Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Pig Digestive System-Digestive System of The PigDokument4 SeitenPig Digestive System-Digestive System of The PiglsvcsbNoch keine Bewertungen
- Sugar Cane JuiceDokument5 SeitenSugar Cane Juices.sabapathyNoch keine Bewertungen
- Bodyweight Training PDFDokument10 SeitenBodyweight Training PDFudien20060% (1)
- Analytical and Hortatory ExpositionDokument3 SeitenAnalytical and Hortatory ExpositionChie TjeeNoch keine Bewertungen
- A Pilot Case Study On The Impact of A Self-Prescribed Ketogenic Diet On Biochemical Parameters and Running Performance in Healthy and Physically Active IndividualsDokument27 SeitenA Pilot Case Study On The Impact of A Self-Prescribed Ketogenic Diet On Biochemical Parameters and Running Performance in Healthy and Physically Active Individualsblaz86Noch keine Bewertungen
- Carpal Tunnel Syndrome - Wikipedia PDFDokument107 SeitenCarpal Tunnel Syndrome - Wikipedia PDFMuhammadNoch keine Bewertungen
- Mushroom Attitude and Usuage Study 6-23-11Dokument111 SeitenMushroom Attitude and Usuage Study 6-23-11Eric J. BrucknerNoch keine Bewertungen
- TreadliftDokument39 SeitenTreadliftAhong Ben Saleyella100% (5)
- Saettigung Lebensmittel Satiety IndexDokument13 SeitenSaettigung Lebensmittel Satiety IndexVera SimilarNoch keine Bewertungen
- Diet and Osteoarthritis: Cholesterol ReductionDokument2 SeitenDiet and Osteoarthritis: Cholesterol ReductionbagasNoch keine Bewertungen
- Genpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)Dokument67 SeitenGenpath 04 - RENAL LABORATORY TESTS - ppt.MEd 2016 (Ninaarajade's Conflicted Copy 2016-10-29) (ASUS's Conflicted Copy 2016-11-14)RjDNoch keine Bewertungen
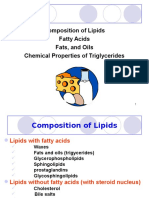
- Lipids: Composition of Lipids Fatty Acids Fats, and Oils Chemical Properties of TriglyceridesDokument29 SeitenLipids: Composition of Lipids Fatty Acids Fats, and Oils Chemical Properties of TriglyceridesRichelyn Lanes CaburogNoch keine Bewertungen
- Fad Diets PowerPointDokument54 SeitenFad Diets PowerPointandrea6024100% (1)
- The of By: Detection Lactose and Maltose Means of MethylamineDokument3 SeitenThe of By: Detection Lactose and Maltose Means of MethylamineŠĭlệncěIšmyPŕIdệNoch keine Bewertungen
- Spirulina Improves Growth - Egg Production and Meat Quality - 2012Dokument15 SeitenSpirulina Improves Growth - Egg Production and Meat Quality - 2012julesverneNoch keine Bewertungen
- Exercises With Different TensesDokument3 SeitenExercises With Different TensesrodicabudesNoch keine Bewertungen
- Narce, Almera Rose F. Pharmacology BSN-2A Instructor: Ms. Kenvyne Quides-Calugay, RN, Man Drug Study 2 FinalsDokument1 SeiteNarce, Almera Rose F. Pharmacology BSN-2A Instructor: Ms. Kenvyne Quides-Calugay, RN, Man Drug Study 2 FinalsAlmera Rose NarceNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug StudyKaloy KamaoNoch keine Bewertungen
- Soto 9780307594884 1p All r1Dokument336 SeitenSoto 9780307594884 1p All r1wamu8850Noch keine Bewertungen
- Meena Photo EssayDokument17 SeitenMeena Photo Essayapi-533348723Noch keine Bewertungen
- Biology 2a03 - Lab 1 Outline 2012Dokument28 SeitenBiology 2a03 - Lab 1 Outline 2012Ata AnsariNoch keine Bewertungen
- Si MPletesDokument1.139 SeitenSi MPletesRitaLiangNoch keine Bewertungen
- Project Sta 108 1Dokument13 SeitenProject Sta 108 1Hazwan HamimNoch keine Bewertungen
- Unit 5 Nutritional Consideration in The Prevention and Management of Cardiovascular Diseases, Educational PlatformDokument18 SeitenUnit 5 Nutritional Consideration in The Prevention and Management of Cardiovascular Diseases, Educational Platformzia ullah100% (1)
- Muscle & Fitness USA - June 2016Dokument208 SeitenMuscle & Fitness USA - June 2016mario198501100% (2)
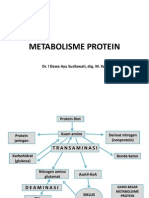
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDokument31 SeitenMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- XXXXDokument8 SeitenXXXXalcelNoch keine Bewertungen
- Oliver Et Al., 2009 Glucose Sensors-A ReviewDokument14 SeitenOliver Et Al., 2009 Glucose Sensors-A ReviewMoisi XhoxhiNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaIndri NizaNoch keine Bewertungen
- The Damage of Food PDFDokument2 SeitenThe Damage of Food PDFYvonne CarlileNoch keine Bewertungen