK,44 in which numerically higher (but with an inhaled corticosteroid as both maintenance and
rescue treatment for asthma patients was initially assessed
280 4×BUD+SABA by comparing this approach with high-dose inhaled
200 (294 events) corticosteroids as maintenance and a short-acting inhaled
120 β2 agonist as rescue.14,45 Subsequently, a study was reported
40 in which the strategy of combined maintenance and
0 rescue treatment was compared with a four-fold higher
Number of exacerbations
dose of inhaled corticosteroids as maintenance and a
280 BUD/Form+SABA short-acting β2 agonist as rescue.40 Findings of these
200 (330 events)
studies show that use of this combination as both
120 maintenance and rescue greatly reduces risk for severe
40 asthma exacerbations when compared with other
0
approaches (figure 3), with an associated reduction in oral
280 BUD/Form maintenance and corticosteroid use. Thus, for some patients who need
200 reliever maintenance treatment with a combination inhaler
(160 events)*
120 containing budesonide and formoterol, the inhaler can
also be used as rescue when needed, thereby allowing the
40
0 patient to manage their asthma with one inhaler. The
0 3 6 9 12 15 19 23 27 31 35 39 43 47 51 55 reason for this benefit is not yet clear, but it could happen
Weeks since randomisation because of early administration of the inhaled
corticosteroid, given as part of the rescue treatment, at the
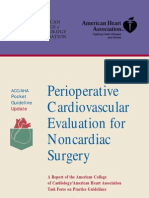
Figure 3: Number of severe asthma exacerbations needing medical intervention (oral or systemic time of worsening asthma control.
corticosteroid treatment) over 1 year in the STAY study
BUD=budesonide. Form=formoterol. SABA=short-acting inhaled β2 agonist Every exacerbation is represented by a The cost-effectiveness of using combinations of inhaled
line. The first exacerbation is the upper line and any subsequent event a patient had is recorded below. *Rate corticosteroids and long-acting β2 agonists to treat
reduction 46% to 53% versus both groups; p<0·001. moderate persistent asthma has been investigated.49–51
798 www.thelancet.com Vol 368 August 26, 2006
Review
A B
Figure 4: Induced sputum specimens from patients with eosinophilic airway inflammation (A) or neutrophilic airway inflammation (B)
Magnification is ×40 (A) and ×25 (B).
Findings have shown improved effectiveness at partial or bronchitis (figure 4). Occasionally, no cellular
complete offset of costs or at modest additional cost. inflammation will be present.57 Eosinophilic bronchitis is
Although addition of a long-acting β2 agonist to inhaled steroid responsive,58 whereas non-eosinophilic bronchitis
corticosteroids improves clinically relevant outcomes in is usually not.59 In the same patient, the nature of
most patients with moderate asthma more so than inflammation can change with time depending on the
further increases in dose of inhaled corticosteroid,52 the cause of the exacerbation. For example, an exacerbation
size of benefit is reduced in people with severe asthma. due to allergen exposure or reduction of dose of inhaled
This finding is highlighted in a meta-analysis,53 in which corticosteroid is usually eosinophilic and responds to an
researchers described that the combination of long-acting increase in dose of the inhaled drug; addition of a long-
β2 agonists and inhaled corticosteroids resulted in acting β2 agonist is not necessary. Long-acting β2
greater improvement in lung function and symptoms agonists become effective for management of symptoms
when compared with a 2–2·5-fold higher dose of inhaled if the individual continues to be hyper-responsive despite
corticosteroids. However, in 15 trials in which outcomes adequate control of eosinophilic inflammation.
of exacerbation were reported, no group difference was Eosinophilic bronchitis in an asymptomatic patient is
recorded (2% [95% CI 0–4]) in absolute risk of patients predictive of an exacerbation60 and therefore needs to be
having moderate exacerbations. Authors of this meta- suppressed by boosting the dose of inhaled corticosteroid.
analysis did not look at the differences between formoterol While trying to work out the minimum dose of inhaled
and salmeterol as add-on treatments. Nevertheless, this corticosteroid for an individual, maintaining the dose in
analysis points out that, despite our current best a patient whose asthma is well controlled would be
strategies, many patients do not have well controlled prudent if the eosinophil count is greater than 2%.61 An
asthma. Therefore, other approaches to improve asthma exacerbation due to a viral or bacterial infection is usually
control in these individuals need to be investigated. neutrophilic. A viral infection resolves spontaneously
with supportive additional treatment with a short-acting
Use of biomarkers to guide treatment of or long-acting bronchodilator; increasing doses of inhaled
moderate asthma corticosteroids are not necessary and are usually not
Markers of inflammation could help to guide use of anti- effective. A bacterial infection requires an antibiotic.
