Das könnte Ihnen auch gefallen
- NCP Risk For InfectionDokument6 SeitenNCP Risk For InfectionCazze SunioNoch keine Bewertungen
- Velez College of Nursing F. Ramos Street, Cebu CityDokument57 SeitenVelez College of Nursing F. Ramos Street, Cebu Cityinah krizia lagueNoch keine Bewertungen
- Complications in PregnancyDokument36 SeitenComplications in PregnancyJADE PATEGANoch keine Bewertungen
- Emj Cases : Questions For Case 1Dokument8 SeitenEmj Cases : Questions For Case 1Azmyza Azmy100% (1)
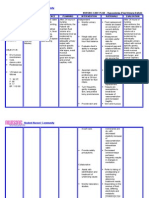
- NCP PlanningDecreased in Cardiac Output Related To Low Hemoglobin and Hematocrit CountDokument6 SeitenNCP PlanningDecreased in Cardiac Output Related To Low Hemoglobin and Hematocrit CountMabelle SorianoNoch keine Bewertungen
- Impaired Gas Exchange NCPDokument3 SeitenImpaired Gas Exchange NCPRomel BaliliNoch keine Bewertungen
- NCP MeningitisDokument2 SeitenNCP MeningitisARISNoch keine Bewertungen
- Nursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short TermDokument3 SeitenNursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short Termgeng gengNoch keine Bewertungen
- 6B Pregnant and Lactacting WomenDokument3 Seiten6B Pregnant and Lactacting Womenmo'niqueNoch keine Bewertungen
- Nursing Care Plan DMDokument8 SeitenNursing Care Plan DMnikaaraaaNoch keine Bewertungen
- Buergers Power PointDokument16 SeitenBuergers Power PointYan VencerNoch keine Bewertungen
- Spina Bifida, Meningocele MyelomeningoceleDokument1 SeiteSpina Bifida, Meningocele MyelomeningocelesmilingstarsNoch keine Bewertungen
- Ineffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.Dokument6 SeitenIneffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.SAROL, RYAN CHRISTIAN B.Noch keine Bewertungen
- Intussusception: PathophysiologyDokument8 SeitenIntussusception: PathophysiologyNaufal AndaluNoch keine Bewertungen
- NCP PROPER Cough CoroDokument3 SeitenNCP PROPER Cough Corokonoha2214839100% (2)
- Now, Try Some Big Leap.: Keep GoingDokument2 SeitenNow, Try Some Big Leap.: Keep GoingShyla ManguiatNoch keine Bewertungen
- NCP Meningitis Sure NaniDokument2 SeitenNCP Meningitis Sure NaniARISNoch keine Bewertungen
- Nursing Care Plan For LYING inDokument4 SeitenNursing Care Plan For LYING inKarissa CiprianoNoch keine Bewertungen
- NCPsDokument13 SeitenNCPsRocel DevillesNoch keine Bewertungen
- CJ C J CJ CJ Cî CJ CJ C C ! "! Cî C Ë # C Ë # CJ$ C C 0 "% C C & C C C Ë Î C "' (C Ëj "ËjDokument105 SeitenCJ C J CJ CJ Cî CJ CJ C C ! "! Cî C Ë # C Ë # CJ$ C C 0 "% C C & C C C Ë Î C "' (C Ëj "ËjShirin Forbes Aquino100% (2)
- NCP Risk For InjuryDokument2 SeitenNCP Risk For Injurycristina_galang_2Noch keine Bewertungen
- NCP of Endometrical CancerDokument2 SeitenNCP of Endometrical CancerFrando kennethNoch keine Bewertungen
- Premenstrual Dysphoric DisorderDokument11 SeitenPremenstrual Dysphoric Disorderapi-3764215Noch keine Bewertungen
- APOLONIO, JC - Natural Theory - Thomas AquinasDokument3 SeitenAPOLONIO, JC - Natural Theory - Thomas AquinasJustin ApolonioNoch keine Bewertungen
- Group 6 Group Case Study DONEDokument5 SeitenGroup 6 Group Case Study DONEE.R.ONoch keine Bewertungen
- CHN - IdbDokument11 SeitenCHN - IdbCharm RoweNoch keine Bewertungen
- NCPDokument3 SeitenNCPJoevelyn LaynoNoch keine Bewertungen
- Family Nursing Care Plan ChapterDokument1 SeiteFamily Nursing Care Plan ChapterJhe PangsNoch keine Bewertungen
- NCP (Postpartum Hemmorhage)Dokument3 SeitenNCP (Postpartum Hemmorhage)Anne DyNoch keine Bewertungen
