Das könnte Ihnen auch gefallen
- TOPIC 3 - The Endocrine SystemDokument34 SeitenTOPIC 3 - The Endocrine SystemKaren Pearl TagleNoch keine Bewertungen
- Oestrogen, Progesterone, AndrogensDokument58 SeitenOestrogen, Progesterone, AndrogensTandin SonamNoch keine Bewertungen
- 01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)Dokument46 Seiten01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)sahilaminNoch keine Bewertungen
- Endocrine SystemDokument30 SeitenEndocrine SystemYary MayorNoch keine Bewertungen
- Drugs Affecting Reproduction: DR - R - PrameelaDokument76 SeitenDrugs Affecting Reproduction: DR - R - PrameelaRamadi PrameelaNoch keine Bewertungen
- EstrogenDokument41 SeitenEstrogenShanty ManekNoch keine Bewertungen
- Progesterone in A NutshellDokument14 SeitenProgesterone in A NutshellkiyannNoch keine Bewertungen
- AndrogensDokument19 SeitenAndrogensMirza Shaharyar BaigNoch keine Bewertungen
- Hormones of The Reproductive SystemDokument9 SeitenHormones of The Reproductive Systemkarthickmech1987Noch keine Bewertungen
- Hormones and Related Drugs: Mechanism of ActionDokument21 SeitenHormones and Related Drugs: Mechanism of ActionaviraaworldNoch keine Bewertungen
- New Estrogen and ProgesteroneDokument56 SeitenNew Estrogen and ProgesteroneHBrNoch keine Bewertungen
- Sex HarmoneDokument22 SeitenSex Harmonesuyash jainNoch keine Bewertungen
- Female Sex HormonesDokument28 SeitenFemale Sex HormonesAbdimalik AliNoch keine Bewertungen
- Gonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologyDokument34 SeitenGonadal Hormones & Inhibitors Contraceptives: DR Dhoro Clinical PharmacologykelvinNoch keine Bewertungen
- Lecturio 3952Dokument11 SeitenLecturio 3952Pranjali WeladiNoch keine Bewertungen
- 1 EndocrinologyDokument15 Seiten1 EndocrinologyJessa MayNoch keine Bewertungen
- Drugs Used in Reproductive Health: Estrogen and ProgestinDokument41 SeitenDrugs Used in Reproductive Health: Estrogen and ProgestindrfatimarizNoch keine Bewertungen
- Drugs Acting On The Endocrine SystemDokument90 SeitenDrugs Acting On The Endocrine SystemKATHERINE GRACE JOSENoch keine Bewertungen
- Androgens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongDokument16 SeitenAndrogens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongAbhijeet BhagatNoch keine Bewertungen
- Endocrine SystemDokument14 SeitenEndocrine SystemNovie Jane HontiverosNoch keine Bewertungen
- Endocrine Physiology Lecture by Mrs M MUTSANGU POLY ND1Dokument56 SeitenEndocrine Physiology Lecture by Mrs M MUTSANGU POLY ND1letwinemwale02Noch keine Bewertungen
- Estrogen and ProgesteroneDokument45 SeitenEstrogen and Progesteronevinay0717Noch keine Bewertungen
- Steroids JenniferKettelDokument25 SeitenSteroids JenniferKettelvinay0717Noch keine Bewertungen
- Discussion Notes AnaphyDokument36 SeitenDiscussion Notes Anaphyjade tanNoch keine Bewertungen
- 1 Endocrinology 1Dokument14 Seiten1 Endocrinology 1Jessa MayNoch keine Bewertungen
- EstrDokument2 SeitenEstraviraaworldNoch keine Bewertungen
- Menopause Semester 6 (IMTU)Dokument37 SeitenMenopause Semester 6 (IMTU)nyangaraNoch keine Bewertungen
- Cortisol, Fixing ImbalancesDokument21 SeitenCortisol, Fixing ImbalancesTheresa Dale100% (2)
- 4th Block Endocrine PowerpointDokument70 Seiten4th Block Endocrine PowerpointKevinNoch keine Bewertungen
- Hormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraDokument40 SeitenHormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraGelo Robin JacosalemNoch keine Bewertungen
