Sysmex Educational Enhancement & Development
SEED-Africa Newsletter | No 3 | February 2011
The Prothrombin Time Test The purpose of this newsletter is to provide laboratory staff with an overview of the prothrombin time test, the concept of the INR and oral anticoagulation.
The need for anticoagulation
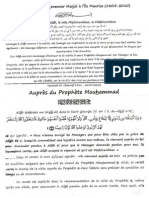
n If the carboxyl groups are not added, the clotting factors as well as PC and PS are non-functional. As was discussed in the first newsletter, the fundamental principle of haemostasis is to minimise blood loss at sites of n In the coagulation process, clotting factors need to vessel injury whilst maintaining blood flow at all times. This be bound to phospholipid (the surface of activated is maintained via a highly regulated fine-tuned interaction platelets), a process that can only take place in the of multiple biological processes. When this balance is presence of carboxyl groups on the clotting factors and disturbed in favour of excessive clot formation, patients using are at risk of developing pathological thrombosis which Fig-1 - Proof 1 calcium ions as a ligand. will interfere with blood circulation and may be fatal. Such patients are commonly treated with anticoagulant drugs which aim to restore the haemostatic balance and therefore Clotting factors II, VII, IX, X PRECURSOR FORMS Glutamic Acid minimise the risk of thrombosis. Examples of disorders for which oral anticoagulants are commonly prescribed are reduced venous thromboembolism (deep vein thrombosis/pulmonary Vit K embolism), atrial fibrillation, coronary heart disease and
ischaemic stroke.
Warfarin
The most commonly prescribed anticoagulant for long term use is warfarin. The mechanism of action of warfarin is as follows: n Warfarin inhibits the enzyme vitamin K epoxide reductase
n
Vit K Epoxide Reductase WARFARIN Vit K Epoxide
Carboxylase
FUNCTIONAL FACTORS GLA
COO-+Ca+Platelet Phospholipid
This results in an inability to convert vitamin K epoxide back into reduced vitamin K.
Figure 1. The mechanism of action of warfarin
Reduced vitamin K is required as a co-factor for the enzyme gamma carboxylase. Gamma carboxylase is an enzyme that adds carboxyl groups to the glutamic acid residues on the precursor clotting factors II, VII, IX and X as well as protein C and protein S, all of which are produced in the liver.
SEED-Africa Newsletter | No 3 | February 2011 Sysmex Educational Enhancement & Development
2/3
The great advantage of warfarin is that it is an oral drug. The disadvantage however is that there is substantial variability in its biological effect from person to person and also in a single individual over time. There are multiple factors that contribute to this including genetics, diet and concomitant drug use. As the benefits of warfarin are restricted to a narrow therapeutic window, laboratory monitoring is mandatory in order to minimise the risk of haemorrhagic complications or ongoing hypercoagulabilty.
The manual PT method a) Requirements
n
Waterbath at 37C Thermometer Pipettes 100 l & 200 l Pipette tips Stop watch x 2 Glass test tubes - 5 ml Thromboplastin reagent (e.g. Innovin Siemens) Spun down patient plasma Normal patient plasma n Pooled normal plasma or n Citrol Level 1 (non-assayed or assayed) Control plasma Citrol Level 1 assayed Scientific calculator
The prothrombin time (PT)
The PT is a baseline screening test for patients with suspected bleeding abnormalities and is extensively used for monitoring oral anticoagulant therapy (warfarin and other coumadin drugs). It is not useful for investigating possible causes of clotting in a patient. It is used to assess for defects in the extrinsic and common pathways. A prolonged clotting time could be due to reduced or absent activity of one or more of factors VII, FX, FV, FII and fibrinogen. The reduced activity could be due to a quantitative deficiency or reduced function of a clotting factor due to the vitamin K absence or inhibition (warfarin) or due to an inhibitor directed against the clotting factor.
n
EXTRINSIC
INTRINSIC FXII
b) Innovin
n
Thromboplastin reagent containing tissue factor, phospholipid (platelet substitute) and calcium chloride Lyophilised long expiry times ~ 2-3 years
[PT]
[PTT] FXI
n n Very
TF/FVII FX COMMON
II (Prothrombin)
FIX (FVIII) (FV)
Needs to be reconstituted with preservative free distilled water Must warm up to 37C before use. Stability after reconstitution 10 days 2-8C if kept stoppered n 5 days 15-25C if kept stoppered n 24 hours at 37C if kept stoppered (in waterbath)
n
Fibrinogen
n
Refer to the package insert for comprehensive handling instructions
Figure 2. Clotting pathway tested by the prothrombin time
The thromboplastin reagent used to start the clotting reaction in the PT test is in fact the equivalent of tissue factor (TF).
