Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hospital: List of Departments in Hospital and Its FunctionsDokument7 SeitenHospital: List of Departments in Hospital and Its FunctionsErine ParanNoch keine Bewertungen
- Customized NQAS Checklist For Non Beded PHC of OdishaDokument40 SeitenCustomized NQAS Checklist For Non Beded PHC of Odishaqa100% (1)
- NASKAH PUBLIKASI 1,5 (Bahasa Inggris)Dokument15 SeitenNASKAH PUBLIKASI 1,5 (Bahasa Inggris)yuyunNoch keine Bewertungen
- Of Hospital Management System: Requirement Specification DocumentDokument14 SeitenOf Hospital Management System: Requirement Specification DocumentHarshvardhan SoniNoch keine Bewertungen
- Test Bank For Medical Terminology A Living Language 6th Edition by FremgenDokument45 SeitenTest Bank For Medical Terminology A Living Language 6th Edition by Fremgena596727542100% (2)
- ACCP Standards of PracticeDokument4 SeitenACCP Standards of Practiceryuurecca0% (1)
- JAWSmith FinalDokument34 SeitenJAWSmith FinalRENIEL MARK BASENoch keine Bewertungen
- Test Bank For Understanding Health Insurance 13th Edition by GreenDokument14 SeitenTest Bank For Understanding Health Insurance 13th Edition by Greenpatriciajonesewrkbtsnfg100% (14)
- Decision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsDokument12 SeitenDecision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsPatricia Franco-VillaNoch keine Bewertungen
- Medical AuditDokument9 SeitenMedical AuditKailash NagarNoch keine Bewertungen
- Closed Medical Record ReviewDokument6 SeitenClosed Medical Record ReviewMuzna Iqbal50% (2)
- Patient Handbook & Telephone DirectoryDokument28 SeitenPatient Handbook & Telephone Directoryapi-219008748Noch keine Bewertungen
- Records Management 10th Edition Read Test BankDokument25 SeitenRecords Management 10th Edition Read Test BankJamesGonzalezwbpg100% (44)
- Acute Care PT Core CompetenciesDokument16 SeitenAcute Care PT Core CompetenciesYoga HanditaNoch keine Bewertungen
- Carol and Odis Peavy School of Nursing University of St. Thomas Accelerated Bachelor of Science in Nursing (ABSN) TrackDokument16 SeitenCarol and Odis Peavy School of Nursing University of St. Thomas Accelerated Bachelor of Science in Nursing (ABSN) TrackKamil MominNoch keine Bewertungen
- Open EMRDokument38 SeitenOpen EMRSuhail BhatiaNoch keine Bewertungen
- Incident ReportsDokument13 SeitenIncident Reportsrobertesguerra18Noch keine Bewertungen
- Quality IndicatorsDokument10 SeitenQuality IndicatorsKanna NikithaNoch keine Bewertungen
- This Study Resource Was: Chapter 9: Essay QuestionsDokument5 SeitenThis Study Resource Was: Chapter 9: Essay QuestionsSherlock HolmesNoch keine Bewertungen
- Booklet 14 Keeping of Patience RecordsDokument12 SeitenBooklet 14 Keeping of Patience RecordsNeo Mervyn MonahengNoch keine Bewertungen
- ICD-10 Guidelines For The Physician CoderDokument17 SeitenICD-10 Guidelines For The Physician Coderlina_villegas_13Noch keine Bewertungen
- Nclex New Lastest New LastDokument266 SeitenNclex New Lastest New LastNadim Khalid0% (2)
- 4 F Guevara Muñoz B3 U2Dokument15 Seiten4 F Guevara Muñoz B3 U2CHRISTIAN GUEVARANoch keine Bewertungen
- Cruise Ship Health Care Guidelines PrepDokument8 SeitenCruise Ship Health Care Guidelines PrepMaxMusterNoch keine Bewertungen
- Care 2000Dokument9 SeitenCare 2000Sneha_Sawant_4900100% (2)
- The 2.2m Contract Between King's College London's Institute of Psychiatry and The UK Ministry of Defence.Dokument27 SeitenThe 2.2m Contract Between King's College London's Institute of Psychiatry and The UK Ministry of Defence.DocumentsZA100% (2)
- HCC GuidebookDokument153 SeitenHCC Guidebookleadmonkeyboy100% (2)
- Guidelines On The Management of Medico Legal Complaints in Ministry of Health 2ND Edition 2019Dokument41 SeitenGuidelines On The Management of Medico Legal Complaints in Ministry of Health 2ND Edition 2019Nokoline HuNoch keine Bewertungen
- Ppe3 Table Reflection and Signed OffDokument4 SeitenPpe3 Table Reflection and Signed Offapi-318846856Noch keine Bewertungen
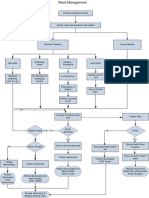
- Ward ManagementDokument1 SeiteWard Managementaman kumar jhaNoch keine Bewertungen