Das könnte Ihnen auch gefallen
- Norml Thurston County Press Release 8-24-2012Dokument2 SeitenNorml Thurston County Press Release 8-24-2012Rose Jane EiltsNoch keine Bewertungen
- Arrest and Cost Analysis of Marijuana Possession Enforcement Report 8-23-2012Dokument29 SeitenArrest and Cost Analysis of Marijuana Possession Enforcement Report 8-23-2012Rose Jane EiltsNoch keine Bewertungen
- TCNORML Lowest Enforcement Policy SampleDokument3 SeitenTCNORML Lowest Enforcement Policy SampleRose Jane EiltsNoch keine Bewertungen
- Kent 2010 Schedule 16 SAO Report Ar1006406Dokument2 SeitenKent 2010 Schedule 16 SAO Report Ar1006406Rose Jane EiltsNoch keine Bewertungen
- Bremerton 2010 Schedule 16 SAO Report Ar1006433Dokument3 SeitenBremerton 2010 Schedule 16 SAO Report Ar1006433Rose Jane EiltsNoch keine Bewertungen
- Public Hearing PCMedical Marijuana Notice June 2012Dokument6 SeitenPublic Hearing PCMedical Marijuana Notice June 2012Rose Jane EiltsNoch keine Bewertungen
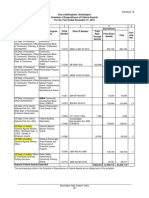
- Thurston County 2010 Schedule 16Dokument9 SeitenThurston County 2010 Schedule 16Rose Jane EiltsNoch keine Bewertungen
- Olympia 2010 Schedule 16 SAO Ar1006319Dokument2 SeitenOlympia 2010 Schedule 16 SAO Ar1006319Rose Jane EiltsNoch keine Bewertungen
- Tacoma 2010 Schedule 16 SAO Ar1006397Dokument14 SeitenTacoma 2010 Schedule 16 SAO Ar1006397Rose Jane EiltsNoch keine Bewertungen
- Spokane 2010 Schedule 16 SAO Report Ar1006365Dokument7 SeitenSpokane 2010 Schedule 16 SAO Report Ar1006365Rose Jane EiltsNoch keine Bewertungen
- City of Lacey 2010 Sched 16Dokument2 SeitenCity of Lacey 2010 Sched 16Rose Jane EiltsNoch keine Bewertungen
- Everett 2010 Schedule 16 SAO Ar1006420-2Dokument2 SeitenEverett 2010 Schedule 16 SAO Ar1006420-2Rose Jane EiltsNoch keine Bewertungen
- Lacey Moratorium Mar 8 2012Dokument13 SeitenLacey Moratorium Mar 8 2012Rose Jane EiltsNoch keine Bewertungen
- Ellensburg 4611 Agenda Report On Moratorium To Public Access CentersDokument2 SeitenEllensburg 4611 Agenda Report On Moratorium To Public Access CentersRose Jane EiltsNoch keine Bewertungen
- Bellingham 2010 Schedule 16 SAO Report Ar1006404Dokument3 SeitenBellingham 2010 Schedule 16 SAO Report Ar1006404Rose Jane EiltsNoch keine Bewertungen
- Lacey Ordinance - Medical Marijuana Collective Gardens 02.02Dokument1 SeiteLacey Ordinance - Medical Marijuana Collective Gardens 02.02Rose Jane EiltsNoch keine Bewertungen
- Date: To: From: Subject:: Page 1Dokument5 SeitenDate: To: From: Subject:: Page 1Rose Jane EiltsNoch keine Bewertungen
- Ellensburg 4611 Med Marijuana Moratorium Extension OrdDokument7 SeitenEllensburg 4611 Med Marijuana Moratorium Extension OrdRose Jane EiltsNoch keine Bewertungen
- Update - City Moratoria On Medical Cannabis Collective GardensDokument4 SeitenUpdate - City Moratoria On Medical Cannabis Collective GardensRose Jane EiltsNoch keine Bewertungen
- Seattle Ord 123661Dokument8 SeitenSeattle Ord 123661Rose Jane EiltsNoch keine Bewertungen
- Lacey Moratorium Mar 8 2012Dokument13 SeitenLacey Moratorium Mar 8 2012Rose Jane EiltsNoch keine Bewertungen
- Ellensburg 4610 Extension Collective GardensDokument8 SeitenEllensburg 4610 Extension Collective GardensRose Jane EiltsNoch keine Bewertungen
- 2012 02 13 Regulation of Island Alternative Medicine Collective Gardens in The City of LangleyDokument61 Seiten2012 02 13 Regulation of Island Alternative Medicine Collective Gardens in The City of LangleyRose Jane EiltsNoch keine Bewertungen
- Bullet Points For Moratoriums On Medical Cannabis Collective GardensDokument1 SeiteBullet Points For Moratoriums On Medical Cannabis Collective GardensRose Jane EiltsNoch keine Bewertungen
- Lacey PCMemoMariCommunityGrows (Upton Comments) Final2Dokument20 SeitenLacey PCMemoMariCommunityGrows (Upton Comments) Final2Rose Jane EiltsNoch keine Bewertungen
- Lacey Proposed Application - 02.02Dokument3 SeitenLacey Proposed Application - 02.02Rose Jane EiltsNoch keine Bewertungen