inflammatory treatment. Currently, two tests are available Researchers on two randomised clinical trials tested the
clinically: total and differential cell counts in sputum54 principles of individualised treatment by comparing this
and fraction of nitric oxide in exhaled breath55 are both strategy of asthma management with approaches based
reliable and reproducible. Normal values for sputum cell on national guidelines. In one trial, 74 patients with
counts have been established,56 and this method provides asthma were randomly assigned either a management
the most direct and fairly non-invasive assessment of strategy aimed at maintaining their sputum eosinophil
airway inflammation. Sputum cell counts help to identify count below 3% or standard clinical care based on the
whether exacerbations of asthma are associated with British Thoracic Society’s guidelines.62 Individuals in the
eosinophilic, neutrophilic, or a combined pattern of sputum management group had significantly fewer
www.thelancet.com Vol 368 August 26, 2006 799
Review
severe asthma exacerbations than those in the standard
care group, and significantly fewer participants were 100
Sputum strategy
Proportion free of exacerbation (%)
admitted to hospital with asthma. The reduction in Conventional strategy
80
exacerbations was achieved without an increase in total
corticosteroid dose in the sputum group. In a larger 60 p=0·04
multicentre Canadian study, 107 patients were randomly
assigned either clinical guideline-based treatment or a 40
strategy to maintain sputum eosinophils below 2% after
establishing the minimum treatment to maintain 20
control.63 Primary outcomes were relative risk reduction
0
for occurrence of the first exacerbation and length of time 0 100 200 300 400 500 600 700 800
without exacerbation. Compared with participants in the Days from maintenance
guideline-based group, patients allocated sputum Number at risk
management had longer time to first exacerbation (by
Sputum strategy 48 41 38 33 27 20 13 5 0
213 days), lower relative risk reduction (by 49%; figure 5),
Conventional 52 42 33 26 19 16 12 9 0
and fewer exacerbations needing prednisone (5 vs 15). strategy
This benefit was seen mainly in patients needing
treatment with inhaled steroid in a daily dose equivalent Figure 5: Kaplan-Meier survival curve of patients free of asthma
to fluticasone 250 μg. The cumulative dose of inhaled exacerbations over 2 years in the Canadian study63
corticosteroid during the trial was similar in both groups. several cells in the airway, notably airway epithelium, and
Reduction of non-eosinophilic exacerbations and are non-specific. The fraction of exhaled nitric oxide can
lengthening of time free of exacerbation by treatment also rise with non-eosinophilic bronchitis. In a randomised
with a long-acting β2 agonist were outcomes seen only in controlled trial, investigators looked at whether amounts
the sputum strategy arm. Since these events were not of exhaled nitric oxide could be used to guide asthma
recorded in patients receiving a long-acting β2 agonist in treatment.69 97 patients with mild to moderate asthma
the clinical strategy, possibly, when eosinophilic were randomly allocated to one of two strategies, whereby
inflammation is under control, this drug might prevent dose of inhaled corticosteroid was adjusted every 4 weeks
deterioration of asthma caused by a viral or bacterial to either keep the fraction of nitric oxide in exhaled breath
infection. However, this analysis was secondary and needs at less than 15 ppb or to prevent loss of asthma control as
prospective assessment. Use of strategies such as sputum defined by Global Initiative for Asthma guidelines. Rates
cell counts seems prudent to limit administration of of exacerbation did not differ between the two groups.
additional drugs to patients whose variability in airflow However, the nitric oxide strategy enabled a significant
obstruction and airway hyper-responsiveness are reduction in the maintenance dose of inhaled
uncontrolled despite adequate control of their eosinophilic corticosteroid. Whether a raised fraction of exhaled nitric
bronchitis. Also, whether dose-titration of corticosteroids oxide in asymptomatic patients needs any treatment
to completely abolish luminal (or tissue) eosinophils action is not clear. Thus, although the measurement is
would further improve asthma outcomes remains to be easy to use, especially in children, its precise role in
seen. Although the contribution of airway eosinophils to improving treatment of moderate asthma needs further
asthma exacerbations is arguable, their measurement has assessment, particularly when it is associated with non-
consistently been proven to be beneficial in guiding eosinophilic bronchitis.
asthma treatment. The sputum strategy was not superior
to clinical guideline-based therapy in patients with mild Other treatments
asthma and therefore is probably not necessary. In several studies, researchers have investigated clinical
A raised fraction of nitric oxide in exhaled breath is benefit when leukotriene receptor antagonists are added
associated with loss of asthma control during reductions to inhaled corticosteroids in adults and children with
in dose of inhaled corticosteroids64 and correlates moderate persistent asthma. However, authors of a meta-
moderately with eosinophilic bronchitis.65 Titration of the analysis of benefits achieved have concluded that addition
dose of inhaled corticosteroids based on measurements of these drugs to inhaled corticosteroids might modestly
of the fraction of exhaled nitric oxide in children is improve asthma control compared with inhaled
associated with improvements in airway hyper- corticosteroids alone, but this strategy cannot be
responsiveness.66 However, this measure is less able to recommended as a substitute for increasing the dose of
discriminate eosinophilic from non-eosinophilic airway inhaled corticosteroids.70 Furthermore, leukotriene
inflammation in patients receiving inhaled receptor antagonists have been shown to be less effective
corticosteroids.67 The fraction of nitric oxide in exhaled than long-acting β2 agonists when combined with inhaled
breath typically falls before airway eosinophilia is corticosteroids.71
controlled.68 Also, exhaled nitric oxide concentrations Data for the effectiveness of immunotherapy in patients
indicate activity of the nitric oxide synthase enzyme in with moderate asthma are scarce. Hence, no firm
800 www.thelancet.com Vol 368 August 26, 2006
Review
conclusions can be drawn or recommendations made on compared with best pharmacological treatment for
such an approach for patients who need a moderate dose reduction of asthma exacerbations (currently a combination
of inhaled corticosteroids to maintain symptom control. of inhaled corticosteroid and long-acting β2 agonist) has
Low-dose theophylline has also been assessed as add-on not been assessed.
