Das könnte Ihnen auch gefallen
- Introduction to Clinical Reproductive EndocrinologyVon EverandIntroduction to Clinical Reproductive EndocrinologyBewertung: 1 von 5 Sternen1/5 (1)
- Paraphimosis in The DogDokument4 SeitenParaphimosis in The DogErick GarciaNoch keine Bewertungen
- Effects of Dietary Flax Seed and Sunflower Seed Supplementation On Normal Canine Serum Polyunsaturated Fatty Acids and Skin and Hair PDFDokument7 SeitenEffects of Dietary Flax Seed and Sunflower Seed Supplementation On Normal Canine Serum Polyunsaturated Fatty Acids and Skin and Hair PDFjenNoch keine Bewertungen
- Anestesia em Animais Silvestres Capitulo 1Dokument24 SeitenAnestesia em Animais Silvestres Capitulo 1Daniel CostaNoch keine Bewertungen
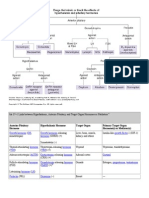
- Anterior Pituitary Hormone Hypothalamic Hormone Target Organ Primary Target Organ Hormone(s) or Mediator(s)Dokument10 SeitenAnterior Pituitary Hormone Hypothalamic Hormone Target Organ Primary Target Organ Hormone(s) or Mediator(s)kep1313Noch keine Bewertungen
- Somatostain: Growth Hormone - Inhibiting Hormone (GHIH)Dokument9 SeitenSomatostain: Growth Hormone - Inhibiting Hormone (GHIH)Daniel AtiehNoch keine Bewertungen
- 2 HZ Hypothalamic and Pituitary Hormones HZDokument20 Seiten2 HZ Hypothalamic and Pituitary Hormones HZAmirabbas SaffariNoch keine Bewertungen
- EndocrinologyDokument7 SeitenEndocrinologyVijith.V.kumarNoch keine Bewertungen
- Endocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIDokument77 SeitenEndocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIdrdhirenvet100% (9)
- Tesamorelin Is Used To Stimulate GH and Its Lipolytic Effects, Helping To Decrease TheDokument19 SeitenTesamorelin Is Used To Stimulate GH and Its Lipolytic Effects, Helping To Decrease TheGeraldine PatayanNoch keine Bewertungen
- Jardine Jade Albert C. Valdez, RMTDokument48 SeitenJardine Jade Albert C. Valdez, RMTEj BersalonaNoch keine Bewertungen
- Gonadal Hormones and InhibitorsDokument101 SeitenGonadal Hormones and Inhibitors2012100% (4)
- FSH Final JLy 7 08Dokument6 SeitenFSH Final JLy 7 08TanveerNoch keine Bewertungen
- FSH Final JLy 7 08 PDFDokument6 SeitenFSH Final JLy 7 08 PDFTanveerNoch keine Bewertungen
- Hormone of Reproductive System (Synthesis and Mechanism of Action)Dokument38 SeitenHormone of Reproductive System (Synthesis and Mechanism of Action)pwfNoch keine Bewertungen
- 1 Hormone Intro.Dokument6 Seiten1 Hormone Intro.Nashat SaadiNoch keine Bewertungen
- Gonadotropins: Luteinizing and Follicle Stimulating HormonesDokument4 SeitenGonadotropins: Luteinizing and Follicle Stimulating HormoneschintyaNoch keine Bewertungen
- 1 Pituitary Hormonesthis.8732849.PowerpointDokument24 Seiten1 Pituitary Hormonesthis.8732849.Powerpointmustafa aliNoch keine Bewertungen
- ENDODokument141 SeitenENDOearldem1996Noch keine Bewertungen
- GNRH Antagonist in InfertilityDokument70 SeitenGNRH Antagonist in InfertilityBrijesh MishraNoch keine Bewertungen
- The Normal Menstrual CycleDokument12 SeitenThe Normal Menstrual CycleDheyaa A. SabahNoch keine Bewertungen
- Drug Acting On The Endocrine SystemDokument156 SeitenDrug Acting On The Endocrine SystemGenki Fay B. LequiganNoch keine Bewertungen
- GonadotropinsDokument3 SeitenGonadotropinsUMINAHNoch keine Bewertungen
- Anterior and Posterio Pituitary GlandDokument7 SeitenAnterior and Posterio Pituitary GlandAnny AlvrzNoch keine Bewertungen
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDokument27 SeitenThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanNoch keine Bewertungen
- What Is A Hormone?Dokument8 SeitenWhat Is A Hormone?IJSmartNoch keine Bewertungen
- GNRH and GonadotropinsDokument47 SeitenGNRH and Gonadotropinskaleab AlemayehuNoch keine Bewertungen
- Ovarian and Menstrual CyclesDokument19 SeitenOvarian and Menstrual CyclesDrDiya AlkayidNoch keine Bewertungen