SEED-Africa Newsletter | No 3 | February 2011 Sysmex Educational Enhancement & Development
3/3
c) Manual Method
n
The PT is converted to an INR using the following formula: INR = (Patient PT / MNPT)ISI MNPT mean normal PT time (obtained from a pool of 20+ normal plasmas or alternately from a commercial normal control such as Citrol Level 1). For manual testing, each technologist must determine his/her own MNPT time. A scientific calculator is required to calculate the final INR value. The INR should only be used for patients on anticoagulant therapy. Interpretation of INR: INR 2-3 - therapeutic INR <2 underdosed, at risk of clotting INR >3 overdosed, at risk of bleeding For non anticoagulated patients, the PT numerical value in seconds should be used in conjunction with normal reference ranges for interpretation. The normal reference range should be established locally by each laboratory but on average will be ~10-13 seconds. A prolonged value suggests a defect in the extrinsic and/ or common pathway. A low value usually has no clinical significance but should be reviewed case by case. The next edition will focus on the activated partial thromboplastin time and the mechanism of action of heparin.
Check that temperature of water in waterbath is at 37C. Warm up reagent (Innovin) to 37C (dispense quantity required for number of planned tests into test tube, place test tube in rack submerged in waterbath). Add 100 l of patient plasma to glass test tube in waterbath. Add 200 l of Innovin to patient test tube and start stop watch immediately. Immediately mix well and start looking for fibrin strands. Keep swirling tube back into the water to ensure that the temperature of the reaction remains at 37C. Gently tilt tube when lifting it out the water and check for clot continuously. As soon as fibrin strands are observed, stop the stopwatch and record the time. Ideally the test should be done in duplicate and the average of the two times recorded. Repeat with normal control plasma. It is best to use pooled normal plasma to obtain the mean normal PT time, but if this is not available then use a commercial normal control that is compatible with the thromboplastin reagent eg. Citrol Level 1.
Prothrombin time and INR
PT results are commonly reported as an international normalised ratio (INR). The World Health Organisation introduced the concept of the INR in order to standardise reporting of PT results for patients on warfarin (or equivalent coumadin derivatives) oral anticoagulant therapy. Different thromboplastin reagents have different sensitivities, i.e. will result in slightly different clotting times on the same plasma samples. As the degree of prolongation of the PT is used to assess whether the patient is adequately anticoagulated, the results in seconds and hence the interpretation will be influenced by the reagent used. In order to compensate for these differences reagents are assigned an international sensitivity index or ISI value. The ideal reagent would have an ISI value of 1. It is always advisable to use a reagent with an ISI value as close to one as possible.
Sysmex South Africa (Pty) Ltd.