therapy to inhaled corticosteroids.72 The size of benefit
achieved is less than for long-acting β2 agonists. Another Conclusions
potential treatment option for patients with moderate Most patients with asthma have mild intermittent and
asthma is omalizumab, which is a recombinant humanised persistent disease. Those with mild persistent asthma
monoclonal antibody against IgE. This anti-IgE forms are usually not well controlled. Low doses of inhaled
complexes with free IgE, thus blocking the interaction corticosteroids can generally provide ideal disease control
between the immunoglobulin and effecter cells, decreases and reduce risk for severe asthma exacerbations in both
concentrations of free IgE in serum, and thus lessens early children and adults. Intermittent inhaled corticosteroid
and late asthmatic responses after allergen inhalation.73 treatment at the time of an exacerbation has also been
When compared with placebo in patients on moderate-to- suggested as a strategy for mild persistent asthma, but it
high doses of inhaled corticosteroids, omalizumab reduced is less effective than low-dose regular treatment for most
asthma exacerbations and enabled a small decline in dose outcomes. Leukotriene receptor antagonists are another
of inhaled corticosteroid.74 However, this drug is expensive treatment option for this population, but they are also
and it has not been compared with proven additive less effective than low-dose inhaled corticosteroids.
treatments such as long-acting β2 agonists, which are Patients with moderate persistent asthma can be
cheaper. Therefore, this strategy is not currently regarded as those who are not ideally controlled on low-
recommended in international guidelines for patients dose inhaled corticosteroids. In adults, the combination
with moderate asthma. of a corticosteroid and long-acting β2 agonist (usually in
one inhaler) is better than doubling the dose of inhaled
Future research directions corticosteroid to achieve better asthma control and reduce
Despite abundant evidence that currently available exacerbation risks. In children, much less evidence is
treatments are very effective and can provide good asthma available that a combination is more effective than an
control for most patients with mild or moderate persistent increased dose of inhaled corticosteroid. One of the
asthma, several important issues still need to be clarified combinations available to treat asthma (budesonide and
about pharmacological management. In a few studies, formoterol) has also been assessed as both maintenance
researchers have shown that individuals with asthma lose and rescue therapy. This approach further reduces risks
lung function at a greater rate than non-smoking healthy for severe exacerbations. If asthma control is not
people,1,75 and this finding has been corroborated in achieved despite the patient taking effective treatment,
children and adults with newly diagnosed, mild asthma.76 measurement of the inflammatory response in the airway
Early intervention with inhaled corticosteroids reduces, in sputum or exhaled breath might be helpful to guide
but does not prevent, this accelerated decline in lung management. Allergen immunotherapy and cytokine-
function.16 The effect of other anti-asthma drugs (eg, anti- targeted treatment and monoclonal antibodies are not
leukotrienes) has not been assessed for this issue. routinely indicated, but might be effective in selected
Moreover, we do not yet know how early to begin anti- patients. Pharmacotherapy should always be accompanied
inflammatory treatment in asthma patients. Whereas by patient’s education about the disease and use of
inhaled corticosteroids do not seem to prevent development inhalers and allergen avoidance (when indicated) and a
of asthma in at-risk infants,28 the potential for anti- written management plan.
leukotrienes, which can reduce allergen-induced airway Conflict of interest statement
eosinophilia,34 bone-marrow eosinophil production,34 and POB is a consultant for, has received speaker’s fees from, or holds grants-
dendritic-cell trafficking,78 to do so is unknown. Also, as far in-aid from Altana, AstraZeneca, Biolipox, Boehringer, GlaxoSmithKline,
IVAX, and Topigen in the past 2 years. He does not own any shares,
as we know, no studies have assessed the benefits of anti- stocks, or options in any company. KP holds grants-in-aid from
inflammatory treatment in mild intermittent asthma. GlaxoSmithKline and Sepracor for investigator-initiated studies and has
Lastly, the goal of individualising treatment on the basis of received honoraria from Merck, Altana, and AstraZeneca in the past
pharmacogenetics—that is, identification of the best 2 years for lectures. He does not own any shares, stocks or options in any
company. He did not receive any fees for contributing to this article.
treatment option based on knowledge of a patient’s
genotype or of the inflammatory state of their airway—is Acknowledgments
KP is supported by a Canada research chair in airway regulation and
an important area for current and future research. Already, inflammation.
findings have suggested that patients with an Arg-Arg
References
polymorphism at position 16 of the β2 receptor could be at 1 Global Initiative for Asthma. Global strategy for asthma
greater risk of adverse effects from regular use of β2 management and prevention: NIH publication no 02-3659, updated
agonists,79 and changing treatment based on control of 2004. Available at: www.ginasthma.org.