- Gonadal HormonesDokument40 SeitenGonadal HormonesJoyce VillanuevaNoch keine Bewertungen
- Pharmacology: Drugs Acting On The Reproductive SystemDokument8 SeitenPharmacology: Drugs Acting On The Reproductive SystemShun Reigh SumilangNoch keine Bewertungen
- Hormonal Agents PharmacologyDokument64 SeitenHormonal Agents Pharmacologynica velanoNoch keine Bewertungen
- Action of PillDokument9 SeitenAction of Pillnajdah fakhirahNoch keine Bewertungen
- Toksikologi Makalah Tentang Efek Kimia Pada Sistem ReproduksiDokument13 SeitenToksikologi Makalah Tentang Efek Kimia Pada Sistem ReproduksiRifdah Fidrilani RahayuNoch keine Bewertungen
- Physiology, Luteinizing Hormone - StatPearls - NCBI BookshelfDokument5 SeitenPhysiology, Luteinizing Hormone - StatPearls - NCBI Bookshelfpopa.irinaNoch keine Bewertungen
- DisxussionDokument2 SeitenDisxussionGERA KAYE BUNCALANNoch keine Bewertungen
- Endocrinology Notes: Veterinary PhysiologyDokument16 SeitenEndocrinology Notes: Veterinary PhysiologyBrian AllanNoch keine Bewertungen
- Oxytocin, ADH Lecture For 2nd Year MBBS by DR Waeem KausarDokument28 SeitenOxytocin, ADH Lecture For 2nd Year MBBS by DR Waeem KausarIMDCBiochemNoch keine Bewertungen
- Reproductive Endocrinology FinalDokument98 SeitenReproductive Endocrinology FinalChino Paolo SamsonNoch keine Bewertungen
- Endocrinology Pharmacology: Hormone Agonists, Antagonists & ModulatorsDokument151 SeitenEndocrinology Pharmacology: Hormone Agonists, Antagonists & Modulatorsj.doe.hex_87100% (1)
- GNRH Agonists Et AnatagonistsDokument44 SeitenGNRH Agonists Et Anatagonistshoussein.hajj.md100% (1)
- Gonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsDokument29 SeitenGonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsGopal Prasad DahalNoch keine Bewertungen
- The Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogDokument41 SeitenThe Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogEvi Liana BahriahNoch keine Bewertungen
- Anterior Pituitary HormonesDokument46 SeitenAnterior Pituitary Hormonespramod bhaleraoNoch keine Bewertungen
- Notes For Lecture 9Dokument11 SeitenNotes For Lecture 9BelNoch keine Bewertungen
- Steroid Hormones in Food Producing Animals: Regulatory Situation in EuropeDokument19 SeitenSteroid Hormones in Food Producing Animals: Regulatory Situation in Europekj185Noch keine Bewertungen
- Use of ExogenousDokument6 SeitenUse of ExogenousInfinit13Noch keine Bewertungen
- Reproductive MedicineDokument330 SeitenReproductive MedicineunknownxemNoch keine Bewertungen
- George Trachte ENDO/REPRO: RD NDDokument3 SeitenGeorge Trachte ENDO/REPRO: RD NDHailey RobertsNoch keine Bewertungen
- Hormon ReproDokument36 SeitenHormon Reproalvinrinaldi1101Noch keine Bewertungen
- MenopauseDokument21 SeitenMenopauseDr K AmbareeshaNoch keine Bewertungen
- Pituitary, Thyroid & Adrenal HormonesDokument13 SeitenPituitary, Thyroid & Adrenal HormonesJose Melmar Autida AutenticoNoch keine Bewertungen
- Luteinizing HormoneDokument8 SeitenLuteinizing HormoneSaba MalikNoch keine Bewertungen
- TECHNOLOGICAL INSTITUTE OF THE PHILIPPINES ASSIGNMENTDokument4 SeitenTECHNOLOGICAL INSTITUTE OF THE PHILIPPINES ASSIGNMENTMarvin ParasNoch keine Bewertungen
- Role of hormones on reproductionDokument5 SeitenRole of hormones on reproductionkushal NeupaneNoch keine Bewertungen
- Hypopituitarism Group F BSN 3Dokument21 SeitenHypopituitarism Group F BSN 3Mari IllustriousNoch keine Bewertungen
- TESTIS Endocrinology Overview RSS Yuen Et Al 2018Dokument7 SeitenTESTIS Endocrinology Overview RSS Yuen Et Al 2018LudimilaNoch keine Bewertungen
- REPRODUCTIVE HORMONES AND THEIR FUNCTIONSDokument6 SeitenREPRODUCTIVE HORMONES AND THEIR FUNCTIONSOwolabi PetersNoch keine Bewertungen
- Puberty and The HPG AxisDokument36 SeitenPuberty and The HPG AxiskjhkaNoch keine Bewertungen
- Growth Hormone Physiology in AdultsDokument26 SeitenGrowth Hormone Physiology in AdultsDini Jatiya AnggrainiNoch keine Bewertungen
