Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Operating Room Nursing: S Y 2018-2019 FIRST SEMDokument29 SeitenOperating Room Nursing: S Y 2018-2019 FIRST SEMMaria Sheila BelzaNoch keine Bewertungen
- Đề Thi Học Kì 2 Tiếng Anh Lớp 8Dokument16 SeitenĐề Thi Học Kì 2 Tiếng Anh Lớp 8Uyên VũNoch keine Bewertungen
- English Civil WarDokument48 SeitenEnglish Civil WarsmrithiNoch keine Bewertungen
- MulanDokument1 SeiteMulanEnricNoch keine Bewertungen
- JQC Complaint No. No 12385 Judge Claudia Rickert IsomDokument165 SeitenJQC Complaint No. No 12385 Judge Claudia Rickert IsomNeil GillespieNoch keine Bewertungen
- Vol Vii TocDokument3 SeitenVol Vii Tocscribdman1Noch keine Bewertungen
- Khristine Rea Regino v. Pangasinan Colleges of Science and Technology, Et Al, G.R. No. 156109, November 18, 2004Dokument16 SeitenKhristine Rea Regino v. Pangasinan Colleges of Science and Technology, Et Al, G.R. No. 156109, November 18, 2004sunsetsailor85Noch keine Bewertungen
- The Supremacy of The ConstitutionDokument24 SeitenThe Supremacy of The ConstitutionJade FongNoch keine Bewertungen
- DL 57 PDFDokument2 SeitenDL 57 PDFmaheshm_erpNoch keine Bewertungen
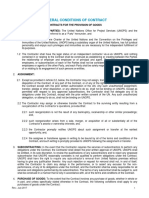
- UNOPS General Conditions Goods ENDokument12 SeitenUNOPS General Conditions Goods ENMohammedNoch keine Bewertungen
- Formulario Ds 160Dokument14 SeitenFormulario Ds 160Starling Javier AbogadoNoch keine Bewertungen
- Plaint Dissolution of MarriageDokument3 SeitenPlaint Dissolution of MarriageAmina AamerNoch keine Bewertungen
- Hubbard Co Jail PlanningDokument8 SeitenHubbard Co Jail PlanningShannon GeisenNoch keine Bewertungen
- CrimDokument1 SeiteCrimEdwin VillaNoch keine Bewertungen
- Science Writing Exercise 09-2014Dokument2 SeitenScience Writing Exercise 09-2014Chris Cesar Berdin Lagrio25% (4)
- Prime Marine Service vs. NLRC DDokument3 SeitenPrime Marine Service vs. NLRC DCzar Ian AgbayaniNoch keine Bewertungen
- Lincoln Movie Review & Film Summary (2012) - : Daniel Day-LewisDokument3 SeitenLincoln Movie Review & Film Summary (2012) - : Daniel Day-LewisGonzaloqplorenz XpNoch keine Bewertungen
- Simone de BeauvoirDokument6 SeitenSimone de BeauvoirŞtefan PopovNoch keine Bewertungen
- G.R. No. 159889 June 5, 2008Dokument4 SeitenG.R. No. 159889 June 5, 2008Tovy BordadoNoch keine Bewertungen
- Rudi Schwab: The Forgotten Letters by Daniel SchwabDokument138 SeitenRudi Schwab: The Forgotten Letters by Daniel SchwabDaniel SchwabNoch keine Bewertungen
- 47 - Ong Vs CA, GR 95386, May 29, 1997Dokument6 Seiten47 - Ong Vs CA, GR 95386, May 29, 1997美咲剛Noch keine Bewertungen
- Prisoner of Zenda - Elements of The NovelDokument16 SeitenPrisoner of Zenda - Elements of The NovelNor Azizah Bachok100% (5)
- Class XII English CORE Chapter 5 - Indigo by Louis FischerDokument15 SeitenClass XII English CORE Chapter 5 - Indigo by Louis FischerShivam YadavNoch keine Bewertungen
- Contract Ii Case Review (Doc Frustration) PDFDokument25 SeitenContract Ii Case Review (Doc Frustration) PDFkhairiah tsamNoch keine Bewertungen
- Defaulter Web List BBBDokument20 SeitenDefaulter Web List BBBBB ENTERPRISESNoch keine Bewertungen
- Clean Hands, Pure HeartDokument325 SeitenClean Hands, Pure HeartnathanethridgeNoch keine Bewertungen
- Black Lives Matter Protests Movie TranscriptDokument9 SeitenBlack Lives Matter Protests Movie TranscriptActionNewsJaxNoch keine Bewertungen
- JN KDokument24 SeitenJN Kcatch.amit19Noch keine Bewertungen
- ASIL Public International Law Bar Reviewer 2019 PDFDokument73 SeitenASIL Public International Law Bar Reviewer 2019 PDFVM50% (2)
- Lets Talk Dating LeaderDokument5 SeitenLets Talk Dating LeaderLy Ri CaNoch keine Bewertungen