Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- TV Studio ChainDokument38 SeitenTV Studio ChainKalpesh Katara100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grade 5 DLL ENGLISH 5 Q3 Week 2Dokument7 SeitenGrade 5 DLL ENGLISH 5 Q3 Week 2Armie Joimie ValdezNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- MKT305 (Module 6 Segmentation)Dokument53 SeitenMKT305 (Module 6 Segmentation)Ngọc AnhhNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Italian Companies Eastern China - JAN 2014Dokument139 SeitenItalian Companies Eastern China - JAN 2014AndresNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- MMDA v. Viron Transportation CoDokument3 SeitenMMDA v. Viron Transportation CoTtlrpqNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Nursing Process Guide: St. Anthony's College Nursing DepartmentDokument10 SeitenNursing Process Guide: St. Anthony's College Nursing DepartmentAngie MandeoyaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Wolfgang Tillmans - NoticeDokument74 SeitenWolfgang Tillmans - NoticeSusana Vilas-BoasNoch keine Bewertungen
- Allergens 08242023Dokument5 SeitenAllergens 08242023Maalvika SinghNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Math9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Dokument37 SeitenMath9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Precious Arni100% (7)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Fashion Designer Research Paper ThesisDokument4 SeitenFashion Designer Research Paper Thesisafbteyrma100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Case Analysis OF Rajinder Singh V. State of PunjabDokument12 SeitenCase Analysis OF Rajinder Singh V. State of PunjabP TejeswariNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Way of St. LouiseDokument18 SeitenWay of St. LouiseMaryann GuevaradcNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Ind Nifty ItDokument2 SeitenInd Nifty ItRaghavendraNoch keine Bewertungen
- d301244x012 PDFDokument330 Seitend301244x012 PDFFIRMANSYAH100% (1)
- Tyvak PlatformsDokument1 SeiteTyvak PlatformsNguyenNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
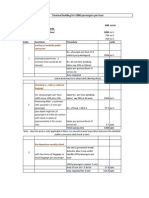
- Bus Terminal Building AreasDokument3 SeitenBus Terminal Building AreasRohit Kashyap100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nclex PogiDokument8 SeitenNclex Pogijackyd5Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Rock Classification Gizmo WorksheetDokument4 SeitenRock Classification Gizmo WorksheetDiamond실비Noch keine Bewertungen
- Test A 10 - 12520231610Dokument2 SeitenTest A 10 - 12520231610Quang HuyNoch keine Bewertungen
- SMEC01 CBRS Guide For NBC Reports - v1.1Dokument53 SeitenSMEC01 CBRS Guide For NBC Reports - v1.1phal sovannarithNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Infor LN Baan - Debugging The BshellDokument26 SeitenInfor LN Baan - Debugging The BshellShiva KumarNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- SHARE SEA Outlook Book 2518 r120719 2Dokument218 SeitenSHARE SEA Outlook Book 2518 r120719 2Raafi SeiffNoch keine Bewertungen
- COT Cott Aug 2017Dokument30 SeitenCOT Cott Aug 2017Ala BasterNoch keine Bewertungen
- Everyday Use AnalysisDokument8 SeitenEveryday Use AnalysisThe 3d PlanetNoch keine Bewertungen
- Staedtler FIMO Catalogue 2019 (STAEDTLER Hobby Creative Catalogue 2019 En)Dokument100 SeitenStaedtler FIMO Catalogue 2019 (STAEDTLER Hobby Creative Catalogue 2019 En)Tom S50% (2)
- Process of Trial of Criminal Cases in India (Flow Chart)Dokument1 SeiteProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- George Herbert Scherff Walker Bush: Agentur of The New World OrderDokument36 SeitenGeorge Herbert Scherff Walker Bush: Agentur of The New World Orderextemporaneous100% (3)
- Marxist Critique On LiberalsDokument17 SeitenMarxist Critique On LiberalsEmman TagubaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- TLE10 - Q3 - Lesson 5Dokument17 SeitenTLE10 - Q3 - Lesson 5Ella Cagadas PuzonNoch keine Bewertungen
- StratificationDokument91 SeitenStratificationAshish NairNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)