- Chapter 5Dokument6 SeitenChapter 5Shiny ChenNoch keine Bewertungen
- Male ReproDokument81 SeitenMale ReproNanda Hikma LestariNoch keine Bewertungen
- Hormone 1Dokument34 SeitenHormone 1Fan SmithNoch keine Bewertungen
- Bp503t Pcol Unit-VDokument46 SeitenBp503t Pcol Unit-VAakkkNoch keine Bewertungen
- Why Is My HRT Not Working Lauren ReidDokument6 SeitenWhy Is My HRT Not Working Lauren ReidConce RamirezNoch keine Bewertungen
- MS EndoDokument22 SeitenMS EndoFrechel Ann Landingin PedrozoNoch keine Bewertungen
- 1 - Endocrine 1 (Introduction) - MedicineDokument36 Seiten1 - Endocrine 1 (Introduction) - MedicineBHUWAN BASKOTANoch keine Bewertungen
- 2019 Gonadal Hormones-3Dokument197 Seiten2019 Gonadal Hormones-3Vishwajeet RaneNoch keine Bewertungen
- Endocrine SystemDokument10 SeitenEndocrine SystemPeej Reyes100% (1)
- Drugs On Reproductive System Physiology: N11 Pharmacology For NursesDokument2 SeitenDrugs On Reproductive System Physiology: N11 Pharmacology For NursesAlec Xavier MirandaNoch keine Bewertungen
- 3 EndocrinologyDokument4 Seiten3 EndocrinologyJessa MayNoch keine Bewertungen
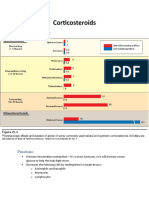
- CorticosteroidsDokument4 SeitenCorticosteroidsUsmanNoch keine Bewertungen
- Endocrine Pathophysiology Nursing NotesDokument4 SeitenEndocrine Pathophysiology Nursing Notesgrad_nurse_2015100% (2)
- Review in Science 3rd QuarterDokument8 SeitenReview in Science 3rd QuarterAyeisha ReyesNoch keine Bewertungen
- Andropause (Male Menopause) A Simple Guide To The Condition, Diagnosis And ManagementVon EverandAndropause (Male Menopause) A Simple Guide To The Condition, Diagnosis And ManagementNoch keine Bewertungen
- Male HormonesDokument30 SeitenMale Hormonesmjawadullah5Noch keine Bewertungen
- Estrogen EpidemicDokument14 SeitenEstrogen EpidemicDarmarsar100% (2)
- Hormon ReproDokument36 SeitenHormon Reproalvinrinaldi1101Noch keine Bewertungen
- S 040 LBLDokument9 SeitenS 040 LBLSykat ZamanNoch keine Bewertungen
- Sex Hormones PDFDokument54 SeitenSex Hormones PDFmohsen mirdamadiNoch keine Bewertungen
- Overview of The Endocrine SystemDokument9 SeitenOverview of The Endocrine SystemTAGUIAM, Danica A.Noch keine Bewertungen
- New Estrogen and ProgesteroneDokument39 SeitenNew Estrogen and ProgesteroneWegrimel AriegaraNoch keine Bewertungen
- General Biology Lesson 13Dokument13 SeitenGeneral Biology Lesson 13GUCOR, LOVELY SHANE C.Noch keine Bewertungen
- Gonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsDokument29 SeitenGonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsGopal Prasad DahalNoch keine Bewertungen
- Estrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongDokument24 SeitenEstrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongdrfatimarizNoch keine Bewertungen
- Progesterone in Orthomolecular Medicine by Ray PeatDokument66 SeitenProgesterone in Orthomolecular Medicine by Ray PeatJulian MiñoNoch keine Bewertungen
- Anatomy & Physiology Endocrine System: Ilah M, SKPDokument36 SeitenAnatomy & Physiology Endocrine System: Ilah M, SKPOmbun FajarNoch keine Bewertungen
- Endocrinology Excerpts: Hypothalamic-Pituitary-Adrenal AxisDokument9 SeitenEndocrinology Excerpts: Hypothalamic-Pituitary-Adrenal AxisKiana TehraniNoch keine Bewertungen
- EstorgenDokument34 SeitenEstorgenAbubakar JallohNoch keine Bewertungen
- Gonad Overview 2023 ADokument103 SeitenGonad Overview 2023 AElena Borş MorariNoch keine Bewertungen
- B0dfbaf2 Beed 4ca7 99fb Ff3588d75dc0Dokument3 SeitenB0dfbaf2 Beed 4ca7 99fb Ff3588d75dc0api-26938624Noch keine Bewertungen
