Das könnte Ihnen auch gefallen
- Pediatric Antibiotic Dosing Card 2012Dokument2 SeitenPediatric Antibiotic Dosing Card 2012yoshilimsiacoshigyoNoch keine Bewertungen
- KAPS Paper 2 Sample 2Dokument39 SeitenKAPS Paper 2 Sample 2piNoch keine Bewertungen
- Practice Test # 01 (Past Year PPSC Paper) : JOIN IS at WHATSAPP +92 333 2243031Dokument19 SeitenPractice Test # 01 (Past Year PPSC Paper) : JOIN IS at WHATSAPP +92 333 2243031Saima ShehzadNoch keine Bewertungen
- Essentials of Microbiology 1st Edition PDFDokument648 SeitenEssentials of Microbiology 1st Edition PDFJohn Khna100% (1)
- Clindamycin Drug StudyDokument3 SeitenClindamycin Drug StudygoyaNoch keine Bewertungen
- Antimicrobial Susceptibility Testing PDFDokument19 SeitenAntimicrobial Susceptibility Testing PDFdatitoxNoch keine Bewertungen
- LincosamidesDokument19 SeitenLincosamidesManahil RiazNoch keine Bewertungen
- MedicamenteDokument89 SeitenMedicamentenicole_22100% (4)
- Cleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165Dokument14 SeitenCleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165krizelNoch keine Bewertungen
- Clindamycin Gel Is Used ForDokument4 SeitenClindamycin Gel Is Used Forgustavo83_prNoch keine Bewertungen
- Cleocin Clindamycin Phosphate Vaginal Cream, USPDokument19 SeitenCleocin Clindamycin Phosphate Vaginal Cream, USPAurelio Villanueva ValleNoch keine Bewertungen
- Clindamycin ANMFv1.0 20220609Dokument3 SeitenClindamycin ANMFv1.0 20220609tom.condon.02Noch keine Bewertungen
- Kaptin Antidiarrheal Susp Patient Information LeafletDokument1 SeiteKaptin Antidiarrheal Susp Patient Information Leafletpharmacia1.comNoch keine Bewertungen
- Canine Glaucoma - Medical and Surgical Traetment OptionsDokument6 SeitenCanine Glaucoma - Medical and Surgical Traetment OptionsRochiWinchesterNoch keine Bewertungen
- Klindam Acne Solution Clindamycin Phosphate Prime Pharmaceutical SDN BHD 24 OCT 2017 ENG 1Dokument1 SeiteKlindam Acne Solution Clindamycin Phosphate Prime Pharmaceutical SDN BHD 24 OCT 2017 ENG 1TQINNoch keine Bewertungen
- Clobetasol CreamDokument9 SeitenClobetasol CreamGiulianospharmacyNoch keine Bewertungen
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDokument3 SeitenSummary of Product Characteristics: 4.1 Therapeutic IndicationsasdwasdNoch keine Bewertungen
- Clonidine Hydrochloride InjectionDokument9 SeitenClonidine Hydrochloride InjectionJan Nicole SeriñaNoch keine Bewertungen
- Ludura Lulitec CreamDokument1 SeiteLudura Lulitec CreamGaurav NNoch keine Bewertungen
- Clindamycin Uses, Dosage & Side EffectsDokument5 SeitenClindamycin Uses, Dosage & Side Effectstarun yadavNoch keine Bewertungen
- Pedoman Penggunaan Antibiotik Pada PasienDokument5 SeitenPedoman Penggunaan Antibiotik Pada PasienErvina Lie100% (1)
- Clindamycin: A Drug Study OnDokument7 SeitenClindamycin: A Drug Study Ondanica grace gubaNoch keine Bewertungen
- Micafungin Sodium-100mg Powder For Solution For InfusionDokument6 SeitenMicafungin Sodium-100mg Powder For Solution For InfusionMd. Abdur RahmanNoch keine Bewertungen
- Cimetidine, A Review of The Recent Developments and Reports in Cutaneous MedicineDokument7 SeitenCimetidine, A Review of The Recent Developments and Reports in Cutaneous MedicineFikry AwaluddinNoch keine Bewertungen
- Diphenhydramine Hydrochloride (Benadryl) 50mg/1mlDokument6 SeitenDiphenhydramine Hydrochloride (Benadryl) 50mg/1ml'SheenMarkReal'Noch keine Bewertungen
- ClindamycinDokument2 SeitenClindamycinarkee_06Noch keine Bewertungen
- Acute Poisoning Guidelines.Dokument7 SeitenAcute Poisoning Guidelines.Manoj KumarNoch keine Bewertungen
- Medication Safety IssuesDokument43 SeitenMedication Safety IssuesSarah NurAzkia El RoesmanNoch keine Bewertungen
- SMPC Polyderm CreamDokument6 SeitenSMPC Polyderm CreamAxmed MaxamedNoch keine Bewertungen
