Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Dcfs Vitamink ProcedureDokument3 SeitenDcfs Vitamink ProcedurediscussNoch keine Bewertungen
- Academic Qualification DR Yam ROKADokument22 SeitenAcademic Qualification DR Yam ROKASafin RokaNoch keine Bewertungen
- Nelly Lim - Vs - CA and Juan SimDokument2 SeitenNelly Lim - Vs - CA and Juan SimOculus DecoremNoch keine Bewertungen
- Clinical Research Profesionals in IndiaDokument5 SeitenClinical Research Profesionals in Indiasng1Noch keine Bewertungen
- Occupations on SOL from July 2013Dokument5 SeitenOccupations on SOL from July 2013Bruce LeeNoch keine Bewertungen
- Guideline: Standards For Paediatric Intravenous Fluids: NSW Health (Second Edition)Dokument27 SeitenGuideline: Standards For Paediatric Intravenous Fluids: NSW Health (Second Edition)hartomas bumiharjoNoch keine Bewertungen
- ResumeDokument3 SeitenResumeapi-301877122Noch keine Bewertungen
- Ureteritis Cystica Radiologic-Pathologic Correlation Imaging Science TodayDokument7 SeitenUreteritis Cystica Radiologic-Pathologic Correlation Imaging Science TodayvdograNoch keine Bewertungen
- MG II S2-Hospital-2Dokument5 SeitenMG II S2-Hospital-2Iuliana RaduNoch keine Bewertungen
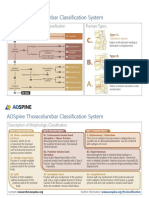
- AOSpine Thoracolumbar Classification System - Pocket CardDokument2 SeitenAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Case Study On :'œmarketing Strategies of Henry Ford of Heart Surgery - Narayana Health Care Also Known As Narayana Hrudayalaya, Leading India in World For Health Care'Dokument7 SeitenCase Study On :'œmarketing Strategies of Henry Ford of Heart Surgery - Narayana Health Care Also Known As Narayana Hrudayalaya, Leading India in World For Health Care'Editor IJTSRDNoch keine Bewertungen
- 12.4.18 Final Revised 12.4.18 Joint Letter To HHS DOJ DOE Uphold Definition of SexDokument8 Seiten12.4.18 Final Revised 12.4.18 Joint Letter To HHS DOJ DOE Uphold Definition of SexShane Vander HartNoch keine Bewertungen
- Jose Rizal's TravelsDokument45 SeitenJose Rizal's TravelsStephanie Ann Marie DueñasNoch keine Bewertungen
- Chapter 8, Part B - The Spinal Cord!Dokument9 SeitenChapter 8, Part B - The Spinal Cord!Putamen NongchaiNoch keine Bewertungen
- Advertising in Pharmaceutical Industry in IndiaDokument9 SeitenAdvertising in Pharmaceutical Industry in IndiaMegha SinghNoch keine Bewertungen
- Maple Syrup Urine DiseaseDokument2 SeitenMaple Syrup Urine Diseaseapi-240776501Noch keine Bewertungen
- Multi-Specialty Clinic Doctors GuideDokument3 SeitenMulti-Specialty Clinic Doctors GuideJMC Radiology Department0% (1)
- Magnetic Therapy in Eastern Europe A 30 Year ReviewDokument3 SeitenMagnetic Therapy in Eastern Europe A 30 Year ReviewMichael McDonnough100% (2)
- Myocardial Bridges Over Interventricular Branches of Coronary ArteriesDokument4 SeitenMyocardial Bridges Over Interventricular Branches of Coronary Arterieseditorjmst100% (1)
- Macon Beacon Calls Out Democrat Marshand Crisler For Playing The Race CardDokument2 SeitenMacon Beacon Calls Out Democrat Marshand Crisler For Playing The Race CardMajority In Mississippi blogNoch keine Bewertungen
- Challenges In Obstetric Anesthesia: 10 Key Issues for CRNAsDokument38 SeitenChallenges In Obstetric Anesthesia: 10 Key Issues for CRNAsPaulHerreraNoch keine Bewertungen
- LCP Técnica PreservaciónDokument6 SeitenLCP Técnica PreservacióndrjorgewtorresNoch keine Bewertungen
- GeneticsDokument56 SeitenGeneticsSri DevyNoch keine Bewertungen
- Ankylosing Spondylitis and HomoeopathyDokument12 SeitenAnkylosing Spondylitis and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNoch keine Bewertungen
- Lingual Orthodontics PDFDokument202 SeitenLingual Orthodontics PDFYan-HongLin100% (1)
- ASHA Module 7Dokument87 SeitenASHA Module 7Prabir Kumar ChatterjeeNoch keine Bewertungen
- Neutral Zone Approach For Rehabilitation of Severely Atrophic RidgeDokument5 SeitenNeutral Zone Approach For Rehabilitation of Severely Atrophic RidgeLynda M. NaranjoNoch keine Bewertungen
- Pulse Oximetry: Principles and Limitations: ReviewsDokument8 SeitenPulse Oximetry: Principles and Limitations: ReviewsDavid González GamboaNoch keine Bewertungen
- ProspectusDokument92 SeitenProspectusAnwer SaidNoch keine Bewertungen
- Operational Guidelines RBSKDokument43 SeitenOperational Guidelines RBSKanunad100% (1)