2 Lemiere C, Bai TR, Balter M, et al. Adult asthma consensus
airway eosinophils can reduce asthma exacerbations;62,63 guidelines update 2003. Can Respir J 2004; 11 (suppl A):
however, the relative effectiveness of this approach 9A–18A.
www.thelancet.com Vol 368 August 26, 2006 801
Review
3 Cockcroft DW, Swystun VA. Asthma control versus asthma severity. 27 The Childhood Asthma Management Plan research group. Long-
J Allergy Clin Immunol 1996; 98: 1016–18. term effects of budesonide or nedocromil in children with asthma.
4 Turner-Warwick M. Nocturnal asthma: a study in general practice. N Engl J Med 2000; 343: 1054–63.
J R Coll Gen Pract 1989; 39: 239–43. 28 Guilbert TW, Morgan WJ, Zeiger RS, et al. Long-term inhaled
5 Rabe KF, Vermeire PA, Soriano JB, Maier WC. Clinical corticosteroids in preschool children at high risk for asthma.
management of asthma in 1999: the Asthma Insights and Reality in N Engl J Med 2006; 354: 1985–97.
Europe (AIRE) study. Eur Respir J 2000; 16: 802–07. 29 Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F.
6 Rabe KF, Adachi M, Lai CK, et al. Worldwide severity and control of Intermittent inhaled corticosteroids in infants with episodic
asthma in children and adults: the global asthma insights and wheezing. N Engl J Med 2006; 354: 1998–2005.
reality surveys. J Allergy Clin Immunol 2004; 114: 40–47. 30 Pedersen S, O’Byrne P. A comparison of the efficacy and safety
7 Chapman KR, Ernst P, Grenville A, Dewland P, Zimmerman S. of inhaled corticosteroids in asthma. Allergy 1997; 52 (39 suppl):
Control of asthma in Canada: failure to achieve guideline targets. 1–34.
Can Respir J 2001; 8 (suppl A): 35A–40A. 31 Agertoft L, Pedersen S. Effect of long-term treatment with inhaled
8 Kwok MY, Walsh-Kelly CM, Gorelick MH, Grabowski L, Kelly KJ. budesonide on adult height in children with asthma. N Engl J Med
National Asthma Education and Prevention Program severity 2000; 343: 1064–69.
classification as a measure of disease burden in children with acute 32 Bacharier LB, Raissy HH, Wilson L, McWilliams B, Strunk RC,
asthma. Pediatrics 2006; 117: S71–77. Kelly HW. Long-term effect of budesonide on hypothalamic-
9 Pearlman DS, Berger WE, Kerwin E, LaForce C, Kundu S, pituitary-adrenal axis function in children with mild to moderate
Banerji D. Once-daily ciclesonide improves lung function and is asthma. Pediatrics 2004; 113: 1693–99.
well tolerated by patients with mild-to-moderate persistent asthma. 33 Drazen JM, Israel E, O’Byrne PM. Treatment of asthma with drugs
J Allergy Clin Immunol 2005; 116: 1206–12. modifying the leukotriene pathway. N Engl J Med 1999; 340:
10 Pearlman DS, Peden D, Condemi JJ, et al. Efficacy and safety of 197–206.
fluticasone propionate/salmeterol HFA 134A MDI in patients with 34 Parameswaran K, Watson R, Gauvreau GM, Sehmi R, O’Byrne PM.
mild-to-moderate persistent asthma. J Asthma 2004; 41: 797–806. The effect of pranlukast on allergen-induced bone marrow
11 Israel E, Rubin P, Kemp JP, et al. The effect of inhibition of eosinophilopoiesis in subjects with asthma.
5-lipoxygenase by zileuton in mild- to moderate asthma. Am J Respir Crit Care Med 2004; 169: 915–20.
Ann Intern Med 1993; 119: 1059–66. 35 Zeiger RS, Szefler SJ, Phillips BR, et al. Response profiles to
12 Vaquerizo MJ, Casan P, Castillo J, et al. Effect of montelukast added fluticasone and montelukast in mild-to-moderate persistent
to inhaled budesonide on control of mild to moderate asthma. childhood asthma. J Allergy Clin Immunol 2006; 117: 45–52.