- 2019 Gonadal Hormones-3Dokument197 Seiten2019 Gonadal Hormones-3Vishwajeet RaneNoch keine Bewertungen
- Julho - 22 Us CoachDokument7 SeitenJulho - 22 Us CoachPantajr - GTR250Noch keine Bewertungen
- Eurl Rhesus Lab: Listing Des Reactifs Et Consommables Snibe 2021Dokument5 SeitenEurl Rhesus Lab: Listing Des Reactifs Et Consommables Snibe 2021Fateh AzwiNoch keine Bewertungen
- Superovulasi PDFDokument68 SeitenSuperovulasi PDFHayatul IlmiNoch keine Bewertungen
- Estrogen, Progesterone, Testesterone, and Placental HormonesDokument57 SeitenEstrogen, Progesterone, Testesterone, and Placental HormonesBramwell K. MiteiNoch keine Bewertungen
- (Pha) Le 5Dokument19 Seiten(Pha) Le 5Gabby TanNoch keine Bewertungen
- Pituitary and ThyroidDokument54 SeitenPituitary and ThyroidSaif AliNoch keine Bewertungen
- Assessment of Pituitary Function and Hormone EvaluationDokument114 SeitenAssessment of Pituitary Function and Hormone Evaluationmalex33yNoch keine Bewertungen
- List of Human Hormones: Hormone ListingDokument7 SeitenList of Human Hormones: Hormone ListingMohammed AslumNoch keine Bewertungen
- 10 best steroid cycles for bodybuildingDokument6 Seiten10 best steroid cycles for bodybuildingKaizer DaveNoch keine Bewertungen
- Endocrine System IntroductionDokument5 SeitenEndocrine System IntroductionAnnapurna DangetiNoch keine Bewertungen
- Endocrine - HistoworldDokument12 SeitenEndocrine - HistoworldKarl Torres Uganiza RmtNoch keine Bewertungen
- The HPO AxisDokument4 SeitenThe HPO AxisBilal Irshan Eka RiselioNoch keine Bewertungen
- UT Progestin PDFDokument10 SeitenUT Progestin PDFLidyaNoch keine Bewertungen
- Predicted ovarian response and treatment protocolsDokument1 SeitePredicted ovarian response and treatment protocolsatawa1Noch keine Bewertungen
- Hormonal Advances OlufemiDokument90 SeitenHormonal Advances OlufemiDare Olalekan AnthonyNoch keine Bewertungen
- Glucocorticoids and Mineralocorticoids: Roles and EffectsDokument27 SeitenGlucocorticoids and Mineralocorticoids: Roles and EffectsAmrit GaireNoch keine Bewertungen
- The Ultimate PCT Supplement (Hpta Restoration) - Looksmax - Org - Men's Self-Improvement & AestheticsDokument25 SeitenThe Ultimate PCT Supplement (Hpta Restoration) - Looksmax - Org - Men's Self-Improvement & Aestheticskrakesh7848Noch keine Bewertungen
- Anatomy, Physiology of The Endocrine System: Geofrey S. SevillenoDokument55 SeitenAnatomy, Physiology of The Endocrine System: Geofrey S. Sevillenocoral jade cuaNoch keine Bewertungen
- Endo ReviewerDokument5 SeitenEndo ReviewerZIAN LABADIANoch keine Bewertungen
- Human Physiology An Integrated Approach 7Th Edition Silverthorn Solutions Manual Full Chapter PDFDokument36 SeitenHuman Physiology An Integrated Approach 7Th Edition Silverthorn Solutions Manual Full Chapter PDFcleopatrabanhft1vh7100% (10)
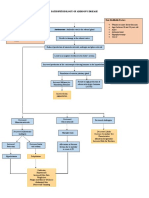
- Pathophysiology of Addison's Disease ExplainedDokument2 SeitenPathophysiology of Addison's Disease ExplainedHanna NocumNoch keine Bewertungen
- ENG Srdjan Pandurevic - Luteinising Hormone and Insulin Resistance-1Dokument14 SeitenENG Srdjan Pandurevic - Luteinising Hormone and Insulin Resistance-1Srđan PandurevićNoch keine Bewertungen
- Vetocept Uses, Dosage & Storage for Ovarian Cysts TreatmentDokument1 SeiteVetocept Uses, Dosage & Storage for Ovarian Cysts TreatmentImran KhanNoch keine Bewertungen
- NEET Chemical Control and Coordination Important QuestionsDokument14 SeitenNEET Chemical Control and Coordination Important QuestionsAditiNoch keine Bewertungen
- Tablas de Valores Hormonales NormalesDokument2 SeitenTablas de Valores Hormonales NormalesFrances HernandezNoch keine Bewertungen
- Biol 460 Case StudyDokument11 SeitenBiol 460 Case Studyapi-353888678Noch keine Bewertungen
- Which OCP Is Best Handout PDFDokument4 SeitenWhich OCP Is Best Handout PDFMarianna LeeNoch keine Bewertungen