- Diabetes Mellitus and HypoglycemiaDokument4 SeitenDiabetes Mellitus and Hypoglycemiaapi-26938624Noch keine Bewertungen
- Endocrine System IDokument2 SeitenEndocrine System Iapi-26938624Noch keine Bewertungen
- Endocrine System IVDokument3 SeitenEndocrine System IVapi-26938624Noch keine Bewertungen
- Endocrine System IIIDokument3 SeitenEndocrine System IIIapi-26938624Noch keine Bewertungen
- c1fd6bbd Ff7a 480d A20e C93bd3a3cedfDokument35 Seitenc1fd6bbd Ff7a 480d A20e C93bd3a3cedfapi-26938624Noch keine Bewertungen
- 13ffd1fa Eda0 4eb8 Bb3a 7802feec40daDokument40 Seiten13ffd1fa Eda0 4eb8 Bb3a 7802feec40daapi-26938624Noch keine Bewertungen
- Endorcine System IIDokument4 SeitenEndorcine System IIapi-26938624Noch keine Bewertungen
- Lecture 47 April 13th-EndocrineDokument1 SeiteLecture 47 April 13th-Endocrineapi-26938624Noch keine Bewertungen
- Lecture 50 April 20th-DiabetesDokument2 SeitenLecture 50 April 20th-Diabetesapi-26938624Noch keine Bewertungen
- Nervous System IIDokument2 SeitenNervous System IIapi-26938624Noch keine Bewertungen
- Lecture 46 April 11th-EndocrineDokument3 SeitenLecture 46 April 11th-Endocrineapi-26938624Noch keine Bewertungen
- Nervous System IDokument4 SeitenNervous System Iapi-26938624Noch keine Bewertungen
- Lecture 48 April 17th-Endocrine (Extra Class)Dokument4 SeitenLecture 48 April 17th-Endocrine (Extra Class)api-26938624Noch keine Bewertungen
- OP & OA ChartDokument3 SeitenOP & OA Chartapi-26938624100% (1)
- Lecture 49 April 18th-DiabetesDokument3 SeitenLecture 49 April 18th-Diabetesapi-26938624Noch keine Bewertungen
- Lecture 45 April 4th-EndocrineDokument2 SeitenLecture 45 April 4th-Endocrineapi-26938624Noch keine Bewertungen
- Lecture 43 March 28th-NervousDokument3 SeitenLecture 43 March 28th-Nervousapi-26938624Noch keine Bewertungen
- Lecture 39 March 9th-MSKDokument3 SeitenLecture 39 March 9th-MSKapi-26938624Noch keine Bewertungen
- Lecture 44 March 30th - NO NOTESDokument1 SeiteLecture 44 March 30th - NO NOTESapi-26938624Noch keine Bewertungen
- Lecture 42 March 23rd-NervousDokument2 SeitenLecture 42 March 23rd-Nervousapi-26938624Noch keine Bewertungen
- Lecture 41 March 16th-NervousDokument2 SeitenLecture 41 March 16th-Nervousapi-26938624Noch keine Bewertungen
- Conditions of The Musculoskeleltal SystemDokument4 SeitenConditions of The Musculoskeleltal Systemapi-26938624Noch keine Bewertungen
- Lecture 40 March 14th-MSKDokument5 SeitenLecture 40 March 14th-MSKapi-26938624Noch keine Bewertungen
- Extra DDX NotesDokument1 SeiteExtra DDX Notesapi-26938624Noch keine Bewertungen
- DDX - Gastrointestinal Disorders ChartDokument21 SeitenDDX - Gastrointestinal Disorders Chartapi-26938624100% (2)
- Lecture 36 February 28th-Male Genetalia and ReproductionDokument3 SeitenLecture 36 February 28th-Male Genetalia and Reproductionapi-26938624Noch keine Bewertungen
- Lecture 37 March 2nd-RenalDokument2 SeitenLecture 37 March 2nd-Renalapi-26938624Noch keine Bewertungen
- Lecture 35 February 16th-Male Genetalia and ReproductionDokument3 SeitenLecture 35 February 16th-Male Genetalia and Reproductionapi-26938624Noch keine Bewertungen
- Lecture 33 February 7th-Breast and AxillaDokument4 SeitenLecture 33 February 7th-Breast and Axillaapi-26938624Noch keine Bewertungen
- The Following Presentation Contains Slides Not Suitable For Very Young Audiences. Parental Guidance Is Recommended.Dokument102 SeitenThe Following Presentation Contains Slides Not Suitable For Very Young Audiences. Parental Guidance Is Recommended.Princess Aira Bucag CarbonelNoch keine Bewertungen