- Ongoing AppraisalDokument2 SeitenOngoing AppraisalLouisa Marie MirandaNoch keine Bewertungen
- Uterine Myoma Case Study Group A FinalDokument88 SeitenUterine Myoma Case Study Group A Finallowell cerezoNoch keine Bewertungen
- Activity IntoleranceDokument1 SeiteActivity IntoleranceAndrea Francesca SantosNoch keine Bewertungen
- Cell Ab ActivitiesDokument7 SeitenCell Ab ActivitiesJanelle Cabida Supnad100% (1)
- NCP LeprosyDokument3 SeitenNCP LeprosyJane MinNoch keine Bewertungen
- Acute Tonsil Lo PharyngitisDokument27 SeitenAcute Tonsil Lo PharyngitisCheysser Alagao50% (2)
- Impaired Tissue PerfusionDokument2 SeitenImpaired Tissue PerfusionLyka Mae Imbat - PacnisNoch keine Bewertungen
- NSO - Adam's Forward Bend TestDokument2 SeitenNSO - Adam's Forward Bend TestMaha AmilNoch keine Bewertungen
- NCP RiskDokument2 SeitenNCP RiskNorries Jonell CaballarNoch keine Bewertungen
- Fluid Volume DeficitDokument2 SeitenFluid Volume DeficitpeternohibiNoch keine Bewertungen
- Acute Lymphocytic Leukemia Treatment PaperDokument18 SeitenAcute Lymphocytic Leukemia Treatment Paperapi-282231236Noch keine Bewertungen
- Nursing Care Plan: Sweating Temperature Rigors Nausea Vomiting Diarrhoea Lethargy MalaiseDokument1 SeiteNursing Care Plan: Sweating Temperature Rigors Nausea Vomiting Diarrhoea Lethargy Malaise06eltianNoch keine Bewertungen
- Case Pres AutosavedDokument21 SeitenCase Pres AutosavedJaysellePuguonTabijeNoch keine Bewertungen
- NCP Episiotomy WoundDokument3 SeitenNCP Episiotomy WoundJP2001Noch keine Bewertungen
- Reflective Journal 1Dokument4 SeitenReflective Journal 1api-365605511Noch keine Bewertungen
- Hypovolemia (Fluid Deficit)Dokument2 SeitenHypovolemia (Fluid Deficit)Lyn Reyes100% (1)
- Flail Chest (Tayug)Dokument25 SeitenFlail Chest (Tayug)Adrian MallarNoch keine Bewertungen
- GastroschisisDokument19 SeitenGastroschisiskunaidongNoch keine Bewertungen
- Silliman University: Nursing Care Plan On Preeclampsia With Severe FeaturesDokument8 SeitenSilliman University: Nursing Care Plan On Preeclampsia With Severe FeaturesRyan Robert V. VentoleroNoch keine Bewertungen
- Case Study CSDokument21 SeitenCase Study CSThessa Lonica GarciaNoch keine Bewertungen
- NCP in PediaDokument3 SeitenNCP in Pediajoister011750% (2)
- NCP 1Dokument6 SeitenNCP 1Maedine Urbano-BrionesNoch keine Bewertungen
- Fatigue and Back Pain NCP PresentationDokument18 SeitenFatigue and Back Pain NCP PresentationTine Guibao100% (1)
- Nursing Care Plan: MDH Ob/GyneDokument10 SeitenNursing Care Plan: MDH Ob/GyneTrisha Dianne RaquenioNoch keine Bewertungen
- Assessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationDokument3 SeitenAssessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationCrissa AngelNoch keine Bewertungen
- Cord ProlapseDokument2 SeitenCord ProlapseUsman Ali AkbarNoch keine Bewertungen
- OxytocinDokument1 SeiteOxytocinjhinNoch keine Bewertungen
- Diabetes Mellitus NCPDokument7 SeitenDiabetes Mellitus NCPjfgnzls182892% (12)
- DM NCPDokument7 SeitenDM NCPMichael Anthony Cardenas Macaballug67% (3)
- DM Care PlanDokument9 SeitenDM Care PlanHarish Kumar KumawatNoch keine Bewertungen
- Nursing Care PlansDokument6 SeitenNursing Care PlansTwobee Kriz LeghidNoch keine Bewertungen
- NCP CSDokument7 SeitenNCP CSTwobee Kriz LeghidNoch keine Bewertungen
- Nursing Care PlansDokument6 SeitenNursing Care PlansTwobee Kriz LeghidNoch keine Bewertungen
- ECLAMPSIADokument1 SeiteECLAMPSIATwobee Kriz LeghidNoch keine Bewertungen
- Preparation Outline (Informative Speech)Dokument5 SeitenPreparation Outline (Informative Speech)Adam ShamsuNoch keine Bewertungen