- The Hypothalamus and Pituitary GlandDokument44 SeitenThe Hypothalamus and Pituitary GlandRujha Haniena Ahmad RidzuanNoch keine Bewertungen
- Chemical Coordination and IntegrationDokument7 SeitenChemical Coordination and IntegrationAnonymous -Noch keine Bewertungen
- MCQ REPRODUCTION: HORMONES, FOLLICULAR DEVELOPMENT, MENSTRUAL CYCLEDokument2 SeitenMCQ REPRODUCTION: HORMONES, FOLLICULAR DEVELOPMENT, MENSTRUAL CYCLEwanderer_1010100% (1)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossVon EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossBewertung: 4 von 5 Sternen4/5 (22)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanVon EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanBewertung: 3.5 von 5 Sternen3.5/5 (3)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthVon EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNoch keine Bewertungen
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthVon EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthBewertung: 5 von 5 Sternen5/5 (37)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 5 von 5 Sternen5/5 (1)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainVon EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainBewertung: 3.5 von 5 Sternen3.5/5 (6)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeVon EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeBewertung: 5 von 5 Sternen5/5 (1)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Keto Friendly Recipes: Easy Keto For Busy PeopleVon EverandKeto Friendly Recipes: Easy Keto For Busy PeopleBewertung: 2 von 5 Sternen2/5 (1)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingVon EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingBewertung: 5 von 5 Sternen5/5 (59)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItVon EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItBewertung: 4.5 von 5 Sternen4.5/5 (19)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouVon EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNoch keine Bewertungen
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodVon EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodBewertung: 4.5 von 5 Sternen4.5/5 (18)
- Ultrametabolism: The Simple Plan for Automatic Weight LossVon EverandUltrametabolism: The Simple Plan for Automatic Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (28)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodVon EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodBewertung: 2 von 5 Sternen2/5 (1)
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeVon EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeBewertung: 4 von 5 Sternen4/5 (3)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfVon EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfBewertung: 5 von 5 Sternen5/5 (2)
- Younger: A Breakthrough Program to Reset Your Genes, Reverse Aging & Turn Back the Clock 10 YearsVon EverandYounger: A Breakthrough Program to Reset Your Genes, Reverse Aging & Turn Back the Clock 10 YearsNoch keine Bewertungen
- The Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffVon EverandThe Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffNoch keine Bewertungen
- The Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITVon EverandThe Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITBewertung: 5 von 5 Sternen5/5 (1)
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesVon EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesNoch keine Bewertungen
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaVon EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNoch keine Bewertungen
- Kintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritVon EverandKintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritBewertung: 4.5 von 5 Sternen4.5/5 (3)
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossVon EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (22)