Das könnte Ihnen auch gefallen
- Darvocet N Drug CardDokument1 SeiteDarvocet N Drug CardSheri490Noch keine Bewertungen
- Glycerin: (Gli-Ser-In)Dokument2 SeitenGlycerin: (Gli-Ser-In)Aryanto DedyNoch keine Bewertungen
- Drug PrilosecDokument1 SeiteDrug PrilosecSrkocher100% (1)
- Lopressor (Metoprolol) 100mgDokument2 SeitenLopressor (Metoprolol) 100mgAdrianne Bazo100% (2)
- Drug StudyDokument1 SeiteDrug StudyDanian AntonioNoch keine Bewertungen
- Health Teaching (1st-3rd Trimester)Dokument12 SeitenHealth Teaching (1st-3rd Trimester)Jorge Allen DelfinadoNoch keine Bewertungen
- HyoscineDokument4 SeitenHyoscineHana HanaNoch keine Bewertungen
- FiberCon (Polycarbophil)Dokument1 SeiteFiberCon (Polycarbophil)ENoch keine Bewertungen
- Tricyclic antidepressants overviewDokument2 SeitenTricyclic antidepressants overviewAaLona RobinsonNoch keine Bewertungen
- Brand Name: Generic Name: Drug ClassificationDokument2 SeitenBrand Name: Generic Name: Drug ClassificationChristine Pialan SalimbagatNoch keine Bewertungen
- Metoclopramide (Reglan)Dokument1 SeiteMetoclopramide (Reglan)ENoch keine Bewertungen
- Faverin® Fluvoxamine Maleate Film-Coated, Scored Tablets (50 MG and 100 MG)Dokument14 SeitenFaverin® Fluvoxamine Maleate Film-Coated, Scored Tablets (50 MG and 100 MG)Sohaib HassanNoch keine Bewertungen
- Inhalation agents and anesthetic drugsDokument3 SeitenInhalation agents and anesthetic drugsNicole CardenasNoch keine Bewertungen
- (Generic Name) ® Drotaverine 40mgDokument2 Seiten(Generic Name) ® Drotaverine 40mgSangar Sardar100% (1)
- Anes Drugs TableDokument20 SeitenAnes Drugs TableKathleen Grace ManiagoNoch keine Bewertungen
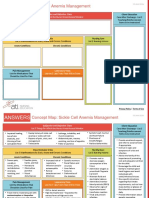
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDokument2 SeitenNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- See Full Prescribing Information For Complete Boxed WarningDokument43 SeitenSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug Studysarah1217Noch keine Bewertungen
- San Beda College College of Nursing drug study guideDokument3 SeitenSan Beda College College of Nursing drug study guideaycee0316Noch keine Bewertungen
- Drug Study Catapres. Losartan, Nootropil Cefuroxime, ArcoxiaDokument2 SeitenDrug Study Catapres. Losartan, Nootropil Cefuroxime, Arcoxiajoy_monterubioNoch keine Bewertungen
- Mental Status: Bates Assessment ToolDokument10 SeitenMental Status: Bates Assessment ToolAngela IlustrisimoNoch keine Bewertungen
- CholestyramineDokument1 SeiteCholestyramineKatie McPeekNoch keine Bewertungen
- Pharmaco TherapeuticsDokument19 SeitenPharmaco TherapeuticsJareena BegumNoch keine Bewertungen
- DrugsDokument20 SeitenDrugsLee Won100% (1)
- IsoprenalineDokument2 SeitenIsoprenalineImmanuel Victor GeorgeNoch keine Bewertungen
- Cardiovascular AgentsDokument22 SeitenCardiovascular AgentsEsther Faith GabrielNoch keine Bewertungen
- Combizar Drug StudyDokument6 SeitenCombizar Drug StudymrnmrsllNoch keine Bewertungen
- PrevacidDokument1 SeitePrevacidAdrianne BazoNoch keine Bewertungen
- PhenobarbitalDokument1 SeitePhenobarbitalJesrel DelotaNoch keine Bewertungen
- LIVOLIN FORTE ACTIONS AND USESDokument5 SeitenLIVOLIN FORTE ACTIONS AND USESDick Morgan FerrerNoch keine Bewertungen
- TumsDokument2 SeitenTumsAdrianne BazoNoch keine Bewertungen
- Drug OmeprazoleDokument1 SeiteDrug OmeprazoleSrkocherNoch keine Bewertungen