Thorax 2003; 58: 204–10. 36 Harrison TW, Oborne J, Newton S, Tattersfield AE. Doubling the
13 Chanez P, Karlstrom R, Godard P. High or standard initial dose of dose of inhaled corticosteroid to prevent asthma exacerbations:
budesonide to control mild-to-moderate asthma? Eur Respir J 2001; randomised controlled trial. Lancet 2004; 363: 271–75.
17: 856–62. 37 Garrett J, Williams S, Wong C, Holdaway D. Treatment of acute
14 Rabe KF, Pizzichini E, Stallberg B, et al. Budesonide/formoterol in asthmatic exacerbations with an increased dose of inhaled steroid.
a single inhaler for maintenance and relief in mild-to-moderate Arch Dis Child 1998; 79: 12–17.
asthma: a randomized, double-blind trial. Chest 2006; 129: 246–56. 38 Fitzgerald JM, Becker A, Sears MR, Mink S, Chung K, Lee J.
15 O’Byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose Doubling the dose of budesonide versus maintenance treatment in
inhaled budesonide and formoterol in mild persistent asthma: the asthma exacerbations. Thorax 2004; 59: 550–56.
OPTIMA randomized trial. Am J Respir Crit Care Med 2001; 164: 39 Zetterstrom O, Buhl R, Mellem H, et al. Improved asthma control
1392–97. with budesonide/formoterol in a single inhaler, compared with
16 Pauwels RA, Pedersen S, Busse WW, et al. Early intervention with budesonide alone. Eur Respir J 2001; 18: 262–68.
budesonide in mild persistent asthma: a randomised, double-blind 40 O’Byrne PM, Bisgaard H, Godard PP, et al. Budesonide/formoterol
trial. Lancet 2003; 361: 1071–76. combination therapy as both maintenance and reliever medication
17 Boushey HA, Sorkness CA, King TS, et al. Daily versus as-needed in asthma. Am J Respir Crit Care Med 2005; 171: 129–36.
corticosteroids for mild persistent asthma. N Engl J Med 2005; 352: 41 Bateman ED, Boushey HA, Bousquet J, et al. Can guideline-defined
1519–28. asthma control be achieved? The gaining optimal asthma control
18 Zeiger RS, Bird SR, Kaplan MS, et al. Short-term and long-term study. Am J Respir Crit Care Med 2004; 170: 836–44.
asthma control in patients with mild persistent asthma receiving 42 Bisgaard H. Effect of long-acting beta2 agonists on exacerbation
montelukast or fluticasone: a randomized controlled trial. rates of asthma in children. Pediatr Pulmonol 2003; 36: 391–98.
Am J Med 2005; 118: 649–57. 43 Nelson HS, Weiss ST, Bleeker ER, Yancey SW, Dorinsky PM, and
19 Garcia Garcia ML, Wahn U, Gilles L, Swern A, Tozzi CA, Polos P. the SMART study group. The Salmeterol Multicenter Asthma
Montelukast, compared with fluticasone, for control of asthma Research Trial: a comparison of usual pharmacotherapy for asthma
among 6 to 14-year-old patients with mild asthma: the MOSAIC or usual pharmacotherapy plus salmeterol. Chest 2006; 129: 15–26.
study. Pediatrics 2005; 116: 360–69. 44 Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide
20 Shepherd GL, Hetzel MR, Clark TJ. Regular versus symptomatic surveillance study: comparison of salmeterol with salbutamol in
aerosol bronchodilator treatment of asthma. Br J Dis Chest 1981; 75: asthmatic patients who require regular bronchodilator treatment.
215–17. BMJ 1993; 306: 1034–37.
21 Sears MR, Taylor DR, Print CG, et al. Regular inhaled beta-agonist 45 Scicchitano R, Aalbers R, Ukena D, et al. Efficacy and safety of
treatment in bronchial asthma. Lancet 1990; 336: 1391–96. budesonide/formoterol single inhaler therapy versus a higher dose
22 Crane J, Pearce N, Flatt A, et al. Prescribed fenoterol and death of budesonide in moderate to severe asthma. Curr Med Res Opin
from asthma in New Zealand, 1981–83: case-control study. Lancet 2004; 20: 1403–18.
1989; 1: 917–22. 46 Palmqvist M, Ibsen T, Mellen A, Lotvall J. Comparison of the
23 Barnes PJ, Pedersen S, Busse WW. Efficacy and safety of inhaled relative efficacy of formoterol and salmeterol in asthmatic patients.
corticosteroids: new developments. Am J Respir Crit Care Med 1998; Am J Respir Crit Care Med 1999; 160: 244–49.
157: S1–53. 47 Anderson GP. Formoterol: pharmacology, molecular basis of
24 Greening AP, Ind PW, Northfield M, Shaw G. Added salmeterol agonism, and mechanism of long duration of a highly potent and
versus higher-dose corticosteroid in asthma patients with symptoms selective beta 2-adrenoceptor agonist bronchodilator. Life Sci 1993;
on existing inhaled corticosteroid. Lancet 1994; 344: 219–24. 52: 2145–60.
