Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Comparison of Drug-Induced Sleep Endoscopy Ver2Dokument34 SeitenComparison of Drug-Induced Sleep Endoscopy Ver2thtklNoch keine Bewertungen
- Sleep Medicine ReviewsDokument16 SeitenSleep Medicine ReviewsCami ElenaNoch keine Bewertungen
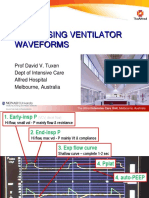
- Ventilator Waveforms DavidTuxen2Dokument41 SeitenVentilator Waveforms DavidTuxen2Syed Shahrul Naz Syed100% (1)
- Practice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateDokument18 SeitenPractice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateMaulana 'Sugat' Iskandar DinataNoch keine Bewertungen
- Obstructive Sleep Aponea SurgeriesDokument638 SeitenObstructive Sleep Aponea Surgerieswillyoueverlovemenk100% (2)
- Short Diagnosis Report: PatientDokument6 SeitenShort Diagnosis Report: PatientCarmen JurcoaneNoch keine Bewertungen
- Ambu Sleepmate Poster PDFDokument1 SeiteAmbu Sleepmate Poster PDFMinh Triết LêNoch keine Bewertungen
- Cpap BipapDokument3 SeitenCpap BipapAmalinaNoch keine Bewertungen
- OSADokument5 SeitenOSAtherese BNoch keine Bewertungen
- Mechanisms and Predisposing Factors For Sleep-Related Breathing Disorders in Children - UpToDateDokument30 SeitenMechanisms and Predisposing Factors For Sleep-Related Breathing Disorders in Children - UpToDateTran Trang AnhNoch keine Bewertungen
- Clinical Guidelines For CPAP TitrationDokument15 SeitenClinical Guidelines For CPAP Titrationsavvy_as_98Noch keine Bewertungen
- Management of Upper Airway DisorderDokument46 SeitenManagement of Upper Airway DisorderSahana Rangarajan100% (1)
- Catástrofes Perioperatorias 2019 PDFDokument415 SeitenCatástrofes Perioperatorias 2019 PDFmariogutiNoch keine Bewertungen
- Manual Dream StarDokument92 SeitenManual Dream StarDanut Dan100% (1)
- Jurnal Keperawatan MuhammadiyahDokument10 SeitenJurnal Keperawatan MuhammadiyahVebryana RamadhaniaNoch keine Bewertungen
- ResMed Autoset Vantage Clinicians ManualDokument272 SeitenResMed Autoset Vantage Clinicians Manualrich_golfNoch keine Bewertungen
- Clinicians To Pediatric Sleep Disorders 2007Dokument370 SeitenClinicians To Pediatric Sleep Disorders 2007Mihaela MuscaluNoch keine Bewertungen
- Case Group 1Dokument10 SeitenCase Group 1JASMEEN RAVALNoch keine Bewertungen
- Obstructive Sleep Apnoea (OSA) Definition of Obstructive Sleep Apnoea (OSA)Dokument4 SeitenObstructive Sleep Apnoea (OSA) Definition of Obstructive Sleep Apnoea (OSA)Abdul JalilNoch keine Bewertungen
- Classification of Sleep DisordersDokument15 SeitenClassification of Sleep Disorderselvinegunawan100% (1)
- FEP Medical Policy Manual: Diagnosis and Medical Management of Obstructive Sleep Apnea SyndromeDokument15 SeitenFEP Medical Policy Manual: Diagnosis and Medical Management of Obstructive Sleep Apnea SyndromeAlfia Pusfitaa SariiNoch keine Bewertungen
- Sleep Apnea and Diabetes RelationshipDokument28 SeitenSleep Apnea and Diabetes RelationshipSumit PuloriaNoch keine Bewertungen
- Resmed Airsense 10 Clinical GuideDokument44 SeitenResmed Airsense 10 Clinical GuideTowtap100% (2)
- Obstructive Sleep ApneaDokument49 SeitenObstructive Sleep ApnearuthNoch keine Bewertungen
- Mode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDateDokument16 SeitenMode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDatedavimemNoch keine Bewertungen
- Portable Devices Used For Home Testing in Obstructive Sleep ApneaDokument42 SeitenPortable Devices Used For Home Testing in Obstructive Sleep ApneaCalifornia Technology Assessment Forum0% (1)
- Yel Cpap Yel Cpap 1587377064Dokument33 SeitenYel Cpap Yel Cpap 1587377064Haitham yousifNoch keine Bewertungen
- Smolensky-Chronobiology and Chronotherapy of Allergic Rhinitis and Bronchial AsthmaDokument31 SeitenSmolensky-Chronobiology and Chronotherapy of Allergic Rhinitis and Bronchial Asthmaeva yustianaNoch keine Bewertungen
- The AASM Manual For The Scoring of Sleep and Associated EventsDokument34 SeitenThe AASM Manual For The Scoring of Sleep and Associated Eventssenseilu8713Noch keine Bewertungen
- Neurological Disorders and Sleep AlterationsDokument20 SeitenNeurological Disorders and Sleep AlterationsGrig GrigNoch keine Bewertungen