- Lacey Planning Commiss Agenda 02-21-12Dokument1 SeiteLacey Planning Commiss Agenda 02-21-12Rose Jane EiltsNoch keine Bewertungen
- Lacey Draft Medical Mari Ordinance February 2012Dokument12 SeitenLacey Draft Medical Mari Ordinance February 2012Rose Jane EiltsNoch keine Bewertungen
- Shoreline Ord0625Dokument34 SeitenShoreline Ord0625Rose Jane EiltsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- VOL. 354, MARCH 14, 2001 339 People vs. Go: - First DivisionDokument15 SeitenVOL. 354, MARCH 14, 2001 339 People vs. Go: - First DivisionMichelle Joy ItableNoch keine Bewertungen
- YseDokument3 SeitenYseHarris VickyNoch keine Bewertungen
- Destination 2 (12A)Dokument3 SeitenDestination 2 (12A)oldhastonian100% (1)
- Plaintiffs' Motion To Strike Affidavits of Brian P WattDokument18 SeitenPlaintiffs' Motion To Strike Affidavits of Brian P WattJanet and James100% (7)
- Methods and Techniques for Collecting Intelligence InformationDokument2 SeitenMethods and Techniques for Collecting Intelligence InformationrenjomarNoch keine Bewertungen
- 2022 S C M R 1846Dokument9 Seiten2022 S C M R 1846Fuck YouNoch keine Bewertungen
- Ajay Gupta and Oakbay Investments Delighted With Affidavit From Pravin GordhanDokument3 SeitenAjay Gupta and Oakbay Investments Delighted With Affidavit From Pravin GordhaneNCA.comNoch keine Bewertungen
- Judicial Review of Religious Conversion CertificatesDokument67 SeitenJudicial Review of Religious Conversion CertificatesTetuan Abdullah Hakim & AhmadNoch keine Bewertungen
- UcDokument9 SeitenUcBrunxAlabastroNoch keine Bewertungen
- Shabtay Versus Levy SynagogueDokument46 SeitenShabtay Versus Levy SynagogueLos Angeles Daily News100% (1)
- Civil Service Examination Form No. 100 Revised September 2016 PDFDokument2 SeitenCivil Service Examination Form No. 100 Revised September 2016 PDFVeronica NavarroNoch keine Bewertungen
- Not PrecedentialDokument6 SeitenNot PrecedentialScribd Government DocsNoch keine Bewertungen
- AMA Computer College v. Garcia, April 14, 2008Dokument20 SeitenAMA Computer College v. Garcia, April 14, 2008Felix TumbaliNoch keine Bewertungen
- Lect 1 Overview of Taxation 2017Dokument68 SeitenLect 1 Overview of Taxation 2017Devisudha ThanaseelanNoch keine Bewertungen
- General Power of AttorneyDokument2 SeitenGeneral Power of Attorneymary ann pacamparaNoch keine Bewertungen
- Comparison of CNCC and CECC 2006Dokument10 SeitenComparison of CNCC and CECC 2006AJBhouseNoch keine Bewertungen
- Filed Court Document Motion For ReconsiderationDokument14 SeitenFiled Court Document Motion For Reconsiderationleenav-1Noch keine Bewertungen
- Notice To Court and All Court OfficersDokument27 SeitenNotice To Court and All Court OfficersMisory96% (113)
- IntroDokument14 SeitenIntroveercasanovaNoch keine Bewertungen
- TechStars Series AA Amended and Restated Articles of IncorporationDokument15 SeitenTechStars Series AA Amended and Restated Articles of IncorporationhadryNoch keine Bewertungen
- BWI 6th Synthesis Report v3.2 FINAL enDokument5 SeitenBWI 6th Synthesis Report v3.2 FINAL enJulio Best Setiyawan100% (1)
- Advisory Calendar of Barangay Mandatory DeliverablesDokument9 SeitenAdvisory Calendar of Barangay Mandatory DeliverablesJo ReyesNoch keine Bewertungen
- Motion For Leave SAMPLEDokument2 SeitenMotion For Leave SAMPLERex TrayaNoch keine Bewertungen
- G.R. No. 237133Dokument11 SeitenG.R. No. 237133MarkNoch keine Bewertungen
- Letter of RequestDokument1 SeiteLetter of RequestJohn Rey Bantay RodriguezNoch keine Bewertungen
- Separation of Powers: Concept Note No. 13Dokument17 SeitenSeparation of Powers: Concept Note No. 13Mark GoNoch keine Bewertungen
- Case Study Related To Insider TradingDokument4 SeitenCase Study Related To Insider TradingSylvie KathuriaNoch keine Bewertungen
- DL101-Module9-International RegistrationDokument48 SeitenDL101-Module9-International RegistrationMizra BezNoch keine Bewertungen
- CG Assignment 1Dokument13 SeitenCG Assignment 1arslan0989Noch keine Bewertungen
- Position PaperDokument2 SeitenPosition PaperAndrew AndrewNoch keine Bewertungen