- Drug Class:: Prototype (Generic/Trade) : Eskalith, LithobidDokument1 SeiteDrug Class:: Prototype (Generic/Trade) : Eskalith, LithobidAaLona Robinson100% (2)
- PHINMA Nursing Drug StudyDokument2 SeitenPHINMA Nursing Drug StudyArianne NicoleNoch keine Bewertungen
- Drug Name Mechanism of Action Indication/ Contraindication Adverse Effect Nursing ResponsibilitiesDokument1 SeiteDrug Name Mechanism of Action Indication/ Contraindication Adverse Effect Nursing ResponsibilitiesJohnrick VenturaNoch keine Bewertungen
- DiflucanDokument1 SeiteDiflucanSheri490Noch keine Bewertungen
- Albuterol, Accuneb Drug CardDokument2 SeitenAlbuterol, Accuneb Drug Carddnw876Noch keine Bewertungen
- Leoprolide Drug StudyDokument2 SeitenLeoprolide Drug Studyhappymee927Noch keine Bewertungen
- Case Presentation Hypokalemic ManDokument61 SeitenCase Presentation Hypokalemic ManHussain AzharNoch keine Bewertungen
- Famotidine (Pepcid)Dokument1 SeiteFamotidine (Pepcid)Adrianne BazoNoch keine Bewertungen
- Coreg (Carvedilol)Dokument1 SeiteCoreg (Carvedilol)Adrianne BazoNoch keine Bewertungen
- Generic and Trade Names, Mechanisms, InterventionsDokument4 SeitenGeneric and Trade Names, Mechanisms, InterventionsSonia FernandesNoch keine Bewertungen
- Gastrointestinal DrugsDokument45 SeitenGastrointestinal DrugsCindy MaslagNoch keine Bewertungen
- Magnesium Hydroxide (Milk of Magnesia)Dokument1 SeiteMagnesium Hydroxide (Milk of Magnesia)ENoch keine Bewertungen
- Drug Card Motrin 800mgDokument2 SeitenDrug Card Motrin 800mgAdrianne BazoNoch keine Bewertungen
- Drug StudyDokument11 SeitenDrug StudyNedemar OcampoNoch keine Bewertungen
- AtroventDokument1 SeiteAtroventSheri490100% (1)
- Drug Study (Romel Cruz Hospital)Dokument35 SeitenDrug Study (Romel Cruz Hospital)Djoan SamontañezNoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug StudyKwin SaludaresNoch keine Bewertungen
- Drug 25Dokument17 SeitenDrug 25carol_gigliotti24100% (1)
- Drug AdvilDokument1 SeiteDrug AdvilDiana Laura LeiNoch keine Bewertungen
- Drug StudyDokument11 SeitenDrug StudyJay VillasotoNoch keine Bewertungen
- Morphine (Astramorph) PCADokument2 SeitenMorphine (Astramorph) PCAAdrianne Bazo100% (3)
- MorphineDokument1 SeiteMorphineCassie100% (3)
- Percocet Drug CardDokument1 SeitePercocet Drug CardSheri490100% (4)
- NURS 2516 Clinical Medications Worksheets: Nursing Process-AssessmentDokument1 SeiteNURS 2516 Clinical Medications Worksheets: Nursing Process-AssessmentAdrianne BazoNoch keine Bewertungen
- Nalbuphine (Nubain)Dokument2 SeitenNalbuphine (Nubain)Adrianne Bazo100% (1)
- Merperidine (Demerol)Dokument1 SeiteMerperidine (Demerol)ENoch keine Bewertungen
- ValiumDokument2 SeitenValiumAdrianne BazoNoch keine Bewertungen
- Zofran IVPDokument1 SeiteZofran IVPAdrianne Bazo100% (1)
- Zocor (Simvastin)Dokument3 SeitenZocor (Simvastin)Adrianne BazoNoch keine Bewertungen
- Zoloft SertralineDokument1 SeiteZoloft SertralineAdrianne Bazo100% (1)
- ZithromycinDokument1 SeiteZithromycinAdrianne BazoNoch keine Bewertungen
- ToradolDokument2 SeitenToradolAdrianne Bazo100% (1)
- Vitamin DDokument2 SeitenVitamin DAdrianne BazoNoch keine Bewertungen
- Levalbuterol XopenexDokument2 SeitenLevalbuterol XopenexCassie100% (1)
- Vitamin EDokument1 SeiteVitamin EAdrianne BazoNoch keine Bewertungen