- GlimepirideDokument12 SeitenGlimepirideMobahil AhmadNoch keine Bewertungen
- Daivonex Cream PI - LPS-11-045Dokument5 SeitenDaivonex Cream PI - LPS-11-045Hesam AhmadianNoch keine Bewertungen
- SucralfateDokument3 SeitenSucralfateHaifa HanifahNoch keine Bewertungen
- Mot Ilium TabDokument11 SeitenMot Ilium TabChandra FatmaNoch keine Bewertungen
- TbactDokument7 SeitenTbactVinay KumarNoch keine Bewertungen
- A New Antibiotic Treats Serious Skin Infections.22 PDFDokument1 SeiteA New Antibiotic Treats Serious Skin Infections.22 PDFL.E.O Antonio Kim Huerta AlcántaraNoch keine Bewertungen
- Clindamycin - ClinicalKeyDokument78 SeitenClindamycin - ClinicalKeyTRI SETYA NINGSIHNoch keine Bewertungen
- Metabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSDokument5 SeitenMetabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSMahmoud khedrNoch keine Bewertungen
- How I Treat Methicillin-Resistant Staphylococcal Pyoderma - WSAVA 2014 Congress - VINDokument5 SeitenHow I Treat Methicillin-Resistant Staphylococcal Pyoderma - WSAVA 2014 Congress - VINAdil HussainNoch keine Bewertungen
- Jurnal Trilac (Triamcinolone)Dokument7 SeitenJurnal Trilac (Triamcinolone)Muhammad IqbalNoch keine Bewertungen
- Klint Klint: Tablets/Injection SuspensionDokument1 SeiteKlint Klint: Tablets/Injection SuspensionibtesamNoch keine Bewertungen
- A, A-Diphenyl-1-Piperidinebutyramide Monohydrochloride, Is A Synthetic Antidiarrheal ForDokument10 SeitenA, A-Diphenyl-1-Piperidinebutyramide Monohydrochloride, Is A Synthetic Antidiarrheal ForDevi SaputriNoch keine Bewertungen
- Abram Study NotesDokument6 SeitenAbram Study Notesteeman2Noch keine Bewertungen
- Product MonographDokument15 SeitenProduct MonographAryl LyraNoch keine Bewertungen
- ReferatkuDokument9 SeitenReferatku5a171Noch keine Bewertungen
- Flagystatin SG 1222Dokument15 SeitenFlagystatin SG 1222MarjMalubayArriolaNoch keine Bewertungen
- Diethyl Carb AmazineDokument7 SeitenDiethyl Carb AmazineMuhammad Fadhil IlhamiNoch keine Bewertungen
- DESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDDokument7 SeitenDESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDRizky Akbar LatifNoch keine Bewertungen
- Clostridium Difficile Guideline - UMMCDokument5 SeitenClostridium Difficile Guideline - UMMCdamondouglas100% (3)
- ArtesunateDokument4 SeitenArtesunateSyifa Ari SuciyaniNoch keine Bewertungen
- 017407s034lbl PDFDokument8 Seiten017407s034lbl PDFNexi anessaNoch keine Bewertungen
- Antiamoebic DrugsDokument23 SeitenAntiamoebic DrugsMoe KebabNoch keine Bewertungen
- Клензит-С MS.ru.enDokument6 SeitenКлензит-С MS.ru.enAhins RobinNoch keine Bewertungen
- The Poisoning in Children 5Dokument4 SeitenThe Poisoning in Children 5Rick RoxNoch keine Bewertungen
- Banocide and Banocide ForteDokument10 SeitenBanocide and Banocide ForteJosephNoch keine Bewertungen
- Honey and LemonDokument7 SeitenHoney and LemontangxiaomeimayNoch keine Bewertungen
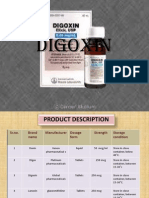
- DigoxinDokument20 SeitenDigoxinAbdulRehmanChaudaryNoch keine Bewertungen
- KAPS Paper 2 Sample 2Dokument39 SeitenKAPS Paper 2 Sample 2Shimaa AbdouNoch keine Bewertungen
- Msds NacloDokument4 SeitenMsds NacloChern YuanNoch keine Bewertungen
- Klindam Capsule Clindamycin Hydrochloride Prime Pharmaceutical SDN BHD 24 OCT 2017 ENG 1Dokument1 SeiteKlindam Capsule Clindamycin Hydrochloride Prime Pharmaceutical SDN BHD 24 OCT 2017 ENG 1TQINNoch keine Bewertungen
- Triamcinolone (Topical) - Drug InformationDokument5 SeitenTriamcinolone (Topical) - Drug InformationMauricio Sv0% (1)
- CLARITHROMYCINDokument3 SeitenCLARITHROMYCINCay SevillaNoch keine Bewertungen
- TRETINOIN-tretinoin Cream Actavis Pharma, IncDokument9 SeitenTRETINOIN-tretinoin Cream Actavis Pharma, IncListiana RachmanNoch keine Bewertungen
