Das könnte Ihnen auch gefallen
- Cerebral Herniation Syndromes and Intracranial HypertensionVon EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNoch keine Bewertungen
- Acute Symptomatic Peri-Lead Edema 33 Hours After Deep Brain Stimulation Surgery: A Case ReportDokument4 SeitenAcute Symptomatic Peri-Lead Edema 33 Hours After Deep Brain Stimulation Surgery: A Case ReportsyarifaNoch keine Bewertungen
- Deep Brain Stimulation For Psychiatric Disorders-SDokument22 SeitenDeep Brain Stimulation For Psychiatric Disorders-SAldo VictoriaNoch keine Bewertungen
- Saj8 19920914Dokument13 SeitenSaj8 19920914Muhammad Faizan RafiqNoch keine Bewertungen
- Stereotactic Implantation of Deep BrainDokument28 SeitenStereotactic Implantation of Deep Brainberna chuaNoch keine Bewertungen
- Luig Jes 2013Dokument12 SeitenLuig Jes 2013ximena sanchezNoch keine Bewertungen
- Blueprint For Neurostimulation With Intranasal Light TherapyDokument28 SeitenBlueprint For Neurostimulation With Intranasal Light Therapy456456456y45y45100% (1)
- Lozano DBS CurrentStatus NatReviews2020Dokument13 SeitenLozano DBS CurrentStatus NatReviews2020bobNoch keine Bewertungen
- Oxford Textbook of Neurocritical CareDokument750 SeitenOxford Textbook of Neurocritical CareMykhailo LysianskyiNoch keine Bewertungen
- Estimulación Nervio VagoDokument12 SeitenEstimulación Nervio VagoMiguel A. RojasNoch keine Bewertungen
- Medsci 07 00047Dokument17 SeitenMedsci 07 00047Jorge MontenegroNoch keine Bewertungen
- MinervaAnestesiol-12294 ProofinPDF V3 2018-03-16Dokument10 SeitenMinervaAnestesiol-12294 ProofinPDF V3 2018-03-16Marcela Sanchez ParraNoch keine Bewertungen
- Sedation Vacation in Neurocritical Care: A Proposal AlgorithmDokument3 SeitenSedation Vacation in Neurocritical Care: A Proposal Algorithmrodolfo riosNoch keine Bewertungen
- Aplicaciones Clínicas de La DbsDokument10 SeitenAplicaciones Clínicas de La DbsTARNoch keine Bewertungen
- Document ABHISHEK CHOUBAYDokument12 SeitenDocument ABHISHEK CHOUBAYRishika AhujaNoch keine Bewertungen
- Deep Brain Stimulation Guide ParkinsonsDokument56 SeitenDeep Brain Stimulation Guide ParkinsonsGaurav MehtaNoch keine Bewertungen
- Milne (2022) - Neuromonitoring and Neurocognitive Outcomes in Cardiac SurgeryDokument16 SeitenMilne (2022) - Neuromonitoring and Neurocognitive Outcomes in Cardiac SurgeryVanessaNoch keine Bewertungen
- Dowd 2017 Basal GangliaDokument9 SeitenDowd 2017 Basal Gangliasingle_ladyNoch keine Bewertungen
- DBS2008Dokument48 SeitenDBS2008Carol Artigas Gómez100% (1)
- Mental Depression©: Andrew HagueDokument7 SeitenMental Depression©: Andrew Hagueajmrr editorNoch keine Bewertungen
- Acute Disseminated Encephalomyelitis in Young Female - A Diagnosis of ExclusionDokument3 SeitenAcute Disseminated Encephalomyelitis in Young Female - A Diagnosis of ExclusionIJAR JOURNALNoch keine Bewertungen
- ECT Guide: Treatments, History, and ProcedureDokument13 SeitenECT Guide: Treatments, History, and ProcedureMahmoud HassanNoch keine Bewertungen
- Delirium After Deep Brain Stimulation in Parkinson's DiseaseDokument10 SeitenDelirium After Deep Brain Stimulation in Parkinson's DiseaseMikeVDCNoch keine Bewertungen
- Review DBSDokument8 SeitenReview DBSEtonia PangNoch keine Bewertungen
- RTMS For The Treatment of Depression A ComprehensiDokument14 SeitenRTMS For The Treatment of Depression A ComprehensiSahuri SahuriNoch keine Bewertungen
- Epidural Hematoma Treatment & ManagementDokument5 SeitenEpidural Hematoma Treatment & ManagementazharyekaputraNoch keine Bewertungen
- Chapter 28 Electroconvulsive Therapy (ECT)Dokument13 SeitenChapter 28 Electroconvulsive Therapy (ECT)VikneswariNoch keine Bewertungen
- Kelompok 2Dokument23 SeitenKelompok 2lutfiah nabilahNoch keine Bewertungen
- JCM 10 05912Dokument8 SeitenJCM 10 05912Sandara SamperNoch keine Bewertungen
- Neuroprotección en TEC, Revisión ActualizadaDokument11 SeitenNeuroprotección en TEC, Revisión ActualizadaGustavo Delgado ReyesNoch keine Bewertungen
- Articulo Este SiZXCDokument7 SeitenArticulo Este SiZXCFabricio NuñezNoch keine Bewertungen
- Spinal Cord Injury: A Systematic Review of Current Treatment OptionsDokument10 SeitenSpinal Cord Injury: A Systematic Review of Current Treatment OptionsEtika Tunjung KencanaNoch keine Bewertungen
