Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Nutech University Admission SlipDokument3 SeitenNutech University Admission SlipaliiiiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- 9th BASIC ENGLISH TEST - 10-08-19 PDFDokument3 Seiten9th BASIC ENGLISH TEST - 10-08-19 PDFJIM GUIMACNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Impact of Training On The Performance of Employeees in The Public Sector - A Case Study of MoWTDokument56 SeitenImpact of Training On The Performance of Employeees in The Public Sector - A Case Study of MoWTJJINGO ISAAC100% (2)
- 1st QE Grade 11 English 2019-20Dokument7 Seiten1st QE Grade 11 English 2019-20Mihatsu TakiNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Linux AdministrationDokument361 SeitenLinux AdministrationmohdkmnNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
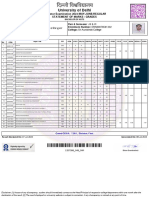
- University of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesDokument2 SeitenUniversity of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesFit CollegeNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Building Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanDokument3 SeitenBuilding Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanrtwthcdjwtNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Philosophical Thoughts in EducationDokument22 SeitenPhilosophical Thoughts in Educationapi-619738021Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- CYRILDokument10 SeitenCYRILEsang DiezNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Kiana Whickham Feedback BridgeDokument7 SeitenKiana Whickham Feedback Bridgeapi-332895647Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Institution Literature Study PDFDokument74 SeitenInstitution Literature Study PDFAditi GoelNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Learning and Talent Development 2012Dokument42 SeitenLearning and Talent Development 2012Phyo ThuNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Astronauts ScriptDokument3 SeitenAstronauts ScriptakkurayhanNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Professional Development Plan (Required)Dokument4 SeitenProfessional Development Plan (Required)api-314843306Noch keine Bewertungen
- Ecpe TestDokument20 SeitenEcpe Test09092004100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Type of Test - Hypotheses PDFDokument32 SeitenType of Test - Hypotheses PDFCarmina CrăciunNoch keine Bewertungen
- Mathematical Excursions 4th Edition Aufmann Test Bank 1Dokument12 SeitenMathematical Excursions 4th Edition Aufmann Test Bank 1malissa100% (50)
- Family Involvement - How Do I Help My Child Study - ChieSB - FDokument5 SeitenFamily Involvement - How Do I Help My Child Study - ChieSB - FChie SBNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- 22 Self-Actualization Tests & Tools To Apply Maslow's TheoryDokument34 Seiten22 Self-Actualization Tests & Tools To Apply Maslow's TheoryIbrahim HarfoushNoch keine Bewertungen
- Community Service Reflection PaperDokument2 SeitenCommunity Service Reflection Paperapi-525941594Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Henry A. Giroux Teachers As IntellectualsDokument341 SeitenHenry A. Giroux Teachers As Intellectualsedgar alirio insuastiNoch keine Bewertungen
- Building Parent-Teacher Relationships: American Federation of TeachersDokument5 SeitenBuilding Parent-Teacher Relationships: American Federation of Teachersapi-609545195Noch keine Bewertungen
- Opertti Et Al - Ibe Unesco 2021 Inclusion in EducDokument6 SeitenOpertti Et Al - Ibe Unesco 2021 Inclusion in EducSergio RiquelmeNoch keine Bewertungen
- Theme and Main Idea Lesson 2Dokument4 SeitenTheme and Main Idea Lesson 2api-581790895Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Person PerceptionDokument2 SeitenPerson Perceptionuzii09Noch keine Bewertungen
- 10 1190@geo2018-0452 1Dokument22 Seiten10 1190@geo2018-0452 1Emanuelle MachadoNoch keine Bewertungen
- Handbook Addendum: Student & ParentDokument42 SeitenHandbook Addendum: Student & ParentExam PurposeNoch keine Bewertungen
- Assessment Form 2 PDFDokument1 SeiteAssessment Form 2 PDFAgnes Bansil Vitug100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Academic TextDokument2 SeitenAcademic TextCatherine ProndosoNoch keine Bewertungen
- HR Questions InterviewDokument54 SeitenHR Questions InterviewAlice AliceNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)