Fernridge Office Park Block 2, 5 Hunter Avenue, Ferndale, Randburg 2194 Phone +27 11 329 9480 Fax +27 11 789 9276 info@sysmex.co.za www.sysmex.co.za
Das könnte Ihnen auch gefallen
- 3 - Toronto Notes 2011 - Anesthesia - and - Peri-Operative - MedicineDokument28 Seiten3 - Toronto Notes 2011 - Anesthesia - and - Peri-Operative - MedicineHisham Qassrawi100% (1)
- The Diagnostic Challenge of Joint Pain - Part2 PDFDokument5 SeitenThe Diagnostic Challenge of Joint Pain - Part2 PDFM Yusuf Ali RNoch keine Bewertungen
- The Diagnostic Challenge of Joint Pain - Part1 PDFDokument5 SeitenThe Diagnostic Challenge of Joint Pain - Part1 PDFM Yusuf Ali RNoch keine Bewertungen
- Eye Can See A Nest of Worms!Dokument1 SeiteEye Can See A Nest of Worms!M Yusuf Ali RNoch keine Bewertungen
- Modele de ParentsDokument4 SeitenModele de ParentsM Yusuf Ali RNoch keine Bewertungen
- The Essential Guide To Brain TumoursDokument43 SeitenThe Essential Guide To Brain TumoursM Yusuf Ali RNoch keine Bewertungen
- SEED No 1 - COAG - Principles of HaemostasisDokument4 SeitenSEED No 1 - COAG - Principles of HaemostasisM Yusuf Ali RNoch keine Bewertungen
- Homozygous Familial HypercholesterolaemiaDokument1 SeiteHomozygous Familial HypercholesterolaemiaM Yusuf Ali RNoch keine Bewertungen
- SEED No 2 - Pre Analytical Factors That Influence Coagulation Test ResultsDokument4 SeitenSEED No 2 - Pre Analytical Factors That Influence Coagulation Test ResultsM Yusuf Ali RNoch keine Bewertungen
- Noor E Muhammad Masjid DocumentsDokument1 SeiteNoor E Muhammad Masjid DocumentsM Yusuf Ali RNoch keine Bewertungen
- Aupres Du Prophete Mouhammad SAWDokument4 SeitenAupres Du Prophete Mouhammad SAWM Yusuf Ali RNoch keine Bewertungen
- Tic Choroidal MelanomaDokument1 SeiteTic Choroidal MelanomaM Yusuf Ali RNoch keine Bewertungen
- Retro Peritoneal Liposarcoma With Lamellar Bone InsideDokument1 SeiteRetro Peritoneal Liposarcoma With Lamellar Bone InsideM Yusuf Ali RNoch keine Bewertungen
- Nearly An Eye-CatcherDokument1 SeiteNearly An Eye-CatcherM Yusuf Ali RNoch keine Bewertungen
- DilatedcardiomyopathyDokument11 SeitenDilatedcardiomyopathyM Yusuf Ali RNoch keine Bewertungen
- Sturge-Weber AngiomatosisDokument1 SeiteSturge-Weber AngiomatosisM Yusuf Ali RNoch keine Bewertungen
- Placental Vasa PreviaDokument1 SeitePlacental Vasa PreviaM Yusuf Ali RNoch keine Bewertungen
- Acute Liver FailureDokument12 SeitenAcute Liver FailureM Yusuf Ali RNoch keine Bewertungen
- Bilateral Spontaneous Anterior Dislocation of Crystalline LensDokument1 SeiteBilateral Spontaneous Anterior Dislocation of Crystalline LensM Yusuf Ali RNoch keine Bewertungen
- A Painful Cranial BulgeDokument1 SeiteA Painful Cranial BulgeM Yusuf Ali RNoch keine Bewertungen
- Corkscrew Oesophagus On Virtual EndosDokument1 SeiteCorkscrew Oesophagus On Virtual EndosM Yusuf Ali RNoch keine Bewertungen
- Valsalva Haemorrhagic Thy After Push-UpsDokument1 SeiteValsalva Haemorrhagic Thy After Push-UpsM Yusuf Ali RNoch keine Bewertungen
- AlcoholDokument10 SeitenAlcoholJean Paul GottretNoch keine Bewertungen
- ALHIDAYA162Dokument2 SeitenALHIDAYA162M Yusuf Ali RNoch keine Bewertungen
- Tuberculosis Sem LancetDokument16 SeitenTuberculosis Sem LancetM Yusuf Ali RNoch keine Bewertungen
- Al Hidaya 161Dokument2 SeitenAl Hidaya 161M Yusuf Ali RNoch keine Bewertungen
- JAMA 2011 Chang 767 8.... Skin ChangesDokument2 SeitenJAMA 2011 Chang 767 8.... Skin ChangesM Yusuf Ali RNoch keine Bewertungen
- Unexpected Life Lessons From Cardiac Anatomy and PhysiologyDokument2 SeitenUnexpected Life Lessons From Cardiac Anatomy and PhysiologyM Yusuf Ali RNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Rayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanDokument17 SeitenRayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanValentine Brokenz Saintz100% (1)