- Deep Brain StimulationDokument4 SeitenDeep Brain StimulationCristian GondacNoch keine Bewertungen
- 2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestDokument169 Seiten2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestKishore Reddy BhavanamNoch keine Bewertungen
- Experimental Therapy May Treat DepressionDokument4 SeitenExperimental Therapy May Treat DepressionjohntandraNoch keine Bewertungen
- Introduction to Traumatic Brain InjuryDokument25 SeitenIntroduction to Traumatic Brain InjuryRyo JamunNoch keine Bewertungen
- Spinal Injury CordDokument10 SeitenSpinal Injury Cordeleanai limaNoch keine Bewertungen
- Efficacy of Sphenopalatine Ganglion Radiofrequency in Refractory Chronic Cluster HeadacheDokument8 SeitenEfficacy of Sphenopalatine Ganglion Radiofrequency in Refractory Chronic Cluster HeadacheareteusNoch keine Bewertungen
- Thy HipotermiaDokument42 SeitenThy HipotermiaDedi SutiaNoch keine Bewertungen
- Ijms 13 11753 PDFDokument20 SeitenIjms 13 11753 PDFVandy IkraNoch keine Bewertungen
- Literature Review Head InjuryDokument5 SeitenLiterature Review Head Injuryafmzinuvouzeny100% (1)
- Fenoy 2017Dokument7 SeitenFenoy 2017syarifaNoch keine Bewertungen
- Brainsci 11 00301 v3Dokument20 SeitenBrainsci 11 00301 v3Carolina MuñozNoch keine Bewertungen
- Brain SciencesDokument20 SeitenBrain SciencesCarolina MuñozNoch keine Bewertungen
- Icp MonitoringDokument6 SeitenIcp Monitoringfarhanfarwani familyNoch keine Bewertungen
- Lee Et Al, 2022Dokument11 SeitenLee Et Al, 2022Bruno KudekenNoch keine Bewertungen
- (Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)Dokument676 Seiten(Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)atif.araf.20Noch keine Bewertungen
- Deep Brain Stimulation Research PaperDokument8 SeitenDeep Brain Stimulation Research Papergipinin0jev2100% (1)
- Good Morning EveryoneDokument6 SeitenGood Morning EveryoneRichlle CortesNoch keine Bewertungen
- 2348 0548.190064 1Dokument8 Seiten2348 0548.190064 1Ankita MohtaNoch keine Bewertungen
- Assessing The Severity of Traumatic Brain Injury-Time For A Change?Dokument12 SeitenAssessing The Severity of Traumatic Brain Injury-Time For A Change?Anonymous R6ex8BM0Noch keine Bewertungen
- MigrainDokument19 SeitenMigrainSecondhand XoxoNoch keine Bewertungen
- Disorders of Peripheral Nerves, From Beginning To EndDokument2 SeitenDisorders of Peripheral Nerves, From Beginning To EndFlea CidNoch keine Bewertungen
- Fneur 13 823189Dokument11 SeitenFneur 13 823189AlexandreNoch keine Bewertungen
- Acupuncture improves cognitive function by enhancing cerebral blood flow and mitochondrial function in dementia ratsDokument7 SeitenAcupuncture improves cognitive function by enhancing cerebral blood flow and mitochondrial function in dementia ratssovalaxNoch keine Bewertungen
- Cisternostomy: A Timely Intervention in Moderate To Severe Traumatic Brain Injuries: Rationale, Indications, and ProspectsDokument6 SeitenCisternostomy: A Timely Intervention in Moderate To Severe Traumatic Brain Injuries: Rationale, Indications, and ProspectsAtul JainNoch keine Bewertungen
- Deep Brain Stimulation in TheDokument17 SeitenDeep Brain Stimulation in Thefelix08121992Noch keine Bewertungen
- Picano 2012Dokument13 SeitenPicano 2012Jayser MatamorosNoch keine Bewertungen
- International Journal of Gerontology: Gwo-Chi Hu, Yi-Min ChenDokument5 SeitenInternational Journal of Gerontology: Gwo-Chi Hu, Yi-Min Chenluthfia ayu az zahraNoch keine Bewertungen
- Running Head: An Insight To The Twenty-Century Electroshock Therapy 1Dokument12 SeitenRunning Head: An Insight To The Twenty-Century Electroshock Therapy 1api-285356333Noch keine Bewertungen
- Catecholamine Influences On Dorsolateral Prefrontal Cortical NetworksDokument11 SeitenCatecholamine Influences On Dorsolateral Prefrontal Cortical NetworkstleticNoch keine Bewertungen
- Chemistry Tutor Job DescriptionDokument1 SeiteChemistry Tutor Job DescriptiontleticNoch keine Bewertungen
- 10 1 1 71 98Dokument10 Seiten10 1 1 71 98tleticNoch keine Bewertungen
