Das könnte Ihnen auch gefallen
- Paket MCU - Kontraktor Pertamina Hulu Mahakam 2020Dokument1 SeitePaket MCU - Kontraktor Pertamina Hulu Mahakam 2020rio HENRYNoch keine Bewertungen
- Tugas Sesi 5 (KP - Anselius Sibagariang)Dokument1 SeiteTugas Sesi 5 (KP - Anselius Sibagariang)Anselius SibagariangNoch keine Bewertungen
- DHSS AA - Tables 2010 UpdatesDokument49 SeitenDHSS AA - Tables 2010 Updatesyudelky81Noch keine Bewertungen
- PROGNOSISDokument2 SeitenPROGNOSISapi-19762967Noch keine Bewertungen
- Prognosis and EvaluationDokument2 SeitenPrognosis and Evaluationapi-19762967Noch keine Bewertungen
- Health Screening Package 2020-2021Dokument2 SeitenHealth Screening Package 2020-2021Stampede VincentNoch keine Bewertungen
- DTG - TLD Presentation For National Roll Out Training - NigeriaDokument45 SeitenDTG - TLD Presentation For National Roll Out Training - NigeriaOlayinka AwofoduNoch keine Bewertungen
- Respiratory Case 3: (Increased) (Increased) (Increased)Dokument2 SeitenRespiratory Case 3: (Increased) (Increased) (Increased)Darpan GelalNoch keine Bewertungen
- Target Population - Health Assessment Matrix - 2021 - 220628 - 092416Dokument1 SeiteTarget Population - Health Assessment Matrix - 2021 - 220628 - 092416Reza ApriansyahNoch keine Bewertungen
- ( Û ) Questionnaire Hospital InformationDokument5 Seiten( Û ) Questionnaire Hospital InformationsjeloNoch keine Bewertungen
- Daftar Inventaris Bahan Berbahaya Dan Beracun Di Lingkungan Rsud CengkarengDokument4 SeitenDaftar Inventaris Bahan Berbahaya Dan Beracun Di Lingkungan Rsud Cengkarengyusuf BakhtiarNoch keine Bewertungen
- Alat Gawat DaruratDokument4 SeitenAlat Gawat Daruratjaja nugrahaNoch keine Bewertungen
- Daftar Peralatan Elektromedik Menurut Ecri Dan WhoDokument4 SeitenDaftar Peralatan Elektromedik Menurut Ecri Dan WhoAulia ArthaNoch keine Bewertungen
- Inclusion Criteria DS-TB Exclusion Criteria DS-TBDokument5 SeitenInclusion Criteria DS-TB Exclusion Criteria DS-TBRannissa PuspitaNoch keine Bewertungen
- MX SummaryDokument4 SeitenMX SummaryPratzNoch keine Bewertungen
- PMM Anchor Winches Daily ChecklistDokument20 SeitenPMM Anchor Winches Daily Checklistyudi jdxNoch keine Bewertungen
- Super Nis Summary 2017-18Dokument1 SeiteSuper Nis Summary 2017-18api-286560136Noch keine Bewertungen
- 體格檢查計劃Dokument2 Seiten體格檢查計劃cindy linNoch keine Bewertungen
- Jadwal Pemeliharaan Dan Perawatan Preventif - PT Abacus Cash Solution Makassar - Periode 2023Dokument10 SeitenJadwal Pemeliharaan Dan Perawatan Preventif - PT Abacus Cash Solution Makassar - Periode 2023satria SuryantoroNoch keine Bewertungen
- Lembar Checklist Instrument: Bulan: MaretDokument2 SeitenLembar Checklist Instrument: Bulan: Maretdisca pravitraNoch keine Bewertungen
- Facility Health, Safety and Environmental Management (Hse)Dokument2 SeitenFacility Health, Safety and Environmental Management (Hse)Syahirah NazriNoch keine Bewertungen
- Facility Health, Safety and Environmental Management (Hse)Dokument2 SeitenFacility Health, Safety and Environmental Management (Hse)Syahirah NazriNoch keine Bewertungen
- Facility Health, Safety and Environmental Management (Hse)Dokument2 SeitenFacility Health, Safety and Environmental Management (Hse)Syahirah NazriNoch keine Bewertungen
- Alkes R MawarDokument4 SeitenAlkes R MawarImam Mulyo SantosoNoch keine Bewertungen
- Certificate of Health: SurnameDokument2 SeitenCertificate of Health: SurnameNK productionNoch keine Bewertungen
- Medical TestDokument1 SeiteMedical TestSarat KumarNoch keine Bewertungen
- Abnormal Vaginal Bleeding Algorithm 050809Dokument1 SeiteAbnormal Vaginal Bleeding Algorithm 050809ffaaNoch keine Bewertungen