- Unlocking The Hidden Potential of Plant Proteins Using Solid State Fermentation EnzymesDokument7 SeitenUnlocking The Hidden Potential of Plant Proteins Using Solid State Fermentation EnzymesInternational Aquafeed magazineNoch keine Bewertungen
- Bio 270 Lecture 10 University of TorontoDokument24 SeitenBio 270 Lecture 10 University of TorontoJD BaruaNoch keine Bewertungen
- 10 Essential Pillars of Employee EngagementDokument71 Seiten10 Essential Pillars of Employee EngagementJorge Olvera100% (1)
- DR Fuhrman's 6-Week Eat To Live and 12-Week Reverse Diabetic PlanDokument5 SeitenDR Fuhrman's 6-Week Eat To Live and 12-Week Reverse Diabetic PlanCyndi McKenna89% (9)
- An Objective Comparison of Chocolate Milk and Surge RecoveryDokument5 SeitenAn Objective Comparison of Chocolate Milk and Surge RecoveryTony MecherkanyNoch keine Bewertungen
- Interchange: Practice For The TOEIC Test For 2ADokument29 SeitenInterchange: Practice For The TOEIC Test For 2ARolando100% (1)
- MITxTreme-World's Fastest Body Transformation ProgramDokument56 SeitenMITxTreme-World's Fastest Body Transformation Programalekad65Noch keine Bewertungen
- Food and Nutrition Research InstituteDokument13 SeitenFood and Nutrition Research InstituteCarla Grace CentenoNoch keine Bewertungen
- Plant NutrientsDokument22 SeitenPlant NutrientslastoutriderNoch keine Bewertungen
- Lesson 1 AssessmentDokument3 SeitenLesson 1 Assessmentapi-377095434Noch keine Bewertungen
- Vitamin B12 in Vegetarian DietsDokument4 SeitenVitamin B12 in Vegetarian DietsJesica DiazNoch keine Bewertungen
- Yang Sheng Fa-Lotus Nei GongDokument9 SeitenYang Sheng Fa-Lotus Nei GongSean Brown100% (2)
- A2 Flexibility TrainingDokument6 SeitenA2 Flexibility TrainingClayesmorePENoch keine Bewertungen
- Other Trace Elements: Forrest H. NielsenDokument23 SeitenOther Trace Elements: Forrest H. NielsenBeatrizCamposNoch keine Bewertungen
- Take It Off Keep It OffDokument228 SeitenTake It Off Keep It OffDawson EllisonNoch keine Bewertungen
- Bicycling 2011-01-02 VinyDokument100 SeitenBicycling 2011-01-02 VinyJean VegasNoch keine Bewertungen
- ملزمة انكليزي رابعDokument51 Seitenملزمة انكليزي رابع3bdalmalikwesam1Noch keine Bewertungen
- Eye Formula Trifold BrochureDokument2 SeitenEye Formula Trifold BrochureCherry San DiegoNoch keine Bewertungen
- Nourish Chapter 1 and 2Dokument45 SeitenNourish Chapter 1 and 2paul onetNoch keine Bewertungen
- DigestionDokument5 SeitenDigestionRashri SharmaNoch keine Bewertungen
- Infinite Book Summary 1621372498707Dokument11 SeitenInfinite Book Summary 1621372498707sabiou amadouNoch keine Bewertungen
- Health Related Physical FitnessDokument5 SeitenHealth Related Physical Fitnessprajapati1983Noch keine Bewertungen
- Human Nutrition Exam.Dokument5 SeitenHuman Nutrition Exam.Anonymous WUZ6mj67% (3)
- Booklet Dayak OnionDokument48 SeitenBooklet Dayak OnionDirayati HanifahNoch keine Bewertungen
- 8 Healthy Smoothie RecipesDokument8 Seiten8 Healthy Smoothie RecipesUdayNoch keine Bewertungen
- Mountain Dog ArmsDokument12 SeitenMountain Dog ArmsÂdâm Jônês90% (10)
- Wainfleet Exotic Animal Bylaw 2018Dokument18 SeitenWainfleet Exotic Animal Bylaw 2018Dave JohnsonNoch keine Bewertungen
- 2016 Guía Europea de Prevención de La Enfermedad Cardiovascular en La PrácticaDokument68 Seiten2016 Guía Europea de Prevención de La Enfermedad Cardiovascular en La PrácticaPaty Alatorre IcazaNoch keine Bewertungen
- Anti Inflammatory Diets 2015Dokument9 SeitenAnti Inflammatory Diets 2015twice againNoch keine Bewertungen