- Chemistry Tutor Job DescriptionDokument1 SeiteChemistry Tutor Job DescriptiontleticNoch keine Bewertungen
- Effects of Music on the Brain & BodyDokument8 SeitenEffects of Music on the Brain & Bodymarkylopez23Noch keine Bewertungen
- MotivationDokument9 SeitenMotivationarsal169100% (1)
- Treating Adult Survivors of Severe Childhood Abuse and Neglect Further Development of An Integrative ModelDokument26 SeitenTreating Adult Survivors of Severe Childhood Abuse and Neglect Further Development of An Integrative ModelIoannis K. GeronikosNoch keine Bewertungen
- Psychological Science: Facial Expressions of Emotion: New Findings, New QuestionsDokument6 SeitenPsychological Science: Facial Expressions of Emotion: New Findings, New QuestionsIoana PascalNoch keine Bewertungen
- Spatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectDokument9 SeitenSpatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectRivulet1Noch keine Bewertungen
- The Takadimi System Reconsidered: Its Psychological Foundations and Some Proposals For ImprovementDokument15 SeitenThe Takadimi System Reconsidered: Its Psychological Foundations and Some Proposals For ImprovementpaperocamilloNoch keine Bewertungen
- Learning and Teaching Styles in Public SchoolsDokument12 SeitenLearning and Teaching Styles in Public SchoolsJeneffer Estal FragaNoch keine Bewertungen
- Conceptual FrameworkDokument10 SeitenConceptual FrameworkMeynard AndresNoch keine Bewertungen
- Verbal Creativity ReportDokument4 SeitenVerbal Creativity Reportjesellebalines3Noch keine Bewertungen
- IWA Duru DemiralayDokument6 SeitenIWA Duru DemiralaySem SemNoch keine Bewertungen
- Break Free - Nathaniel BrandenDokument16 SeitenBreak Free - Nathaniel Brandennbckudxtkudkuf50% (2)
- Diabettes Mellitus and Cognitive ImpairmentsDokument12 SeitenDiabettes Mellitus and Cognitive ImpairmentsPutri YunandaNoch keine Bewertungen
- Building Cooperative BehaviorDokument21 SeitenBuilding Cooperative Behaviorapi-286077776Noch keine Bewertungen
- Guidance on aptitude testingDokument10 SeitenGuidance on aptitude testingAntoNoch keine Bewertungen
- Philippians 4 13 - PPT DEFENSEDokument17 SeitenPhilippians 4 13 - PPT DEFENSESherwina Marie del RosarioNoch keine Bewertungen
- Nursing Care PlanDokument3 SeitenNursing Care PlanJustine Suico100% (1)
- Chapter 5Dokument6 SeitenChapter 5reimo12Noch keine Bewertungen
- FBM PDFDokument1 SeiteFBM PDFJeremiahgibsonNoch keine Bewertungen
- International Journal of School and Cognitive PsychologyDokument4 SeitenInternational Journal of School and Cognitive PsychologyKevin albuquerqueNoch keine Bewertungen
- Phonological Development: Majwin Nur Alam Nurul Atika Nur Khairunnisa Surya Aulia SukarmanDokument12 SeitenPhonological Development: Majwin Nur Alam Nurul Atika Nur Khairunnisa Surya Aulia SukarmanAndhy Andha Dhyan HardhyantiNoch keine Bewertungen
- Whitney Mclaughlin 2019 Ncca PresentationDokument21 SeitenWhitney Mclaughlin 2019 Ncca Presentationapi-298976119Noch keine Bewertungen
- Edid6512 - Design Prospectus - Revised - Nyeisha George-MinottDokument13 SeitenEdid6512 - Design Prospectus - Revised - Nyeisha George-Minottapi-298012003100% (1)
- Depression in Men OPED - Dr. MugambiDokument3 SeitenDepression in Men OPED - Dr. MugambiCosmas MugambiNoch keine Bewertungen
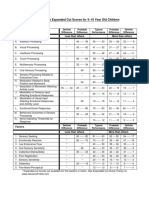
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDokument1 SeiteSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNoch keine Bewertungen
- Coaching Observation AssignmentDokument3 SeitenCoaching Observation Assignmentapi-314123459Noch keine Bewertungen
- Relapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionDokument12 SeitenRelapse Processes After The Extinction of Instrumental Learning: Renewal, Resurgence, and ReacquisitionjsaccuzzoNoch keine Bewertungen
- Theories of Motivation in ManagementDokument10 SeitenTheories of Motivation in ManagementAvani TomarNoch keine Bewertungen
- Bullying ResearchDokument7 SeitenBullying Researchaxel zeusNoch keine Bewertungen
- Quick Functional ScreeningDokument7 SeitenQuick Functional ScreeningEdison HlmNoch keine Bewertungen
- Cns Neurological ExaminationDokument26 SeitenCns Neurological ExaminationDr.P.NatarajanNoch keine Bewertungen