25 Pauwels RA, Lofdahl CG, Postma DS, et al. Effect of inhaled 48 Ind PW, Villasante C, Shiner RJ, et al. Safety of formoterol by
formoterol and budesonide on exacerbations of asthma. Turbuhaler (R) as reliever medication compared with terbutaline in
N Engl J Med 1997; 337: 1405–11. moderate asthma. Eur Respir J 2002; 20: 859–66.
26 Woolcock AJ, Lundback B, Ringdal N, Jacques LA. Comparison of 49 Briggs AH, Bousquet J, Wallace MV, et al. Cost-effectiveness of
addition of salmeterol to inhaled steroids with doubling of the dose asthma control: an economic appraisal of the GOAL study. Allergy
of inhaled steroids. Am J Respir Crit Care Med 1996; 153: 1481–88. 2006; 61: 531–36.
802 www.thelancet.com Vol 368 August 26, 2006
Review
50 Andersson F, Stahl E, Barnes PJ, et al. Adding formoterol to 65 Jones SL, Kittelson J, Cowan JO, et al. The predictive value of
budesonide in moderate asthma: health economic results from the exhaled nitric oxide measurements in assessing changes in asthma
FACET study. Respir Med 2001; 95: 505–12. control. Am J Respir Crit Care Med 2001; 164: 738–43.
51 Jonsson B, Berggren F, Svensson K, O’Byrne PM. An economic 66 Pijnenburg MW, Bakker EM, Hop WC, de Jongste JC. Titrating
evaluation of combination treatment with budesonide and steroids on exhaled nitric oxide in children with asthma: a
formoterol in patients with mild-to-moderate persistent asthma. randomized controlled trial. Am J Respir Crit Care Med 2005; 172:
Respir Med 2004; 98: 1146–54. 831–36.
52 Masoli M, Weatherall M, Holt S, Beasley R. Moderate dose inhaled 67 Berlyne GS, Parameswaran K, Kamada D, Efthimiadis A, Hargreave
corticosteroids plus salmeterol versus higher doses of inhaled FE. A comparison of exhaled nitric oxide and induced sputum as
corticosteroids in symptomatic asthma. Thorax 2005; 60: 730–34. markers of airway inflammation. J Allergy Clin Immunol 2000; 106:
53 Ni CM, Greenstone IR, Ducharme FM. Addition of inhaled long- 638–44.
acting beta2-agonists to inhaled steroids as first line therapy for 68 Lim S, Jatakanon A, Meah S, Oates T, Chung KF, Barnes PJ.
persistent asthma in steroid-naive adults. Relationship between exhaled nitric oxide and mucosal eosinophilic
Cochrane Database Syst Rev 2005; 2: CD005307. inflammation in mild to moderately severe asthma. Thorax 2000;
54 Djukanovic R, Sterk PJ, Fahy JV, Hargreave FE. Standardised 55: 184–88.
methodology of sputum induction and processing. 69 Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of
Eur Respir J Suppl 2002; 37: 1s–2s. exhaled nitric oxide measurements to guide treatment in chronic
55 American Thoracic Society, European Respiratory Society. ATS/ERS asthma. N Engl J Med 2005; 352: 2163–73.
recommendations for standardized procedures for the online and 70 Ducharme FM. Anti-leukotrienes as add-on therapy to inhaled
offline measurement of exhaled lower respiratory nitric oxide and glucocorticoids in patients with asthma: systematic review of
nasal nitric oxide, 2005. Am J Respir Crit Care Med 2005; 171: current evidence. BMJ 2002; 324: 1545.
912–30. 71 Nelson HS, Busse WW, Kerwin E, et al. Fluticasone
56 Belda J, Leigh R, Parameswaran K, O’Byrne PM, Sears MR, propionate/salmeterol combination provides more effective asthma
Hargreave FE. Induced sputum cell counts in healthy adults. control than low-dose inhaled corticosteroid plus montelukast.
Am J Respir Crit Care Med 2000; 161: 475–78. J Allergy Clin Immunol 2000; 106: 1088–95.
57 Simpson JL, Scott R, Boyle MJ, Gibson PG. Inflammatory subtypes 72 Evans DJ, Taylor DA, Zetterstrom O, Chung KF, O’Connor BJ,
in asthma: assessment and identification using induced sputum. Barnes PJ. A comparison of low-dose inhaled budesonide plus
Respirology 2006; 11: 54–61. theophylline and high-dose inhaled budesonide for moderate
58 Kelly MM, Leigh R, Jayaram L, Goldsmith CH, Parameswaran K, asthma. N Engl J Med 1997; 337: 1412–18.
Hargreave FE. Eosinophilic bronchitis in asthma: a model for 73 Fahy JV, Fleming HE, Wong HH, et al. The effect of an anti-IgE
establishing dose-response and relative potency of inhaled monoclonal antibody on the early- and late-phase responses to
corticosteroids. J Allergy Clin Immunol 2006; 117: 989–94. allergen inhalation in asthmatic subjects. Am J Respir Crit Care Med
59 Green RH, Brightling CE, Woltmann G, Parker D, Wardlaw AJ, 1997; 155: 1828–34.
Pavord ID. Analysis of induced sputum in adults with asthma: 74 Walker S, Monteil M, Phelan K, Lasserson TJ, Walters EH. Anti-IgE
identification of subgroup with isolated sputum neutrophilia and for chronic asthma in adults and children.
poor response to inhaled corticosteroids. Thorax 2002; 57: 875–79. Cochrane Database Syst Rev 2006; 2: CD003559.
