Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Chapter IIDokument48 SeitenChapter IIBhavesh SutharNoch keine Bewertungen
- Coast Guard Public School, Daman: (Type Here)Dokument13 SeitenCoast Guard Public School, Daman: (Type Here)Rajeev SinghNoch keine Bewertungen
- Workshop Materials BookletDokument121 SeitenWorkshop Materials BookletlyrechaugustNoch keine Bewertungen
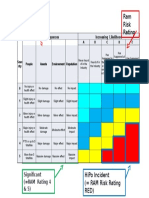
- RAM Revised For PR1418Dokument1 SeiteRAM Revised For PR1418rwerwerwNoch keine Bewertungen
- Breast CancerDokument9 SeitenBreast CancerFenty KaruniawatiNoch keine Bewertungen
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Neonates - UpToDateDokument32 SeitenClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Neonates - UpToDateMary Angela Baella GalvezNoch keine Bewertungen
- Fever PDFDokument3 SeitenFever PDFsubhanoopNoch keine Bewertungen
- Lecturas de ComprensiónDokument3 SeitenLecturas de ComprensiónValentinNoch keine Bewertungen
- Fiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1Dokument133 SeitenFiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1roddy narayanNoch keine Bewertungen
- 03 Worsheet 1-ArgDokument2 Seiten03 Worsheet 1-ArgDarlene AmadorNoch keine Bewertungen
- Vaccine IngredientsDokument7 SeitenVaccine IngredientsShoshannah100% (22)
- BenefitsDokument2 SeitenBenefitsThắng PhạmNoch keine Bewertungen
- Assessment of Risk For Gardening Activities Involving PupilsDokument5 SeitenAssessment of Risk For Gardening Activities Involving PupilsAj tanNoch keine Bewertungen
- Docit - Tips Contoh Manajemen Resikoxls Personal Protective EquipmentDokument12 SeitenDocit - Tips Contoh Manajemen Resikoxls Personal Protective EquipmentBambang SumantriNoch keine Bewertungen
- 2021.07.21 LWV Corpus Christi Lead Contamination in Drinking Water Study & Position Statement - NCDokument13 Seiten2021.07.21 LWV Corpus Christi Lead Contamination in Drinking Water Study & Position Statement - NCcallertimesNoch keine Bewertungen
- Essential Newborn CareDokument14 SeitenEssential Newborn CareJam Corros100% (1)
- Neonatal InfectionDokument18 SeitenNeonatal InfectionchinchuNoch keine Bewertungen
- Epi 3rd Exam ReviewerDokument93 SeitenEpi 3rd Exam ReviewerJillian AsdalaNoch keine Bewertungen
- Health Promotion and Primary Health Care PDFDokument34 SeitenHealth Promotion and Primary Health Care PDFKavya S Mohan100% (2)
- Concept Communicable DiseasesDokument477 SeitenConcept Communicable DiseasesrimeoznekNoch keine Bewertungen
- Problem Statement Chapter-1&2Dokument33 SeitenProblem Statement Chapter-1&2Anonymous 22GBLsme171% (7)
- Code of Ethics Medical ProfessionDokument8 SeitenCode of Ethics Medical ProfessionAustin CharlesNoch keine Bewertungen
- Model Answers Section A and Section BDokument13 SeitenModel Answers Section A and Section Baleezabilal19Noch keine Bewertungen
- Breastfeeding Problems and ManagementDokument28 SeitenBreastfeeding Problems and ManagementlzbthdukerNoch keine Bewertungen
- INFOSAN User Guide FinalDokument17 SeitenINFOSAN User Guide FinalJorge Gregorio SeguraNoch keine Bewertungen
- Clinical Features of DiarrhoeaDokument4 SeitenClinical Features of DiarrhoeaKhogen MairembamNoch keine Bewertungen
- Vambay - Slum RehabilitationDokument10 SeitenVambay - Slum RehabilitationsamairaNoch keine Bewertungen
- Case Study 1 RRLDokument4 SeitenCase Study 1 RRLMae Arra Lecobu-anNoch keine Bewertungen
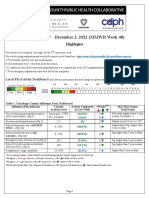
- 2022-23 Flu Surveillance Report - Week 48Dokument5 Seiten2022-23 Flu Surveillance Report - Week 48WKYC.comNoch keine Bewertungen
- What Is Microbial Contamination Types, Risk Factor, PreventionDokument1 SeiteWhat Is Microbial Contamination Types, Risk Factor, PreventionSukh RanaNoch keine Bewertungen