- Dulcolax SuppositoryDokument1 SeiteDulcolax SuppositoryAdrianne BazoNoch keine Bewertungen
- TumsDokument2 SeitenTumsAdrianne BazoNoch keine Bewertungen
- Thyroid Preparations (Thyrar)Dokument1 SeiteThyroid Preparations (Thyrar)Adrianne BazoNoch keine Bewertungen
- Tim OpticDokument2 SeitenTim OpticAdrianne BazoNoch keine Bewertungen
- Theragran (Multiple Vitamins)Dokument3 SeitenTheragran (Multiple Vitamins)Adrianne BazoNoch keine Bewertungen
- Tamoxifen NolvadexDokument1 SeiteTamoxifen NolvadexAdrianne Bazo100% (1)
- Temazepam (Restoril)Dokument1 SeiteTemazepam (Restoril)Adrianne BazoNoch keine Bewertungen
- Seroquel (Quetiapine)Dokument1 SeiteSeroquel (Quetiapine)Adrianne BazoNoch keine Bewertungen
- Prinivil (Lisinapril)Dokument2 SeitenPrinivil (Lisinapril)Adrianne BazoNoch keine Bewertungen
- SinacDokument2 SeitenSinacENoch keine Bewertungen
- Quest RanDokument2 SeitenQuest RanAdrianne BazoNoch keine Bewertungen
- Reglan Drug CardDokument4 SeitenReglan Drug CardAdrianne BazoNoch keine Bewertungen
- RisperdalDokument2 SeitenRisperdalAdrianne Bazo100% (1)
- ProtonixDokument1 SeiteProtonixAdrianne BazoNoch keine Bewertungen
- Prozac FluoxetineDokument2 SeitenProzac FluoxetineENoch keine Bewertungen
- Promethazine (Phenergan)Dokument1 SeitePromethazine (Phenergan)Adrianne BazoNoch keine Bewertungen
- Predacot PrednisoneDokument1 SeitePredacot PrednisoneAdrianne BazoNoch keine Bewertungen
- Protonix IVDokument1 SeiteProtonix IVAdrianne BazoNoch keine Bewertungen
- Potassium ChlorideDokument2 SeitenPotassium ChlorideAdrianne BazoNoch keine Bewertungen
- Pepcid IV FamotidineDokument2 SeitenPepcid IV FamotidineAdrianne BazoNoch keine Bewertungen
- Plavix ClopidogrelDokument2 SeitenPlavix ClopidogrelAdrianne Bazo50% (2)
- BRT vs Light Rail Costs: Which is Cheaper to OperateDokument11 SeitenBRT vs Light Rail Costs: Which is Cheaper to Operatejas rovelo50% (2)
- International Waiver Attestation FormDokument1 SeiteInternational Waiver Attestation FormJiabao ZhengNoch keine Bewertungen
- Bhagavad Gita: Chapter 18, Verse 47Dokument3 SeitenBhagavad Gita: Chapter 18, Verse 47pankaj kararNoch keine Bewertungen
- SWSP6033 00 2022T3 V1.0-1Dokument14 SeitenSWSP6033 00 2022T3 V1.0-1ayman.abaidallah1990Noch keine Bewertungen
- Sawmill Safety 3-Trim SawsDokument51 SeitenSawmill Safety 3-Trim SawsramptgdNoch keine Bewertungen
- Flotect Vane Operated Flow Switch: Magnetic Linkage, UL ApprovedDokument1 SeiteFlotect Vane Operated Flow Switch: Magnetic Linkage, UL ApprovedLuis GonzálezNoch keine Bewertungen
- Initial Data Base (Narrative)Dokument11 SeitenInitial Data Base (Narrative)LEBADISOS KATE PRINCESSNoch keine Bewertungen
- I Could Easily FallDokument3 SeitenI Could Easily FallBenji100% (1)
- Global GovernanceDokument20 SeitenGlobal GovernanceSed LenNoch keine Bewertungen
- Minotaur Transformation by LionWarrior (Script)Dokument7 SeitenMinotaur Transformation by LionWarrior (Script)Arnt van HeldenNoch keine Bewertungen
- Essay Sustainable Development GoalsDokument6 SeitenEssay Sustainable Development GoalsBima Dwi Nur Aziz100% (1)
- Lecture1 SEODokument24 SeitenLecture1 SEOUsman AnwarNoch keine Bewertungen
- Isha Hatha Yoga - Program Registration FormDokument2 SeitenIsha Hatha Yoga - Program Registration FormKeyur GadaNoch keine Bewertungen
- What Would Orwell Think?Dokument4 SeitenWhat Would Orwell Think?teapottingsNoch keine Bewertungen