- Intrapartal Nursing Care 1 in The Delivery Room MrsDokument184 SeitenIntrapartal Nursing Care 1 in The Delivery Room MrsRandy100% (2)
- Annotated BibliographyDokument23 SeitenAnnotated BibliographycatherinewangcNoch keine Bewertungen
- EVS Unit-5 PPopulation and The EnvironmentDokument13 SeitenEVS Unit-5 PPopulation and The EnvironmentSirajAyesha0% (1)
- 3 2 24 791 PDFDokument4 Seiten3 2 24 791 PDFKeerti PathakNoch keine Bewertungen
- Obstetrics and Gynaecology History Taking TemplateDokument4 SeitenObstetrics and Gynaecology History Taking TemplateLewis Song89% (9)
- Safe MotherhoodDokument16 SeitenSafe MotherhoodOswald DachagaNoch keine Bewertungen
- Huerto, Kathrina B. - OvuviewDokument2 SeitenHuerto, Kathrina B. - OvuviewKathrina Huerto100% (1)
- Respecting The Gift of Sexuality: Unit 10Dokument32 SeitenRespecting The Gift of Sexuality: Unit 10api-357572157100% (1)
- EndometriosisDokument153 SeitenEndometriosisoannny8661Noch keine Bewertungen
- GNRH Antagonists vs. GNRH Agonists 2008Dokument33 SeitenGNRH Antagonists vs. GNRH Agonists 2008Ahmad Badr El-DinNoch keine Bewertungen
- Ethinylestradiol Ph. Eur. 0.03mg + Desogestrel B.P 0.15mg (Microdiol)Dokument19 SeitenEthinylestradiol Ph. Eur. 0.03mg + Desogestrel B.P 0.15mg (Microdiol)asdwasdNoch keine Bewertungen
- Obs-Gynae HX and Examination-Bibek GhimireDokument68 SeitenObs-Gynae HX and Examination-Bibek GhimireKrishna PokhrelNoch keine Bewertungen
- Pathophysiology Breast CancerDokument3 SeitenPathophysiology Breast CancerNathalie kate petallarNoch keine Bewertungen
- Academic Writing UCC102 GROUP 6 Assignment RVDokument7 SeitenAcademic Writing UCC102 GROUP 6 Assignment RVBOL AKETCHNoch keine Bewertungen
- Kenya Teen Pregnancy Fact SheetDokument2 SeitenKenya Teen Pregnancy Fact SheetNational Catholic ReporterNoch keine Bewertungen
- InfertilityDokument29 SeitenInfertilityCristina StanleeNoch keine Bewertungen
- Roger Dodger (Script)Dokument50 SeitenRoger Dodger (Script)Animesh SharmaNoch keine Bewertungen
- Ulipristal Acetate: Review of Its Use in Emergency ContraseptionDokument12 SeitenUlipristal Acetate: Review of Its Use in Emergency ContraseptionAnonymous SDUIPeqXNoch keine Bewertungen
- TOG 2021 Volume 23 Issue 1Dokument81 SeitenTOG 2021 Volume 23 Issue 1Mahmoud AbubakrNoch keine Bewertungen
- Guidelines For Management of Endometrial CarcinomaDokument41 SeitenGuidelines For Management of Endometrial CarcinomaVeenaNoch keine Bewertungen
- Placental HormonesDokument16 SeitenPlacental HormonesSajid Aziz SamoNoch keine Bewertungen
- Anatomy & Physiology - AllDokument15 SeitenAnatomy & Physiology - AllAnubhav ShuklaNoch keine Bewertungen
- FC OB July 2021Dokument13 SeitenFC OB July 2021Johnmer Avelino100% (1)
- Gangguan Haid - PPT YudisDokument34 SeitenGangguan Haid - PPT YudisIde Yudis TiyoNoch keine Bewertungen
- Secondary Amenorrhea: DR Hanaa AlaniDokument44 SeitenSecondary Amenorrhea: DR Hanaa AlaniAakashNoch keine Bewertungen
- Bioethics - Care at The Beginning of LifeDokument3 SeitenBioethics - Care at The Beginning of LifeRobert Francis DikioNoch keine Bewertungen
- Abortion Guidelines and Protocol EnglishDokument44 SeitenAbortion Guidelines and Protocol EnglishAsghar KhanNoch keine Bewertungen
- Sex Education: Politicians, Parents, Teachers and Teens: Special AnalysisDokument4 SeitenSex Education: Politicians, Parents, Teachers and Teens: Special AnalysisrosieNoch keine Bewertungen
- 9autacoids 14010v9023022 Phpapp02Dokument109 Seiten9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)