60 Jatakanon A, Lim S, Barnes PJ. Changes in sputum eosinophils 75 Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-
predict loss of asthma control. Am J Respir Crit Care Med 2000; 161: up study of ventilatory function in adults with asthma. N Engl J Med
64–72. 1998; 339: 1194–200.
61 Belda J, Parameswaran K, Lemiere C, Kamada D, O’Byrne PM, 76 O’Byrne PM, Pedersen S, Busse WW, et al. Effects of early
Hargreave FE. Predictors of loss of asthma control induced by intervention with inhaled budesonide on lung function in newly
corticosteroid withdrawal. Can Respir J 2006; 13: 129–33. diagnosed asthma. Chest 2006; 129: 1478–85.
62 Green RH, Brightling CE, McKenna S, et al. Asthma exacerbations 77 Leigh R, Vethanayagam D, Yoshida M, et al. Effects of montelukast
and sputum eosinophil counts: a randomised controlled trial. and budesonide on airway responses and airway inflammation in
Lancet 2002; 360: 1715–21. asthma. Am J Respir Crit Care Med 2002; 166: 1212–17.
63 Jayaram L, Pizzichini MM, Cook RJ, et al. Determining asthma 78 Parameswaran K, Liang H, Fanat A, Watson R, Snider DP,
treatment by monitoring sputum cell counts: effect on O’Byrne PM. Role for cysteinyl leukotrienes in allergen-induced
exacerbations. Eur Respir J 2006; 27: 483–94. change in circulating dendritic cell number in asthma.
64 Zacharasiewicz A, Wilson N, Lex C, et al. Clinical use of J Allergy Clin Immunol 2004; 114: 73–79.
noninvasive measurements of airway inflammation in steroid 79 Israel E, Chinchilli VM, Ford JG, et al. Use of regularly scheduled
reduction in children. Am J Respir Crit Care Med 2005; albuterol treatment in asthma: genotype-stratified, randomised,
171: 1077–82. placebo-controlled cross-over trial. Lancet 2004; 364: 1505–12.
www.thelancet.com Vol 368 August 26, 2006 803
Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Symbicort Branding Manual PDFDokument79 SeitenSymbicort Branding Manual PDFMauricio Gómez100% (1)
- National GeographicDokument150 SeitenNational GeographicKonna_M100% (6)
- Valvular Pocket GuideDokument64 SeitenValvular Pocket Guideapi-3826574100% (5)
- Respiratory MCQDokument10 SeitenRespiratory MCQSyeda Aroosa Abbas Naqvi100% (1)
- Drugs For AsthmaDokument3 SeitenDrugs For AsthmaMelissa Deso MillerNoch keine Bewertungen
- Drug Study (Seretide)Dokument1 SeiteDrug Study (Seretide)Rene John Francisco100% (1)
- Chapter 29: Nursing Management: Obstructive Pulmonary Diseases Test BankDokument15 SeitenChapter 29: Nursing Management: Obstructive Pulmonary Diseases Test BankBriseidaSolisNoch keine Bewertungen
- Inhaler Chart 2016 PDFDokument2 SeitenInhaler Chart 2016 PDFAlmas TalidaNoch keine Bewertungen
- Bronchial AsthmaDokument43 SeitenBronchial AsthmaAmar BimavarapuNoch keine Bewertungen
- Hi Per Nat Re MiaDokument7 SeitenHi Per Nat Re Miaapi-3826574Noch keine Bewertungen
- Consenso Valvopatias 2006Dokument81 SeitenConsenso Valvopatias 2006api-3826574100% (1)
- Guia Bolso GoldDokument16 SeitenGuia Bolso Goldapi-3826574Noch keine Bewertungen
- Choque SépticoDokument12 SeitenChoque Sépticoapi-3826574Noch keine Bewertungen
- Mia - Correção Por Hip Erg Lice MiaDokument5 SeitenMia - Correção Por Hip Erg Lice Miaapi-3826574Noch keine Bewertungen
- Tep Pioped IIDokument11 SeitenTep Pioped IIapi-3826574100% (2)
- Lancet 2006 - Astha MechanismsDokument14 SeitenLancet 2006 - Astha Mechanismsapi-3826574100% (1)
- AAS Review 2005Dokument11 SeitenAAS Review 2005api-3826574Noch keine Bewertungen
- Hip On at Re MiaDokument9 SeitenHip On at Re Miaapi-3826574Noch keine Bewertungen
- ClarityDokument11 SeitenClarityapi-3826574100% (1)