- Enabiz TahlilleriDokument4 SeitenEnabiz TahlilleriMansoor AyoubiNoch keine Bewertungen
- Abim Lab ValuesDokument4 SeitenAbim Lab ValuesBell GatesNoch keine Bewertungen
- Phlebotomy Study SheetsDokument50 SeitenPhlebotomy Study SheetsJona Aure100% (4)
- Iron Deficiency Anemia in PregnancyDokument10 SeitenIron Deficiency Anemia in PregnancySuci Amalia RendreanaNoch keine Bewertungen
- Immune Thrombocytopenic PurpuraDokument10 SeitenImmune Thrombocytopenic PurpuraRishav AgrawalNoch keine Bewertungen
- Applied Immunology Practical 2 Um BiomedDokument16 SeitenApplied Immunology Practical 2 Um Biomedkiedd_04100% (1)
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDokument15 SeitenApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNoch keine Bewertungen
- Dr. Charles Drew: Father of the Blood BankDokument5 SeitenDr. Charles Drew: Father of the Blood BankPopin554Noch keine Bewertungen
- Hemoglobin and Iron Metabolism: Transport of Respiratory GasesDokument6 SeitenHemoglobin and Iron Metabolism: Transport of Respiratory GasesAnusuya SNoch keine Bewertungen
- Blood Groups: HAP Unit 5thDokument31 SeitenBlood Groups: HAP Unit 5thSNEHASIS POLLEYNoch keine Bewertungen
- 1.blood GroupDokument38 Seiten1.blood GroupteraraNoch keine Bewertungen
- Hemolytic Disease of The NewbornDokument43 SeitenHemolytic Disease of The Newbornalibayaty1Noch keine Bewertungen
- Haemolysis As Influence & Interference FactorDokument4 SeitenHaemolysis As Influence & Interference FactormohammedNoch keine Bewertungen
- Blood GroupDokument12 SeitenBlood Groupalive computerNoch keine Bewertungen
- Pancytopenia and BicytopeniaDokument12 SeitenPancytopenia and BicytopeniaRonny DoankNoch keine Bewertungen
- Blood GroupDokument1 SeiteBlood GroupgpsriramNoch keine Bewertungen
- BT 633-Human Biology & Diseases: Blood Patho-PhysiologyDokument11 SeitenBT 633-Human Biology & Diseases: Blood Patho-PhysiologySriMounicaKalidasuNoch keine Bewertungen
- Blood & Blood ProductsDokument126 SeitenBlood & Blood ProductsdrprasadingleyNoch keine Bewertungen
- Importance of Blood DonationDokument9 SeitenImportance of Blood DonationJoseph KooNoch keine Bewertungen
- Haemonetics Cell Saver CS5Dokument8 SeitenHaemonetics Cell Saver CS5zairmendesNoch keine Bewertungen
- Bloodfilm Preparationandreporting 200512223320Dokument203 SeitenBloodfilm Preparationandreporting 200512223320Alex StefanNoch keine Bewertungen
- Blood Group Testing: Hong-Yang Li and Kai GuoDokument11 SeitenBlood Group Testing: Hong-Yang Li and Kai Guodkp rbmNoch keine Bewertungen
- The Role of The Elution in Antibody InvestigationsDokument5 SeitenThe Role of The Elution in Antibody InvestigationskumaraNoch keine Bewertungen
- Anemia of Chronic Disease: Causes, Symptoms, TreatmentDokument13 SeitenAnemia of Chronic Disease: Causes, Symptoms, Treatmentmaverick mazeNoch keine Bewertungen
- Blood Transfusion Protocols in NeonatesDokument12 SeitenBlood Transfusion Protocols in NeonatesSupriya M A SuppiNoch keine Bewertungen
- Ra 7719 Blood Bank MT-B & C 8Dokument7 SeitenRa 7719 Blood Bank MT-B & C 8Fait Hee100% (1)
- Knowledge, Attitude and Practice Regarding Blood Donation in Medical Undergraduates: A Cross Sectional StudyDokument5 SeitenKnowledge, Attitude and Practice Regarding Blood Donation in Medical Undergraduates: A Cross Sectional StudydeebahashNoch keine Bewertungen
- Red Blood Cell Morphology GuideDokument33 SeitenRed Blood Cell Morphology GuideInahkoni Alpheus Sky OiragasNoch keine Bewertungen
- ABO Forward and Reverse TestingDokument4 SeitenABO Forward and Reverse Testing''Rochelle Mylene ﭢ Ygoña100% (1)