- American College of Radiology ACR Appropriateness CriteriaDokument7 SeitenAmerican College of Radiology ACR Appropriateness CriteriaMeutia PutriNoch keine Bewertungen
- Management of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsDokument8 SeitenManagement of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsAqilah SyafiqahNoch keine Bewertungen
- CA Treatment Osteosarcoma Pedi Web AlgorithmDokument6 SeitenCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNoch keine Bewertungen
- ObGyn Concise Notes NEET-PGDokument57 SeitenObGyn Concise Notes NEET-PGMohamed TayyabNoch keine Bewertungen
- Blood Pressure Medication InitiationDokument1 SeiteBlood Pressure Medication InitiationMurray DrydenNoch keine Bewertungen
- CP HivDokument2 SeitenCP Hivmelania sea kedangNoch keine Bewertungen
- TB Treatment RegimenDokument2 SeitenTB Treatment RegimenTshiamo TekeNoch keine Bewertungen
- Poster of SeptilinDokument1 SeitePoster of SeptilinNishtha KumarNoch keine Bewertungen
- Stroke Physician: Clinical Decision FormDokument6 SeitenStroke Physician: Clinical Decision FormBaiq PritaNoch keine Bewertungen
- Check List Kelengkapan Berkas Perjanjian Kerja Sama PBFDokument2 SeitenCheck List Kelengkapan Berkas Perjanjian Kerja Sama PBFRaditAnoguEngkolNoch keine Bewertungen
- Actual SoapiesDokument8 SeitenActual SoapiesBeverlyn AsparoNoch keine Bewertungen
- Data Peralatan Rs Tipe CDokument46 SeitenData Peralatan Rs Tipe CrusmilawatiNoch keine Bewertungen
- Table 1: Intial Evaluation On Arrival To ER For All PatientsDokument1 SeiteTable 1: Intial Evaluation On Arrival To ER For All PatientsHetoshima KeiNoch keine Bewertungen
- Carcinoma de OvarioDokument7 SeitenCarcinoma de OvarioNicolás BertachiniNoch keine Bewertungen
- No. Resp Tidak Ber PhbsDokument2 SeitenNo. Resp Tidak Ber Phbsnunik widiasutiNoch keine Bewertungen
- Alkes VKDokument430 SeitenAlkes VKImam Mulyo SantosoNoch keine Bewertungen
- EsmoMetastatic Colorectal CancerDokument41 SeitenEsmoMetastatic Colorectal CancerrafatrujNoch keine Bewertungen
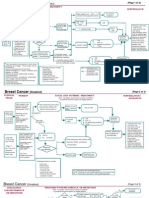
- Breast InvasiveDokument3 SeitenBreast InvasiveAneeshNoch keine Bewertungen
- 1.5 MG/DL 156.6 MG/DL 3.60 MG/DL 133 G/L 0.40Dokument4 Seiten1.5 MG/DL 156.6 MG/DL 3.60 MG/DL 133 G/L 0.40Rachelle Anne LetranNoch keine Bewertungen
- DM CHFDokument2 SeitenDM CHFSafa Abdualrahaman Ali HamadNoch keine Bewertungen
- History FormDokument5 SeitenHistory FormYazeed AsrawiNoch keine Bewertungen
- Abdominal PDFDokument1 SeiteAbdominal PDFChakra BaktiNoch keine Bewertungen
- Perioperative Anticoagulation Bridging Guideline PostedDokument6 SeitenPerioperative Anticoagulation Bridging Guideline PostedNuc Alexandru100% (1)
- Daftar Alat Kesehatan PMK Nomor 56 Tahun 2014Dokument35 SeitenDaftar Alat Kesehatan PMK Nomor 56 Tahun 2014RaniNoch keine Bewertungen
- Anae15291 Sup 0001 Appendixs1Dokument10 SeitenAnae15291 Sup 0001 Appendixs1iamseraNoch keine Bewertungen
- Summary Gynecology - 1Dokument29 SeitenSummary Gynecology - 1Mohamad MostafaNoch keine Bewertungen
- Trial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Dokument4 SeitenTrial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Natalia QuinteroNoch keine Bewertungen
- LRP VGFDPI 2021 004 - ProtocolDokument25 SeitenLRP VGFDPI 2021 004 - ProtocolDileep CRCNoch keine Bewertungen
- ASTRO23Slides VanasDokument18 SeitenASTRO23Slides Vanasjohapatino46Noch keine Bewertungen
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDokument62 SeitenDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNoch keine Bewertungen
