Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Chatter: Rotary Club of Coburg IncDokument8 SeitenThe Chatter: Rotary Club of Coburg IncRotary CoburgNoch keine Bewertungen
- Antimicrobial Activity of CinnamonDokument5 SeitenAntimicrobial Activity of Cinnamonzeglam100% (1)
- I. Overview of The H5N1Dokument11 SeitenI. Overview of The H5N1Tâm NguyễnNoch keine Bewertungen
- UV Data SheetDokument15 SeitenUV Data SheetBrian ThompsonNoch keine Bewertungen
- ISO - ISO - TC 34 - SC 9 - MicrobiologyDokument11 SeitenISO - ISO - TC 34 - SC 9 - Microbiologyradwa tagNoch keine Bewertungen
- Swine Flu - Read About Symptoms, Treatment and H1N1 VaccineDokument10 SeitenSwine Flu - Read About Symptoms, Treatment and H1N1 VaccineRoyal ENoch keine Bewertungen
- (Texts in Applied Mathematics 61) Maia Martcheva - An Introduction To Mathematical Epidemiology-Springer US (2015)Dokument462 Seiten(Texts in Applied Mathematics 61) Maia Martcheva - An Introduction To Mathematical Epidemiology-Springer US (2015)ALBANO JOAQUIM100% (1)
- Occurrence, Characterization, and Antibiogram of Staphylococcus AureusDokument7 SeitenOccurrence, Characterization, and Antibiogram of Staphylococcus Aureusfarkad rawiNoch keine Bewertungen
- Gram Positive Cocci Reviewer 1Dokument6 SeitenGram Positive Cocci Reviewer 1alianaNoch keine Bewertungen
- Detailed Resume - 8.2.19Dokument12 SeitenDetailed Resume - 8.2.19naren_22Noch keine Bewertungen
- Mtap - Bacteriology FinalsDokument6 SeitenMtap - Bacteriology FinalsMoira Pauline LibroraniaNoch keine Bewertungen
- (IMCI) Integrated Management of Childhood IllnessDokument34 Seiten(IMCI) Integrated Management of Childhood Illnessɹǝʍdןnos97% (34)
- Measles Care Study-1Dokument28 SeitenMeasles Care Study-1YourFav RNNoch keine Bewertungen
- Idexx Introduces CDV Quant RealpcrDokument2 SeitenIdexx Introduces CDV Quant RealpcrPankaj BeniwalNoch keine Bewertungen
- Vibrio CholeraeDokument12 SeitenVibrio Choleraedorothy kageniNoch keine Bewertungen
- 7 Types of CurrDokument7 Seiten7 Types of CurrSue Anne Margaret BolivarNoch keine Bewertungen
- Report Text ExerciseDokument4 SeitenReport Text ExerciseJacky TanNoch keine Bewertungen
- Kapect CompoundDokument1 SeiteKapect Compoundmahgad100% (1)
- Epidemiology and Transmission of MeaslesDokument3 SeitenEpidemiology and Transmission of MeaslesharumiyaNoch keine Bewertungen
- Functional Anatomy of The Prokaryotic CellDokument22 SeitenFunctional Anatomy of The Prokaryotic Cellm umair zahirNoch keine Bewertungen
- WHO SurveillanceVaccinePreventable 21 Typhoid R1Dokument13 SeitenWHO SurveillanceVaccinePreventable 21 Typhoid R1Adre Dwi WiratamaNoch keine Bewertungen
- MODULE 6 To 9 LabDokument8 SeitenMODULE 6 To 9 Labkuyainday123Noch keine Bewertungen
- Pneumonia in Children: by DR L N Gachare Paediatrician/PulmonologistDokument35 SeitenPneumonia in Children: by DR L N Gachare Paediatrician/PulmonologistAlvin OmondiNoch keine Bewertungen
- Report CXX220621001 1655831565220Dokument2 SeitenReport CXX220621001 1655831565220CKNoch keine Bewertungen
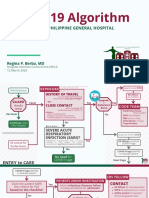
- COVID-19 Algorithm: For The Philippine General HospitalDokument10 SeitenCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNoch keine Bewertungen
- Hepatitis B Profile InterpretationDokument43 SeitenHepatitis B Profile InterpretationSAMMYNoch keine Bewertungen
- Gambaran Penggunaan Antibiotik Tanpa Resep Di Apotek X Kabupaten SragenDokument8 SeitenGambaran Penggunaan Antibiotik Tanpa Resep Di Apotek X Kabupaten Srageneka handayaniNoch keine Bewertungen
- SGD Case Presentation 10Dokument26 SeitenSGD Case Presentation 10Karen C. Del RosarioNoch keine Bewertungen
- Differentiate Prokaryotic and Eukaryotic CellsDokument47 SeitenDifferentiate Prokaryotic and Eukaryotic CellsMj BrionesNoch keine Bewertungen
- Intravascular Catheter-Related Bloodstreaminfections: Mark E. Rupp,, Rajendra KarnatakDokument23 SeitenIntravascular Catheter-Related Bloodstreaminfections: Mark E. Rupp,, Rajendra KarnatakCamilo GomezNoch keine Bewertungen