Das könnte Ihnen auch gefallen
- Phlebotomy Venipuncture ProcedureDokument12 SeitenPhlebotomy Venipuncture ProcedureYoussef MokdadNoch keine Bewertungen
- Skills Checklist Medication Checklist RN Program Rev 1.2014Dokument46 SeitenSkills Checklist Medication Checklist RN Program Rev 1.2014Youssef MokdadNoch keine Bewertungen
- CPG 3-1 Sedation and Analgesia For Diagnostic or Therapeutic ProceduresDokument11 SeitenCPG 3-1 Sedation and Analgesia For Diagnostic or Therapeutic ProceduresYoussef MokdadNoch keine Bewertungen
- NLN Pharmacology Study Guide Final 6-3-2013Dokument65 SeitenNLN Pharmacology Study Guide Final 6-3-2013الأغا محمد زكارنة100% (2)
- NLN Pharmacology Study Guide Final 6-3-2013Dokument65 SeitenNLN Pharmacology Study Guide Final 6-3-2013الأغا محمد زكارنة100% (2)
- Bio StatisticsDokument2 SeitenBio StatisticsYoussef MokdadNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Cardiac Cycle (Page Print 1-2)Dokument2 SeitenCardiac Cycle (Page Print 1-2)hihariv794Noch keine Bewertungen
- Practice StripsDokument9 SeitenPractice StripsErica Yamamoto50% (4)
- Ecg 2Dokument106 SeitenEcg 2hammad992Noch keine Bewertungen
- ECG Exercise, Insights, Ang HighlightsDokument5 SeitenECG Exercise, Insights, Ang HighlightsKerima Danica Lising GayoNoch keine Bewertungen
- 9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Dokument48 Seiten9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Rodrigo GutierrezNoch keine Bewertungen
- DRIPSDokument7 SeitenDRIPSKim Alvarez100% (2)
- SVT and DengueDokument4 SeitenSVT and Denguefrengki prasNoch keine Bewertungen
- 5.soap Chest PainDokument19 Seiten5.soap Chest PainDesiana Kemala SariNoch keine Bewertungen
- Cardiac Five YearsDokument31 SeitenCardiac Five Yearsdileepkumar.duhs4817Noch keine Bewertungen
- Overview of Hypertension in Adults - UpToDate PDFDokument62 SeitenOverview of Hypertension in Adults - UpToDate PDFIzamar RomeroNoch keine Bewertungen
- UsmleDokument3 SeitenUsmleuwandfaNoch keine Bewertungen
- Sunday Academic Meet - 240204 - 081157Dokument7 SeitenSunday Academic Meet - 240204 - 081157Srinivas PingaliNoch keine Bewertungen
- Effect of BP On Exer PracDokument36 SeitenEffect of BP On Exer PracPavan KumarNoch keine Bewertungen
- (PHA) 3.06 Antiarrhythmic Drugs - Dr.Dokument18 Seiten(PHA) 3.06 Antiarrhythmic Drugs - Dr.Mickaela Jaden KimNoch keine Bewertungen
- Test Bank For Human Biology Concepts and Current Issues 7th Edition JohnsonDokument26 SeitenTest Bank For Human Biology Concepts and Current Issues 7th Edition JohnsonJamesJacksonjbpof100% (74)
- (HeartSim 200 DfU) - 982Dokument86 Seiten(HeartSim 200 DfU) - 982edgargadoNoch keine Bewertungen
- Physiology CVS MCQ (Dr. Nassar)Dokument23 SeitenPhysiology CVS MCQ (Dr. Nassar)زياد سعيدNoch keine Bewertungen
- K - 12 Heart As A Pump (Fisiologi)Dokument36 SeitenK - 12 Heart As A Pump (Fisiologi)missirenaNoch keine Bewertungen
- ACLS Appendix 3Dokument32 SeitenACLS Appendix 3tostc100% (1)
- Med II-LE1-1.03 Arrhythmia NotesDokument14 SeitenMed II-LE1-1.03 Arrhythmia NotesAbigael SantosNoch keine Bewertungen
- Ekg PJKDokument110 SeitenEkg PJKDexel Putra SimbolonNoch keine Bewertungen
- Cardioversion and DefibrillationDokument18 SeitenCardioversion and DefibrillationJannah Marie A. Dimaporo100% (4)
- Physical Assessment of Patient With Cardiovascular DisorderDokument3 SeitenPhysical Assessment of Patient With Cardiovascular Disordermichelle marquezNoch keine Bewertungen
- Lecture Notes On CardiologyDokument31 SeitenLecture Notes On CardiologyambiskuysNoch keine Bewertungen
- Fuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary ADokument33 SeitenFuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary AAlfita RahmawatiNoch keine Bewertungen
- ACLS (Notes) (Printable)Dokument2 SeitenACLS (Notes) (Printable)mike_germain1172Noch keine Bewertungen
- (Manuju: Malahayati Nursing Journal, P-Issn: 2655-2728 E-ISSN: 2655-4712 VOLUME 3 NOMOR 3 TAHUN 2021) HAL 340-352Dokument13 Seiten(Manuju: Malahayati Nursing Journal, P-Issn: 2655-2728 E-ISSN: 2655-4712 VOLUME 3 NOMOR 3 TAHUN 2021) HAL 340-352Yurisma KhoerulNoch keine Bewertungen
- Poli Kesja (Laporan CDC Oktober)Dokument54 SeitenPoli Kesja (Laporan CDC Oktober)Welly ElvandariNoch keine Bewertungen
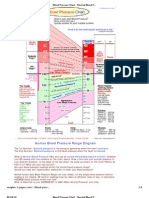
- Blood Pressure ChartDokument4 SeitenBlood Pressure ChartPixelateNoch keine Bewertungen
- Atlas of Cardiovascular EmergenciesDokument296 SeitenAtlas of Cardiovascular EmergenciesDana Bursacovschi100% (4)