- PTS LuxuryDokument1 SeitePTS Luxuryshane.ramirez1980Noch keine Bewertungen
- ACLS ACS Algorithm NewDokument3 SeitenACLS ACS Algorithm Newsambo100% (1)
- Screening of C-Dna Library Using Colony PCRDokument7 SeitenScreening of C-Dna Library Using Colony PCRIJAR JOURNALNoch keine Bewertungen
- Bone Morphogenetic ProteinDokument26 SeitenBone Morphogenetic ProteinvictormoirangthemNoch keine Bewertungen
- Acute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODokument29 SeitenAcute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODOCTOR DanishNoch keine Bewertungen
- Advantages and Disadvantages of Asexual ReproductionDokument12 SeitenAdvantages and Disadvantages of Asexual ReproductionPew Collado PlaresNoch keine Bewertungen
- Mark Scheme (Results) : Pearson EdexcelDokument20 SeitenMark Scheme (Results) : Pearson EdexcelA.S_IN_75Noch keine Bewertungen
- Mutagenesis: Site-Specific: September 2005Dokument13 SeitenMutagenesis: Site-Specific: September 2005Sarnam SinghNoch keine Bewertungen
- 2016 Bacteriology Medical Review HandoutDokument187 Seiten2016 Bacteriology Medical Review HandoutAndrassy Twinkle AlineaNoch keine Bewertungen
- Lab Report #5Dokument9 SeitenLab Report #5yejiNoch keine Bewertungen
- Acute Erythroid Leukemia: Review ArticleDokument10 SeitenAcute Erythroid Leukemia: Review Articlemita potabugaNoch keine Bewertungen
- Duo Dengue Ag-Igg/Igm Rapid Test: OnsiteDokument2 SeitenDuo Dengue Ag-Igg/Igm Rapid Test: OnsiteCristian LaraNoch keine Bewertungen
- Introduction To ImmunoassaysDokument44 SeitenIntroduction To Immunoassaysvidhi100% (1)
- Free Vaccine GuideDokument21 SeitenFree Vaccine Guidesurveytryer2Noch keine Bewertungen
- W-13 ImmunityDokument12 SeitenW-13 ImmunityZelle Da ReyesNoch keine Bewertungen
- Pediatric RhabdomyosarcomaDokument24 SeitenPediatric RhabdomyosarcomaMikael AngelooNoch keine Bewertungen
- A 1 Micro Globulin AdDokument24 SeitenA 1 Micro Globulin AdCARLOSNoch keine Bewertungen
- ELSC 111 2nd Quarter ExamDokument5 SeitenELSC 111 2nd Quarter ExamEdelito BernalNoch keine Bewertungen
- PlasmidDokument8 SeitenPlasmidMido AchiriNoch keine Bewertungen
- Cts-Mdcat 4th Online TestDokument36 SeitenCts-Mdcat 4th Online Testjaipal singhNoch keine Bewertungen
- Erythrocytes Red Blood CellsDokument54 SeitenErythrocytes Red Blood Cellsclarence fernandezNoch keine Bewertungen
- Covid 19Dokument42 SeitenCovid 19ok100% (3)
- Intro To MycologyDokument8 SeitenIntro To Mycologycamille chuaNoch keine Bewertungen
- Sterilization and Aseptic TechniqueDokument3 SeitenSterilization and Aseptic TechniqueE.coilman100% (3)
- Mystery OrganismDokument5 SeitenMystery OrganismJilian McGuganNoch keine Bewertungen
- Analysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)Dokument11 SeitenAnalysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)jeffreyNoch keine Bewertungen
- MCQ of Davidson's Principles and Practice of Medicine: 22 EditionDokument232 SeitenMCQ of Davidson's Principles and Practice of Medicine: 22 EditionAateka100% (1)
- MIKOLOGIDokument27 SeitenMIKOLOGIaxo styleNoch keine Bewertungen
- Family Planing and Sexually Transmitted DiseasesDokument34 SeitenFamily Planing and Sexually Transmitted DiseasesRina KawamuraNoch keine Bewertungen
- Ebola ActivityDokument7 SeitenEbola Activitycory kurdapyaNoch keine Bewertungen
- BACTERIOPHAGEDokument21 SeitenBACTERIOPHAGERobin Oben100% (1)
- 724011.knjiga Respiratory Infections Upper RTInfections Chapter 2 2013Dokument13 Seiten724011.knjiga Respiratory Infections Upper RTInfections Chapter 2 2013Christabella Natalia WijayaNoch keine Bewertungen