- Drugs Used in Urinary Tract InfectionDokument20 SeitenDrugs Used in Urinary Tract InfectionShrishti KansaraNoch keine Bewertungen
- Bioautography Detection in Thin-Layer ChromatographyDokument8 SeitenBioautography Detection in Thin-Layer ChromatographyTonnyLeiteNoch keine Bewertungen
- Daftar Dosis ObatDokument3 SeitenDaftar Dosis Obatnindy vidyaniNoch keine Bewertungen
- Microbiology Newlab سالى ابو السعود 0864986Dokument1 SeiteMicrobiology Newlab سالى ابو السعود 0864986Mohammed TahounNoch keine Bewertungen
- N Vitro Evaluation of Antimicrobial and Antioxidant Activity of Ragon 'S Blood Tree Racaena Cinnabari Alf.f. of Ocotra Sland EmenDokument7 SeitenN Vitro Evaluation of Antimicrobial and Antioxidant Activity of Ragon 'S Blood Tree Racaena Cinnabari Alf.f. of Ocotra Sland EmensugianliNoch keine Bewertungen
- Pediatric Medication Dosing GuildelinesDokument2 SeitenPediatric Medication Dosing GuildelinesMuhammad ZeeshanNoch keine Bewertungen
- Host Parasite Relationship NotesDokument6 SeitenHost Parasite Relationship NotesGrace ValenciaNoch keine Bewertungen
- Hasil Peta Kuman Rumah Sakit Urip Smoharjo: Pseudomonas NO Hasil AntibiotikDokument8 SeitenHasil Peta Kuman Rumah Sakit Urip Smoharjo: Pseudomonas NO Hasil AntibiotikNIDANoch keine Bewertungen
- Drug Tabulation of Ampicillin SulbactamDokument1 SeiteDrug Tabulation of Ampicillin SulbactamJobie CasipongNoch keine Bewertungen
- Usage of Antibiotics in ICU (English)Dokument13 SeitenUsage of Antibiotics in ICU (English)V15CERA FK UNANDNoch keine Bewertungen
- Care Plan Risk For Infection 2Dokument3 SeitenCare Plan Risk For Infection 2Chander KantaNoch keine Bewertungen
- Hepatic EncephalopathyDokument3 SeitenHepatic EncephalopathySuhas KandeNoch keine Bewertungen
- AttachmentDokument62 SeitenAttachmentlevely rizkiNoch keine Bewertungen
- Evaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalDokument6 SeitenEvaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalEditor IJTSRDNoch keine Bewertungen
- Medical ChemDokument1 SeiteMedical ChemGkdhdhdgdgidNoch keine Bewertungen
- مدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFDokument232 Seitenمدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFنورهانعزالدين100% (1)
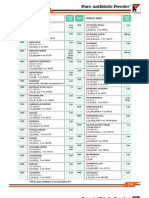
- Pure Antibiotic PowderDokument2 SeitenPure Antibiotic PowderTitan BiotechNoch keine Bewertungen
- Ocular Antibiotics and Anti-Infectives: Regis P. Kowalski, MS, M (ASCP)Dokument16 SeitenOcular Antibiotics and Anti-Infectives: Regis P. Kowalski, MS, M (ASCP)Maria SpatariNoch keine Bewertungen
- Updates Surgical WardDokument3 SeitenUpdates Surgical WardBupaint ArtgalleryNoch keine Bewertungen
- Localized Treatment of Chronic Buruli Ulcer With v1 Id1035 PDFDokument3 SeitenLocalized Treatment of Chronic Buruli Ulcer With v1 Id1035 PDFAnonymous e3TFin8884Noch keine Bewertungen
- Spesialite Golongan AntibiotikDokument5 SeitenSpesialite Golongan AntibiotikBella LunaNoch keine Bewertungen
- (260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPDokument43 Seiten(260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPreginaNoch keine Bewertungen
- Andrographis Paniculata WHO Monographs On Selected Medicinal Plants Volume 2Dokument13 SeitenAndrographis Paniculata WHO Monographs On Selected Medicinal Plants Volume 2JY MarNoch keine Bewertungen
- The Neglected Natural Resources of Goa - For MonographDokument34 SeitenThe Neglected Natural Resources of Goa - For MonographnandkamatNoch keine Bewertungen
- Felix Khuluza & Lutz Heide 18. March - 29. April 2014: PHA 406 Drug and Medical Supplies Management IIDokument20 SeitenFelix Khuluza & Lutz Heide 18. March - 29. April 2014: PHA 406 Drug and Medical Supplies Management IIShoaib BiradarNoch keine Bewertungen
- Antimicrobial Activity From Red Sea CoralDokument7 SeitenAntimicrobial Activity From Red Sea CoralAnggreiniRupidaraNoch keine Bewertungen