Das könnte Ihnen auch gefallen
- Pain SecretsDokument790 SeitenPain SecretsAaron Jones100% (7)
- Pain ManagementDokument60 SeitenPain ManagementRabin KC100% (4)
- 125 QUESTIONS BANK TITLEDokument12 Seiten125 QUESTIONS BANK TITLEnana80% (5)
- Pain ManagementDokument175 SeitenPain ManagementBobby Noel Cerro Jr100% (4)
- From Acute To Chronic Back PainDokument607 SeitenFrom Acute To Chronic Back PainHugo Falqueto100% (2)
- Chronic Pain Management ChartsDokument2 SeitenChronic Pain Management Chartslrpokhrel100% (3)
- PainDokument230 SeitenPainAnonymous uGbcVSJTDg100% (8)
- DRUG TITRATION GUIDEDokument2 SeitenDRUG TITRATION GUIDEEgi Munandar100% (1)
- Handbook of Pain ManagementDokument730 SeitenHandbook of Pain Managementanon_990504998100% (6)
- Peripheral Nerve Injury Anatomical PDFDokument384 SeitenPeripheral Nerve Injury Anatomical PDFSharanjit Dhillon100% (2)
- ATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFDokument1.164 SeitenATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFjesussalvadorsuazaNoch keine Bewertungen
- Assessing Patients Preoperatively (A2 B2 C2 D2 E2 F2 G2Dokument40 SeitenAssessing Patients Preoperatively (A2 B2 C2 D2 E2 F2 G2marina_shawkyNoch keine Bewertungen
- Assessment Management of PainDokument104 SeitenAssessment Management of PainCharles B. LópezNoch keine Bewertungen
- Anesthesia Care PlanDokument2 SeitenAnesthesia Care PlanMedShare100% (10)
- Intravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Dokument5 SeitenIntravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821crsscribdNoch keine Bewertungen
- نسخة Lecture - PAIN Assessment & ManagementDokument52 Seitenنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Lab ValuesDokument6 SeitenLab ValuesdnllkzaNoch keine Bewertungen
- 282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFDokument859 Seiten282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFarief-024100% (2)
- Adjuvant Analgesics (2015) PDFDokument177 SeitenAdjuvant Analgesics (2015) PDFsatriomega100% (1)
- Ketamine For Opiate WithdrawalDokument3 SeitenKetamine For Opiate WithdrawalroboNoch keine Bewertungen
- Drugs and DosagesDokument30 SeitenDrugs and DosagesvanessaNoch keine Bewertungen
- Anaesthesia in Obese PatientsDokument72 SeitenAnaesthesia in Obese PatientsPraveen RamasamyNoch keine Bewertungen
- Intraoperative Fluid ManagementDokument23 SeitenIntraoperative Fluid ManagementMirela Marina BlajNoch keine Bewertungen
- 1495 2020 Anesthesiology Resident MDokument158 Seiten1495 2020 Anesthesiology Resident MPL NLNoch keine Bewertungen
- Bonicas Management of Pain 5th Edition PDFDokument6.053 SeitenBonicas Management of Pain 5th Edition PDFLuz Karinne Gonzalez Julio100% (5)
- Integrative Pain ManagementDokument18 SeitenIntegrative Pain ManagementSarah Coelho HoraNoch keine Bewertungen
- Regional Anesthesia Part 5Dokument7 SeitenRegional Anesthesia Part 5Dianne GalangNoch keine Bewertungen
- Anesthesiology Medical StudentsDokument38 SeitenAnesthesiology Medical StudentsJamesNoch keine Bewertungen
- DETAILED LESSON PLAN IN Health 9Dokument6 SeitenDETAILED LESSON PLAN IN Health 9shiramae91% (11)
- Anesthesia Consent FormDokument2 SeitenAnesthesia Consent Formbalab2311Noch keine Bewertungen
- Pain ManagementDokument175 SeitenPain ManagementGusni FitriNoch keine Bewertungen
- CPG Type 2 DM 6th EditionDokument284 SeitenCPG Type 2 DM 6th EditionAdriana AfiqahNoch keine Bewertungen
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDokument23 SeitenDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanNoch keine Bewertungen