- Valvulopatias PocketDokument26 SeitenValvulopatias Pocketapi-3826574100% (1)
- Difficult WeaningDokument7 SeitenDifficult Weaningapi-3826574Noch keine Bewertungen
- CSAP Full 2002Dokument125 SeitenCSAP Full 20022012Noch keine Bewertungen
- Acca Ha Pocket Guidelines Table APDokument28 SeitenAcca Ha Pocket Guidelines Table APD'woel WulandariNoch keine Bewertungen
- Unstable PKTDokument19 SeitenUnstable PKTapi-3826574Noch keine Bewertungen
- Arritmias SupraventricularesDokument62 SeitenArritmias Supraventricularesapi-3826574Noch keine Bewertungen
- ValvopatiasDokument97 SeitenValvopatiasapi-3826574Noch keine Bewertungen
- Acc-Aha - Full Text) Unstable Anghina and Non-St AmiDokument93 SeitenAcc-Aha - Full Text) Unstable Anghina and Non-St Amiapi-3765169Noch keine Bewertungen
- Avaliação Pré Operatóia PocketDokument24 SeitenAvaliação Pré Operatóia Pocketapi-3826574Noch keine Bewertungen
- Asma NEJMDokument13 SeitenAsma NEJMAlba RNoch keine Bewertungen
- BronchodilatorDokument2 SeitenBronchodilatormelaniNoch keine Bewertungen
- Astm Bronsic Diagnostic Si Management PDFDokument50 SeitenAstm Bronsic Diagnostic Si Management PDFAlina GheNoch keine Bewertungen
- Seretid Discus PDFDokument4 SeitenSeretid Discus PDFRisma ApriliantiNoch keine Bewertungen
- Group 1 Case Study Chapter 24Dokument10 SeitenGroup 1 Case Study Chapter 24Doneva Lyn MedinaNoch keine Bewertungen
- Questions: Chronic Obstructive Pulmonary DiseaseDokument4 SeitenQuestions: Chronic Obstructive Pulmonary DiseaseAnis Hikmah SyabanaNoch keine Bewertungen
- 2014 Revision de EPOCDokument11 Seiten2014 Revision de EPOCjgcardNoch keine Bewertungen
- Seretide: What Is in This LeafletDokument6 SeitenSeretide: What Is in This LeafletJazmaine Karyle ChuaNoch keine Bewertungen
- 26.pulmonary PharmacologyDokument14 Seiten26.pulmonary PharmacologyAnggreany AshariNoch keine Bewertungen
- Presented By: Fatin Amirah Azhar DPM 11/12ADokument19 SeitenPresented By: Fatin Amirah Azhar DPM 11/12AJunainahNoch keine Bewertungen
- NAME of DRUG Generic Name: Salmeterol Xinafoate Classification: Beta2-SelectiveDokument2 SeitenNAME of DRUG Generic Name: Salmeterol Xinafoate Classification: Beta2-SelectiveBianca Camille100% (2)
- COPDSwissguidelinesDokument16 SeitenCOPDSwissguidelinesNurul Kamilah SadliNoch keine Bewertungen
- Type 2 Diabetes Case Study Addressing Interacting ComorbiditiesDokument9 SeitenType 2 Diabetes Case Study Addressing Interacting ComorbiditiesJayr MartinNoch keine Bewertungen
- Approach Considerations: Respiratory Acidosis Treatment & ManagementDokument8 SeitenApproach Considerations: Respiratory Acidosis Treatment & Managementprince1500Noch keine Bewertungen
- AsthmaDokument10 SeitenAsthmaAcohCChaoNoch keine Bewertungen
- COPD 114554 Comparative Analysis of Budesonide Formoterol and Fluticason 110416Dokument7 SeitenCOPD 114554 Comparative Analysis of Budesonide Formoterol and Fluticason 110416RezaFArthaNoch keine Bewertungen
- Respiratory Agents.2015Dokument75 SeitenRespiratory Agents.2015sarwatNoch keine Bewertungen
- Platinum Formulary 2016Dokument61 SeitenPlatinum Formulary 2016jNoch keine Bewertungen
- Breo ElliptaDokument11 SeitenBreo ElliptamohammadNoch keine Bewertungen
- Market Survey Report For Beximco Pharma Eye Drops and InhalersDokument4 SeitenMarket Survey Report For Beximco Pharma Eye Drops and Inhalersmdgayas70Noch keine Bewertungen
- Drugs Acting On The Respiratory SystemDokument13 SeitenDrugs Acting On The Respiratory SystemAlloiBialbaNoch keine Bewertungen
- Nishant Respiratory SecondDokument10 SeitenNishant Respiratory SecondNishantNoch keine Bewertungen