- Hi Tracy: Total Due Here's Your Bill For JanuaryDokument6 SeitenHi Tracy: Total Due Here's Your Bill For JanuaryalexNoch keine Bewertungen
- 15-8377 - 3521 Calandria Communications L. Rivera PDFDokument20 Seiten15-8377 - 3521 Calandria Communications L. Rivera PDFRecordTrac - City of OaklandNoch keine Bewertungen
- Managerial Accounting 12th Edition Warren Test Bank DownloadDokument98 SeitenManagerial Accounting 12th Edition Warren Test Bank DownloadRose Speers100% (21)
- Student Teaching Edtpa Lesson Plan TemplateDokument7 SeitenStudent Teaching Edtpa Lesson Plan Templateapi-3531253350% (1)
- Something About UsDokument18 SeitenSomething About UsFercho CarrascoNoch keine Bewertungen
- 14.marifosque v. People 435 SCRA 332 PDFDokument8 Seiten14.marifosque v. People 435 SCRA 332 PDFaspiringlawyer1234Noch keine Bewertungen
- Hbet1103 Introduction To General LinguisticsDokument11 SeitenHbet1103 Introduction To General LinguisticsNasidah NasahaNoch keine Bewertungen
- Annex-4-JDVP Certificate of Learners MasteryDokument1 SeiteAnnex-4-JDVP Certificate of Learners MasteryZINA ARRDEE ALCANTARANoch keine Bewertungen
- HDFC Bank's Organizational Profile and BackgroundDokument72 SeitenHDFC Bank's Organizational Profile and Backgroundrohitkh28Noch keine Bewertungen
- Ward A. Thompson v. City of Lawrence, Kansas Ron Olin, Chief of Police Jerry Wells, District Attorney Frank Diehl, David Davis, Kevin Harmon, Mike Hall, Ray Urbanek, Jim Miller, Bob Williams, Craig Shanks, John Lewis, Jack Cross, Catherine Kelley, Dan Ward, James Haller, Dave Hubbell and Matilda Woody, Frances S. Wisdom v. City of Lawrence, Kansas Ron Olin, Chief of Police David Davis, Mike Hall, Jim Miller, Bob Williams, Craig Shanks, John L. Lewis, Jack Cross, Kevin Harmon, Catherine Kelley, Dan Ward and James Haller, Jr., 58 F.3d 1511, 10th Cir. (1995)Dokument8 SeitenWard A. Thompson v. City of Lawrence, Kansas Ron Olin, Chief of Police Jerry Wells, District Attorney Frank Diehl, David Davis, Kevin Harmon, Mike Hall, Ray Urbanek, Jim Miller, Bob Williams, Craig Shanks, John Lewis, Jack Cross, Catherine Kelley, Dan Ward, James Haller, Dave Hubbell and Matilda Woody, Frances S. Wisdom v. City of Lawrence, Kansas Ron Olin, Chief of Police David Davis, Mike Hall, Jim Miller, Bob Williams, Craig Shanks, John L. Lewis, Jack Cross, Kevin Harmon, Catherine Kelley, Dan Ward and James Haller, Jr., 58 F.3d 1511, 10th Cir. (1995)Scribd Government DocsNoch keine Bewertungen
- Revised Answer Keys for Scientist/Engineer Recruitment ExamDokument5 SeitenRevised Answer Keys for Scientist/Engineer Recruitment ExamDigantNoch keine Bewertungen
- Buckling of Thin Metal Shells 58Dokument1 SeiteBuckling of Thin Metal Shells 58pawkomNoch keine Bewertungen
- Course Title: Cost Accounting Course Code:441 BBA Program Lecture-3Dokument20 SeitenCourse Title: Cost Accounting Course Code:441 BBA Program Lecture-3Tanvir Ahmed ChowdhuryNoch keine Bewertungen
- 2006 - Bykovskii - JPP22 (6) Continuous Spin DetonationsDokument13 Seiten2006 - Bykovskii - JPP22 (6) Continuous Spin DetonationsLiwei zhangNoch keine Bewertungen
- ControllingDokument8 SeitenControllingAnjo Pasiolco Canicosa100% (2)
- American Buffalo - DAVID MAMETDokument100 SeitenAmerican Buffalo - DAVID MAMETRodrigo Garcia Sanchez100% (10)