- NSAIDDokument1 SeiteNSAIDShubhangiNoch keine Bewertungen
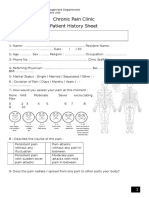
- Chronic Pain Clinic Patient History SheetDokument4 SeitenChronic Pain Clinic Patient History SheetBelal N. MahfouzNoch keine Bewertungen
- MCQ Anti AnxietyDokument2 SeitenMCQ Anti AnxietyMickey Brown89% (28)
- 4.73 (FCM) EBM - Critical Appraisal On Therapy and PreventionDokument6 Seiten4.73 (FCM) EBM - Critical Appraisal On Therapy and PreventionEver Mary Joy EscaleraNoch keine Bewertungen
- Anaesthesia For Thyroid SurgeryDokument19 SeitenAnaesthesia For Thyroid SurgeryPraveen Ramasamy0% (1)
- Pharmacology of Opioid AnalgesicsDokument64 SeitenPharmacology of Opioid AnalgesicsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- The Primary Care of Seizure Disorders: A Practical Guide to the Evaluation and Comprehensive Management of Seizure DisordersVon EverandThe Primary Care of Seizure Disorders: A Practical Guide to the Evaluation and Comprehensive Management of Seizure DisordersNoch keine Bewertungen
- Clinical Use of DexmedetomidineDokument29 SeitenClinical Use of DexmedetomidineAnil SathyadasNoch keine Bewertungen
- Acute Postoperative Pain Manila Relef.Dokument134 SeitenAcute Postoperative Pain Manila Relef.Muchtar Luthfi100% (1)
- 2022 Pharmacology s2t2 HeartfailureDokument6 Seiten2022 Pharmacology s2t2 Heartfailurejed larsen capulong gavinoNoch keine Bewertungen
- Pediatric Anesthesiology Review: Clinical Cases for Self-AssessmentVon EverandPediatric Anesthesiology Review: Clinical Cases for Self-AssessmentNoch keine Bewertungen
- Post Op Pain ManagementDokument42 SeitenPost Op Pain ManagementMuhammad Iqbal A GhaniNoch keine Bewertungen
- Pathogenesis of Peripheral Nerve DisorderDokument47 SeitenPathogenesis of Peripheral Nerve DisorderDanil Anugrah JayaNoch keine Bewertungen
- Adjuvant AnalgesicsDokument44 SeitenAdjuvant AnalgesicsZulfan EfendiNoch keine Bewertungen
- Atlas of Pain Medicine Procedures PDFDokument1.550 SeitenAtlas of Pain Medicine Procedures PDFDr_Zahid_Khan100% (5)
- Postoperative Management in AdultsDokument58 SeitenPostoperative Management in AdultsAjay KumarNoch keine Bewertungen
- Anesthesia Books Obstetric AnesthesiaDokument190 SeitenAnesthesia Books Obstetric AnesthesiaMarcus Menezes100% (1)
- Drugs Acting On The Endocrine SystemDokument90 SeitenDrugs Acting On The Endocrine SystemKATHERINE GRACE JOSENoch keine Bewertungen
- (20060519) Lower Extremity Peripheral Nerve BlockDokument30 Seiten(20060519) Lower Extremity Peripheral Nerve Blockdimas wicaksonoNoch keine Bewertungen
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: 6. General AnesthesiaDokument12 SeitenDr. Naitik D Trivedi & Dr. Upama N. Trivedi: 6. General AnesthesiaNaveen KumarNoch keine Bewertungen
- Veterinary Pharmacology and Toxicology MCQsDokument10 SeitenVeterinary Pharmacology and Toxicology MCQsSunilNoch keine Bewertungen
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDokument287 SeitenThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALINoch keine Bewertungen
- PEDIATRIC REGIONAL ANESTHESIA TECHNIQUESDokument66 SeitenPEDIATRIC REGIONAL ANESTHESIA TECHNIQUEStameem89Noch keine Bewertungen
- Anesthesiology Handbook Part 3Dokument6 SeitenAnesthesiology Handbook Part 3leo90_wyattNoch keine Bewertungen
- Year One of Practice Transition: The Necessary Guide to SuccessVon EverandYear One of Practice Transition: The Necessary Guide to SuccessJason E. PopeNoch keine Bewertungen
- Anesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaDokument3 SeitenAnesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaJhevilin RMNoch keine Bewertungen
- OB1 Lec - AnalgesiaDokument3 SeitenOB1 Lec - Analgesiaapi-3700579Noch keine Bewertungen
- Midazolam 5mg in 1ml Injection - UK ReferenceDokument11 SeitenMidazolam 5mg in 1ml Injection - UK ReferenceDilawar BakhtNoch keine Bewertungen
- ORIF Ankle Surgery RecoveryDokument2 SeitenORIF Ankle Surgery RecoverypatzieNoch keine Bewertungen
- LidocaineDokument11 SeitenLidocaineStanford AnesthesiaNoch keine Bewertungen
- Checklist For Anaesthetic Equipment 2012Dokument2 SeitenChecklist For Anaesthetic Equipment 2012that dude in duettesNoch keine Bewertungen
- Epidural AnalgesiaDokument15 SeitenEpidural AnalgesiaNikhil YadavNoch keine Bewertungen
- LOCAL ANESTHETICS MECHANISMDokument30 SeitenLOCAL ANESTHETICS MECHANISMCorry QyNoch keine Bewertungen
- Peripheral Arterial Occlusive DiseaseDokument4 SeitenPeripheral Arterial Occlusive Diseasekrisfred14100% (1)
- Generic (Brand) Name Use Considerations: Table of Selected Medications Used in Pain ManagementDokument4 SeitenGeneric (Brand) Name Use Considerations: Table of Selected Medications Used in Pain Managementrifal akbarNoch keine Bewertungen
- Travel Information To QatarDokument2 SeitenTravel Information To Qatarkaran patelNoch keine Bewertungen
- Coverage DocumentDokument2 SeitenCoverage Documentsushant24x7Noch keine Bewertungen
- CP 01708016Dokument11 SeitenCP 01708016telur_kudaNoch keine Bewertungen
- Prime Health Med. Svcs. Co. Laila Gomaa, MD. (PD PMC)Dokument10 SeitenPrime Health Med. Svcs. Co. Laila Gomaa, MD. (PD PMC)James LindonNoch keine Bewertungen
- Formulation and Evaluation of Voglibose Mouth Dissolving Tablets by Direct Compression MethodDokument5 SeitenFormulation and Evaluation of Voglibose Mouth Dissolving Tablets by Direct Compression Methodanto_pharma7784Noch keine Bewertungen
- 8 Common Charting Mistakes To Avoi1aDokument4 Seiten8 Common Charting Mistakes To Avoi1aEggy PascualNoch keine Bewertungen
- List of Controlled SubstancesDokument2 SeitenList of Controlled Substancesspiccolo12100% (1)
- 4Q2014EXCELDokument857 Seiten4Q2014EXCELyash143565Noch keine Bewertungen
- 07 26 17Dokument24 Seiten07 26 17WoodsNoch keine Bewertungen
- Paws and Claws Pet Care 101Dokument2 SeitenPaws and Claws Pet Care 101pawsandclawspetcareNoch keine Bewertungen
- Classification Revised For Lung Adenocarcinoma: Fighting Tuberculosis in SiberiaDokument24 SeitenClassification Revised For Lung Adenocarcinoma: Fighting Tuberculosis in SiberiaYantoNoch keine Bewertungen
- Handout On Prescription WritingDokument10 SeitenHandout On Prescription WritingAbdiNoch keine Bewertungen
- Guide to Raising Hospital ClaimsDokument1 SeiteGuide to Raising Hospital ClaimsBalaNoch keine Bewertungen
- Er-Drug StudyDokument41 SeitenEr-Drug Studyrc_lacampuinganyahooNoch keine Bewertungen
- ACAMYLOPHENINDokument21 SeitenACAMYLOPHENINDaniel Sandoval RodriguezNoch keine Bewertungen
- Debbie Carlson CVDokument5 SeitenDebbie Carlson CVdjayne407Noch keine Bewertungen
- IukulyulytDokument25 SeitenIukulyulytRizki D'biskaNoch keine Bewertungen
- Profilaksis MalariaDokument12 SeitenProfilaksis MalariaAlfian MuhajirNoch keine Bewertungen
- CYP450 Chart 5.2016Dokument8 SeitenCYP450 Chart 5.2016bl9nkverseNoch keine Bewertungen
- Buspar (Buspirone)Dokument1 SeiteBuspar (Buspirone)ENoch keine Bewertungen
- Sublingual DdsDokument20 SeitenSublingual DdsrandatagNoch keine Bewertungen
- Pharmaceutical Dosage Forms LaboratoryDokument11 SeitenPharmaceutical Dosage Forms LaboratoryLianneShin100% (1)